

Abstract
Background:
Congenital heart disease (CHD) is a major health problem and its prevalence is different around the world. The aim of study was determination of the epidemiological aspects of CHD in central and southern district of Iran.
Materials and Methods:
In this descriptive and analytical study, 3714 medical records were evaluated from March 21, 2001 to December 18, 2011. Medical records of inpatients from angiography and outpatients in the Heart Clinic of Afshar hospital (a referral hospital in center and south of Iran) were the source of information. Types of CHD and demographic data including age, sex and residential location are collected. The data were analyzed by SPSS (version 17) software. Chi-square and Fisher's exact tests were used to compare variables between groups.
Results:
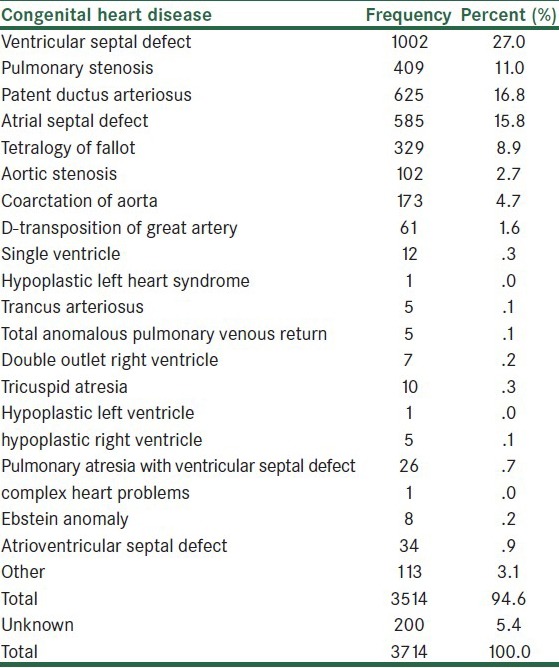
At the study, the mean age of the patients at diagnosis time was 8.8 ± 11.6 year (at the range of one day to 76 years with median of 4 years). The percentage of females and males was 54.2 (n: 2014) and 43.8 (n: 1627), respectively. The chi-square test showed that there was significant difference in frequency of CHDs between females and males (P value < 0.0001). Ventricular septal defect (VSD) was found to be the most frequent of CHDs (27%). Patent ductus arteriosus (PDA) (16.8%), atrial septal defect (ASD) (15.8%), pulmonary stenosis (PS) (11%) and Tetralogy of Fallot (TOF) (8.9%) were more prevalent in CHDs after VSD.
Conclusions:
The frequency of CHDs in female was more than male and VSD, PDA, ASD, PS, and TOF were most common in CHDs, respectively.
Keywords: Congenital heart disease, epidemiological aspect, frequency
INTRODUCTION
Congenital heart disease (CHD) is one of the most common congenital diseases in newborns and cause of death in 1% of life births.[1] CHD is a socio-economic problem, because the cost of medical treatments for parents and governments is high. Prevalence of CHD has been reported to be different around the world. An epidemiological study has shown that the prevalence of CHD is 4.6 to 12.2 per 1000 live births.[2] Another study has shown that the range of CHD is 7.93 to 17.51 per 1000 live births in Iran.[3] The prevalence of CHDs in Egypt (2000) and Central Australia (2004) was 1.01% and 17.5%, respectively.[4,5] However, pattern of CHDs is different in various geographic locations.[4] The majority (85% of all) of CHDs are ventricular septal defect (VSD), atrial septal defect (ASD), Tetralogy of Fallot (TOF), patent ductus arteriosus (PDA), pulmonary stenosis (PS), aortic stenosis (AS), coarctation of aorta (COA) and atrioventricular septal defect (AVSD) which accounts for CHDs. The minority (15%) of CHDs are persistent truncus arteriosus (PTA), tricuspid atresia (TA), total anomalous pulmonary venous connection (TAPVC), hypoplastic left heart syndrome (HLHS), double outlet right ventricle (DORV), single ventricle (SV), Ebstein anomaly (EA) and dextrocardia.[6] In Iran few studies on prevalence of CHDs were done, therefore we are going to report the epidemiological aspects of CHDs in central and southern district of Iran form March 21, 2001 to December 18, 2011.
