

Abstract
Pulmonary blastoma is an uncommon lung malignancy, usually presenting itself as a large chest mass causing pain, hemoptysis, cough and dyspnea; however, it is asymptomatic in up to 40% of patients. We present the case and suggestive images of a 37-year-old non-smoking lady with a monophasic pulmonary blastoma located in the lower lobe of the left lung who underwent a left posterolateral thoracotomy with lower lobectomy, hilar and mediastinal node dissection, followed by chemo and radiation therapy. After 36 mo, there is no disease progression and the patient is in good health, clinically stable and without significant chest pain.
Keywords: Pulmonary blastoma, Pleuropulmonary blastoma, Fetal adenocarcinoma, Lobectomy, Thoracotomy
Core tip: Pulmonary blastoma is a rare condition and diagnosis may be difficult to obtain. It is important to underline that the appropriate management of this unusual type of lesion can be achieved only by a multidisciplinary specialized team, able to plan the correct integrated strategy based on aggressive surgery and chemo-radiation therapy.
INTRODUCTION
Pulmonary blastoma is an unusual lung malignancy, constituting about 0.5% of all lung tumors[1-4]. Its histology resembles lung fetal tissue and can express both epithelial and mesenchymal features. Despite its assumed embryonal origin, the tumor predominantly affects adults[3]. The literature reports a limited number of cases classified as adult type pulmonary blastoma or child pleuropulmonary blastoma[5-8].
In adults, the neoplasm generally presents itself as a large and symptomatic mass causing cough, hemoptysis, fever and chest pain.
CASE REPORT
A 37-year-old non-smoking lady was admitted to the hospital with persistent chest pain, fever and hemoptysis. The chest X-ray showed a gross opacity in the left basal pulmonary field which was first suspected to be empyema complicating a pulmonary infection.
The computed tomography scan (CT scan) revealed the presence of a ten centimeter neoplasm located in the left basal hemithorax. Bronchoscopy showed neoplastic well vascularized vegetation occluding the left lower bronchus and histology through the biopsy permitted diagnosis of a monophasic pulmonary blastoma or the so called fetal adenocarcinoma. The immunohistochemistry obtained by fine needle aspiration biopsy of the lesion under CT scan guidance confirmed the rare lung tumor.
The stage was completed by a CT/positron emission tomography scan (CT/PET), showing an abnormal 18F-FDG uptake limited to the round mass with an elevated SUV of 13, a specific feature of this type of blastoma[1,9]. There was no evidence of other pathological localizations, confirming that the disease was enclosed in the left lung (Figure 1).
Figure 1.
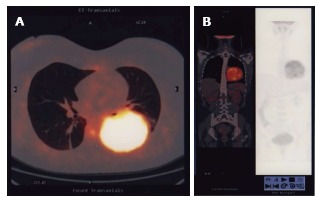
Computed tomography/positron emission tomography scan. A: CT-PET scan showing the large round mass in the left basal hemithorax; B: CT-PET scan showing a frontal vision of the mass inside the chest. CT-PET: Computed tomography/positron emission tomography.
Pre-operative work-up showed no contraindications so the patient underwent surgery. We performed a left posterolateral thoracotomy with lower lobectomy and hilar and mediastinal node dissection (Figure 2).
Figure 2.

A left posterolateral thoracotomy with lower lobectomy. A: Macroscopic vision of the large tumor infiltrating the left lower lobe; B: The cutting surface of the large tumor inside the left lower lobe.
The postoperative course was uneventful, the drains were removed three days after surgery and the patient was discharged three days later.
Definitive histology confirmed a pT3, pN2, M0 malignant monophasic pulmonary blastoma with only one metastatic mediastinal lymph node (Figure 3). The bronchial stump and the multiple specimens taken on the parietal and mediastinal pleura were negative.
Figure 3.

Monophasic pulmonary blastoma. A: Microscopic appearance of cytology in monophasic pulmonary blastoma; B: Monophasic pulmonary blastoma: Prevalence of epithelial on mesenchymal elements.
A month later the patient was evaluated by our interdisciplinary team and was considered eligible for adjuvant chemo and radiation therapy.