MATERIALS AND METHODS
In this descriptive and analytical study, 3714 medical records were evaluated from March 21, 2001 to December 18, 2011. The source of data was medical records of admitted inpatients at angiography ward and outpatients in the Heart Clinic of Afshar Hospital (a referral hospital in center and south of Iran for CHDs management). This hospital admit majority of children with CHDs from Province of Yazd and patients referred form other hospitals in southern district of Iran. Demographic data including age, sex, residential location and type of CHDs are collected. Residential location of the patient was divided into two groups, central district was the province of Yazd and southern provinces included Fars, Kerman, Hormozgan, Sistan and Bluchestan. The different types of CHDs considered for the study were VSD, ASD, PDA, PS, TOF, AS, COA, SV, D-transposition of great artery (D-TGA), HLHS, trancus arteriosus, TAPVC, DORV, TA, hypoplastic left ventricle, hypoplastic right ventricle, pulmonary atresia with ventricular septal defect (PA-VSD), complex heart problems, EA and AVSD. The data were analyzed by SPSS (version 17) software. Chi-square test and Fisher's exact test were used to compare sex and age between groups.
RESULTS
In this investigation 3714 patients and their medical records were included. The mean age of the patients at diagnosis time was 8.8 ± 11.6 year (at the range of 1 day to 76 year). Table 1 showed that the mean age of the patients according to the types of CHDs.
Table 1.
Distribution of mean age in patients with congenital heart disease
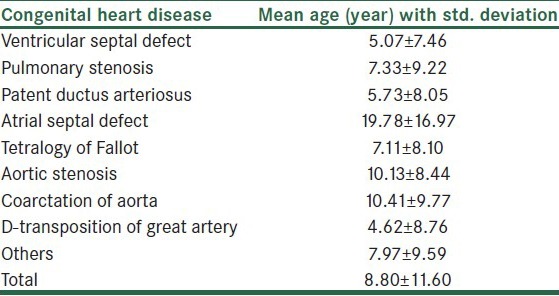
Others: SV, HLHS, trancus arteriosus, total anomalous pulmonary venous return (TAPVR), DORV, TA, hypoplastic left ventricle, hypoplastic right ventricle, PA-VSD, complex heart problems, EA, single atrium and dextrocardia.
The percentage of females and males was 54.2 (n: 2014) and 43.8 (n: 1627), respectively. The sex of 2% (n: 73) of patients in the medical records was unknown [Table 1].
VSD was found the most frequent of CHDs. Table 2 depicted the others.
Table 2.
Frequency and percentage of congenital heart disease
CHDs was more frequent in female and the chi-square test showed that there was significant difference in CHDs between males and females (P value < 0.0001). Also, the study disclosed that there were significant differences in PDA (P value < 0.0001), ASD (P value < 0.0001), TOF (P value < 0.001), AS (P value < 0.004), COA (P value < 0.0001) and D-TGA (P value < 0.0001) between males and females [Table 3].
Table 3.
Frequency of congenital heart diseases based on sex

VSD, PS, PDA, ASD, TOF, AS, COA, D-TGA.
Others: SV, HLHS, trancus arteriosus, TAPVC, DORV, TA, hypoplastic left ventricle, hypoplastic right ventricle, PA-VSD, complex heart problems, EA, single atrium and dextrocardia.
DISCUSSION
Our study showed that VSD was the most frequent (27%) of CHDs. Smitha et al. reported that VSD had 31.82% (in the year 2000), 38.19% (2001), 38.06% (2002), 22.88% (2003) and 26.37% (2004) of prevalence among the all of CHDs in Mysore hospitals. Also, the frequency of VSD in Saudi Arabia (2001) was 39.5%, New Dehli (2001) 46%, Oman[7] and Egypt (2000) 24.9% and 35.3% respectively, Japan (1990) 60%, Qatar (1997) 40.65 and USA (1990) 32.1% (6). Other studies showed these similarities.[8,9,10,11,12,13,14,15,16] In the study the mean age of VSD was 5.07±7.46. About 85% to 90% of VSDs close spontaneously by 1 year of age. So, the incidence of VSDs at first year of age is higher than other stages of life.[17,18,19] The other more frequent of CHDs in the study were PDA (16.8%), ASD (15.8%), PS (11%) and TOF (8.9%). Also, other studies reported that ASD, PDA, PS and TOF are more frequent after VSD.[2,9,13,16] PDA is another common CHD, incidence of which is higher in preterm than term infants. So, at the period of time that we have large numbers of preterm, the incidence of PDA will inflated.[20] The third common CHD in the study was ASD 15.8%. Because ASDs are usually asymptomatic, the incidence of these CHDs at the birth time is lower than adult life. ASD in which infants have a patent foramen ovale with a tiny left-to-right shunt will increase the incidence of it.[21] The mean age of the patients at diagnosis time was 8.8 ± 11.6 years (the rage was one day to 76 years). In Sani's study the rage of CHDs was 9 days to 35 years.[16] In Marelli's study and et al. demonstrated that in 1985 and 2000, the mean age of all patients with severe CHDs was 11 and 17 years, respectively. In 2000, the mean age of patients with CHDs was 40 years.[22] However, the range and the mean age of CHDs will vary according to the time of diagnosis in different studies.[16,22] The percentage of females and males was 54.2 (n: 2014) and 43.8 (n: 1627) respectively and we found that there was significant difference in prevalence of CHDs between males and females (P value < 0.0001). Also, Begic et al. in their study showed that 54.3% of CHDs were boys and 45.7% were girls.[2] Marelli et al. reported that in 2000, 57% of adult with CHDs were female and there was significantly different in prevalence of all CHDs in adults between females and males (4.55 per 1000 females versus 3.61 per 1000 males; P value < 0.0001). Also, in population of children with CHDs 52% of them were females.[22] Other studies showed that the prevalence of CHDs in female is more than male.[8,13] But, Nikyar et al. recorded that the risk of CHDs in males is (1.35 times) more than in females (P value > 0.05) in northern district of Iran.[1] In the study the percentage of females with VSD, PDA (P value < 0.0001), ASD (P value < 0.0001) and PS was higher than females. Also, another research showed that ASD, VSD, PDA and AVCD in females were higher than males. Research data in 1985 were similar with data in 2000.[22] In our study we found that the number of male patients with COA was higher than females and there was significant difference in COA (P value < 0.0001) between male and female. In 2000, Marelli et al. also disclosed that transposition complexes and coarctation were more common in male adults (22). However, types of CHDs are different around the world and some researchers have reported different data for prevalence of CHDs.
SUMMARY
The study findings indicate that the frequency of CHDs in central and southern district of Iran is a major health problem. CHDs were more common in females than males at all. In the details the frequency of females other than males was more in VSD, PS, PDA and ASD. But, the frequency of males other than females was more in TOF, AS, COA and D-TGA. VSD was the most frequent of CHDs.
Also, PDA, ASD, PS and TOF were frequent after VSD.
ACKNOWLEDGEMENT
We would like to thank the Yazd Cardiovascular Research Center because of supporting the study by fund.
Footnotes
Source of Support: Yazd Cardiovascular Research Center.
Conflict of Interest: None declared.
REFERENCES
- 1.Nikyar B, Sedehi M, Mirfazeli A, Qorbani M, Golalipour MJ. Prevalence and pattern of congenital heart disease among neonates in Gorgan, Northern Iran (2007-2008) Iran J Pediatr. 2011;21:307–12. [PMC free article] [PubMed] [Google Scholar]
- 2.Begicć H, Tahirovicć H, Mesihovicć-Dinarevicć S, Ferkovicć V, Aticć N, Latifagicć A. Epidemiological and clinical aspects of congenital heart disease in children in Tuzla Canton, Bosnia-Herzegovina. Eur J Pediatr. 2003;162:191–3. doi: 10.1007/s00431-002-1125-3. [DOI] [PubMed] [Google Scholar]
- 3.Rahim F, Ebadi A, Saki G, Remazani A. Prevalence of congenital heart disease in Iran: A clinical study. J Med Sci. 2008;8:547–52. [Google Scholar]
- 4.Bolisetty S, Daftary A, Ewald D, Knight B, Wheaton G. Congenital heart defects in Central Australia. Med J Aust. 2004;180:614–7. doi: 10.5694/j.1326-5377.2004.tb06122.x. [DOI] [PubMed] [Google Scholar]