Follow-up at 6, 12, 24 and 36 mo revealed no disease progression on PET/CT scan, with a serum decrease of oncological markers. The patient is now in good health, clinically stable and without significant chest pain.
DISCUSSION
Pulmonary blastoma is a rare neoplasm with distinctive biological behavior[4]. It was described for the first time in 1952 by Barnard as an “embryoma” and in 1961 was regularly classified by Spencer who established that the tumor arises from pulmonary blastema as tumors developed from fetal tissues[5,10].
The neoplasm was divided by Koss et al[11] into three groups: biphasic pulmonary blastoma, monophasic pulmonary blastoma with prevalent epithelial expression, and pleuropulmonary blastoma with mesenchymal expression[2,5,10,11].
In adults, the tumor presents itself as a large chest mass causing pain, hemoptysis, cough and dyspnea; however, up to 40% of patients may be asymptomatic[4]. Diagnosis may be difficult to obtain because of the unusual pleomorphic histology but it has to be suspected when there is cytological evidence of heterogeneity with epithelial and mesenchymal malignant cells[12-14]. The radiological appearance consists of a well-delimited circle mass ranging in size from 1.5 to 13 cm in diameter.
Surgical excision is the treatment of choice[4,15]. The prognosis reported in the literature is generally poor, with limited survival within 2-3 years from diagnosis. The difference in survival rate depends on mediastinal node involvement and over the last ten years a better prognosis has been shown with preoperative neoadjuvant chemotherapy[14,16].
In a case of N2 disease, postoperative adjuvant radiation therapy and chemotherapy based on cisplatin and etoposide are considered the treatments of choice[14,17,18].
In conclusion, adult pulmonary blastoma is an unusual lung tumor presenting itself as a large invasive mass. Diagnosis, treatment and follow-up have to be planned by a multidisciplinary team. Integrated strategy based on aggressive surgery and chemo-radiation therapy may be the best choice for a successful treatment.
COMMENTS
Case characteristics
A 37-year-old non-smoking lady with persistent chest pain, fever and hemoptysis.
Clinical diagnosis
A ten centimeter neoplasm located in the left basal hemithorax.
Differential diagnosis
Empyema complicating a pulmonary infection.
Imaging diagnosis
A well-delimited circle mass ranging in size from 1.5 to 13 cm in diameter.
Pathological diagnosis
pT3, pN2, M0 monophasic pulmonary blastoma with one metastatic mediastinal lymph node.
Treatment
Left posterolateral thoracotomy with lower lobectomy and hilar and mediastinal node dissection followed by chemo and radiation therapy.
Related reports
The rare presentation of pulmonary blastoma can make obtaining a diagnosis difficult, so a meticulous evaluation by a multidisciplinary team is mandatory in suspected cases.
Experience and lessons
Pulmonary blastoma is a rare condition that has to be managed by a multidisciplinary team to plan the correct integrated strategy based on aggressive surgery and chemo-radiation therapy.
Peer review
This is a report of a rare case of a malignant lung tumor. The presentation is simple but adequate.