- 5.Bassili A, Mokhtar SA, Dabous NI, Zaher SR, Mokhtar MM, Zaki A. Congenital heart disease among school children in Alexandria, Egypt: An overview on prevalence and relative frequencies. J Trop Pediatr. 2000;46:357–62. doi: 10.1093/tropej/46.6.357. [DOI] [PubMed] [Google Scholar]
- 6.Smitha R, Karat SC, Narayanappa D, Krishnamurthy B, Prasanth SN, Ramachandra NB. Prevalence of congenital heart diseases in Mysore. Indian J Hum Genet. 2006;12:11–6. [Google Scholar]
- 7.Subramanyan R, Joy J, Venugopalan P, Sapru A, al Khusaiby S. Incidence and spectrum of congenital heart disease in Oman. Ann Trop Paediatr. 2000;20:337–41. doi: 10.1080/02724936.2000.11748155. [DOI] [PubMed] [Google Scholar]
- 8.Alabdulgader AA. Congenital heart disease in 740 subjects: Epidemiological aspects. Ann Trop Paediatr. 2001;21:111–8. [PubMed] [Google Scholar]
- 9.Alnajjar AA, Morsy MF, Almuzainy IS, Sheikh AA. Pediatric heart diseases in Madina, Saudi Arabia. Current status and future expectations. Saudi Med J. 2009;30:1186–91. [PubMed] [Google Scholar]
- 10.Bosi G, Scorrano M, Tosato G, Forini E, Chakrokh R. The Italian multicentric study on epidemiology of congenital heart disease: First step of the analysis. Working Party of the Italian Society of Pediatric Cardiology. Cardiol Young. 1999;9:291–9. doi: 10.1017/s1047951100004960. [DOI] [PubMed] [Google Scholar]
- 11.Grech V, Gatt M. Syndromes and malformations associated with congenital heart disease in a population-based study. Int J Cardiol. 1999;68:151–6. doi: 10.1016/s0167-5273(98)00354-4. [DOI] [PubMed] [Google Scholar]
- 12.Mackie AS, Ionescu-Ittu R, Therrien J, Pilote L, Abrahamowicz M, Marelli AJ. Children and adults with congenital heart disease lost to follow-up: Who and when? Circulation. 2009;120:302–9. doi: 10.1161/CIRCULATIONAHA.108.839464. [DOI] [PubMed] [Google Scholar]
- 13.Mocumbi AO, Lameira E, Yaksh A, Paul L, Ferreira MB, Sidi D. Challenges on the management of congenital heart disease in developing countries. Int J Cardiol. 2011;148:285–8. doi: 10.1016/j.ijcard.2009.11.006. [DOI] [PubMed] [Google Scholar]
- 14.Pradat P. Noncardiac malformations at major congenital heart defects. Pediatr Cardiol. 1997;18:11–8. doi: 10.1007/s002469900101. [DOI] [PubMed] [Google Scholar]
- 15.Robida A, Folger GM, Hajar HA. Incidence of congenital heart disease in Qatari children. Int J Cardiol. 1997;60:19–22. doi: 10.1016/s0167-5273(97)00067-3. [DOI] [PubMed] [Google Scholar]
- 16.Sani MU, Mukhtar-Yola M, Karaye KM. Spectrum of congenital heart disease in a tropical environment: An echocardiography study. J Natl Med Assoc. 2007;99:665–9. [PMC free article] [PubMed] [Google Scholar]
- 17.Hiraishi S, Agata Y, Nowatari M, Oguchi K, Misawa H, Hirota H, et al. Incidence and natural course of trabecular ventricular septal defect: Two-dimensional echocardiography and color Doppler flow imaging study. J Pediatr. 1992;120:409–15. doi: 10.1016/s0022-3476(05)80906-0. [DOI] [PubMed] [Google Scholar]
- 18.Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–900. doi: 10.1016/s0735-1097(02)01886-7. [DOI] [PubMed] [Google Scholar]
- 19.Roguin N, Du ZD, Barak M, Nasser N, Hershkowitz S, Milgram E. High prevalence of muscular ventricular septal defect in neonates. J Am Coll Cardiol. 1995;26:1545–8. doi: 10.1016/0735-1097(95)00358-4. [DOI] [PubMed] [Google Scholar]
- 20.Anderson CE, Edmonds LD, Erickson JD. Patent ductus arteriosus and ventricular septal defect: Trends in reported frequency. Am J Epidemiol. 1978;107:281–9. doi: 10.1093/oxfordjournals.aje.a112543. [DOI] [PubMed] [Google Scholar]
- 21.Ooshima A, Fukushige J, Ueda K. Incidence of structural cardiac disorders in neonates: An evaluation by color Doppler echocardiography and the results of a 1-year follow-up. Cardiology. 1995;86:402–6. doi: 10.1159/000176910. [DOI] [PubMed] [Google Scholar]
- 22.Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L. Congenital heart disease in the general population: Changing prevalence and age distribution. Circulation. 2007;115:163–72. doi: 10.1161/CIRCULATIONAHA.106.627224. [DOI] [PubMed] [Google Scholar]