Footnotes
P- Reviewer: Andersen PE, Pereira-Vega A, Wang HY S- Editor: Song XX L- Editor: Roemmele A E- Editor: Lu YJ
References
- 1.Keu KV, Berry GJ, Quon A. Classic biphasic pulmonary blastoma demonstrated by 18F-FDG PET/CT. Clin Nucl Med. 2014;39:346–348. doi: 10.1097/RLU.0b013e31828e987c. [DOI] [PubMed] [Google Scholar]
- 2.Daghfous H, Belloumi N, Braham E, Ben Saad S, El Bay R, El Mezni F, Tritar F. [Case report of pulmonary biphasic tumor with unusual follow-up.] Rev Pneumol Clin. 2014 doi: 10.1016/j.pneumo.2014.01.001. [DOI] [PubMed] [Google Scholar]
- 3.Wang YX, Zhang J, Chu XY, Liu Y, Li F, Wang ZB, Wei LX. Diagnosis and multi-modality treatment of adult pulmonary plastoma: Analysis of 18 cases and review of literature. Asian Pac J Trop Med. 2014;7:164–168. doi: 10.1016/S1995-7645(14)60015-8. [DOI] [PubMed] [Google Scholar]
- 4.Dixit R, Joshi N, Dave L. Biphasic pulmonary blastoma: An unusual presentation with chest wall, rib, and pleural involvement. Lung India. 2014;31:87–89. doi: 10.4103/0970-2113.126002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chen S, Wang S, Gao J, Zhang S. [Pleuropulmonary blastoma: a clinicopathological analysis] Zhongguo Feiai Zazhi. 2010;13:550–553. doi: 10.3779/j.issn.1009-3419.2010.05.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hill DA, Jarzembowski JA, Priest JR, Williams G, Schoettler P, Dehner LP. Type I pleuropulmonary blastoma: pathology and biology study of 51 cases from the international pleuropulmonary blastoma registry. Am J Surg Pathol. 2008;32:282–295. doi: 10.1097/PAS.0b013e3181484165. [DOI] [PubMed] [Google Scholar]
- 7.Dishop MK, Kuruvilla S. Primary and metastatic lung tumors in the pediatric population: a review and 25-year experience at a large children’s hospital. Arch Pathol Lab Med. 2008;132:1079–1103. doi: 10.5858/2008-132-1079-PAMLTI. [DOI] [PubMed] [Google Scholar]
- 8.Jethava A, Dasanu CA. Adult biphasic pulmonary blastoma. Conn Med. 2013;77:19–22. [PubMed] [Google Scholar]
- 9.Sonoda LI, Wagner T, Sanghera B, Wong WL. 18F-FDG PET/CT appearances of adult pulmonary blastoma. Clin Nucl Med. 2013;38:737–738. doi: 10.1097/RLU.0b013e3182995e2d. [DOI] [PubMed] [Google Scholar]
- 10.Zagar TM, Blackwell S, Crawford J, D’Amico T, Christensen JD, Sporn TA, Kelsey CR. Preoperative radiation therapy and chemotherapy for pulmonary blastoma: a case report. J Thorac Oncol. 2010;5:282–283. doi: 10.1097/JTO.0b013e3181c420e1. [DOI] [PubMed] [Google Scholar]
- 11.Koss MN, Hochholzer L, O’Leary T. Pulmonary blastomas. Cancer. 1991;67:2368–2381. doi: 10.1002/1097-0142(19910501)67:9<2368::aid-cncr2820670926>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 12.Wang J, Sun H, Bai R, Liu H, Yu T. Pulmonary blastoma with endobronchial growth. J Thorac Oncol. 2009;4:543–544. doi: 10.1097/JTO.0b013e31819c8646. [DOI] [PubMed] [Google Scholar]
- 13.He W, Jiang G, Xie B, Liu M. Radical resection of a pulmonary blastoma involving the pulmonary artery. Eur J Cardiothorac Surg. 2008;34:695–696. doi: 10.1016/j.ejcts.2008.05.020. [DOI] [PubMed] [Google Scholar]
- 14.Iwata T, Nishiyama N, Inoue K, Kawata Y, Izumi N, Tsukioka T, Shinkawa K, Suehiro S. Biphasic pulmonary blastoma: report of a case. Ann Thorac Cardiovasc Surg. 2007;13:40–43. [PubMed] [Google Scholar]
- 15.Mistry JH, Pawar SB, Mehta H, Popov AF, Mohite PN. Primary pulmonary blastoma of monophasic variety--diagnosis and management. J Cardiothorac Surg. 2013;8:144. doi: 10.1186/1749-8090-8-144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Liman ST, Altinok T, Topcu S, Tastepe AI, Uzar A, Demircan S, Demirag F. Survival of biphasic pulmonary blastoma. Respir Med. 2006;100:1174–1179. doi: 10.1016/j.rmed.2005.10.026. [DOI] [PubMed] [Google Scholar]
- 17.Schulze SM, Sbayi S, Costic JT, Moser RL. A rare case of classic biphasic pulmonary blastoma. Am Surg. 2005;71:1078–1081. [PubMed] [Google Scholar]
- 18.Walker RI, Suvarna K, Matthews S. Case report: pulmonary blastoma: presentation of two atypical cases and review of the literature. Br J Radiol. 2005;78:437–440. doi: 10.1259/bjr/45172814. [DOI] [PubMed] [Google Scholar]