

Abstract
Background
Little empirical data exist to identify the reasons for underreporting in the US Bureau of Labor Statistics (BLS) non-fatal occupational injury and illness data.
Methods
We interviewed occupational injury and illness record keepers from Washington State establishments that participated in the 2008 BLS Survey of Occupational Injuries and Illnesses (SOII). Qualitative and quantitative methods were used to explore recordkeeping and business practices that may explain SOII's incomplete case capture compared with WC claims data.
Results
Most participants (90%) did not comply with OSHA recordkeeping regulations. Other factors including using workplace injury data to evaluate supervisors' or SOII respondent's job performance, recording injuries for a worksite that operates multiple shifts, and failing to follow SOII instructions were more common among establishments with unreported WC claims.
Conclusion
Business practices that incentivize low injury rates, disorganized recordkeeping, and limited communication between BLS and survey respondents are barriers to accurate employer reports of work-related injuries and illnesses. Am. J. Ind. Med. 57:1133–1143, 2014. © 2014 The Authors. American Journal of Industrial Medicine published by Wiley Periodicals, Inc.
Keywords: workplace injuries and illnesses, surveillance, injury underreporting, Bureau of Labor Statistics, Survey of Occupational Injuries and Illnesses, OSHA recordkeeping, workers' compensation data
INTRODUCTION
The US Bureau of Labor Statistics (BLS) provides annual estimates of non-fatal occupational injuries and illnesses. The national and state estimates are based on approximately 230,000 employer reports of OSHA recordable cases collected through the Survey of Occupational Injuries and Illnesses (SOII) [US Department of Labor, 2012]. According to the BLS, SOII is the nation's largest occupational injury and illness surveillance system.
Increasingly, evidence suggests that the BLS fails to accurately estimate the number of occupational injuries and illnesses through the annual survey of employers, although, estimates of the BLS undercount vary widely [Leigh et al., 2004; Rosenman et al., 2006; Boden and Ozonoff, 2008; Oleinick and Zaidman, 2010]. In response to the most recent concerns of unreported injuries and illnesses on employer OSHA logs and in the SOII, the federal government undertook efforts to better understand employer recordkeeping. The US Government Accountability Office evaluated OSHA's audit procedures used to verify the workplace injury and illness data collected through OSHA's Data Initiative [US Government Accountability Office, 2009]; OSHA initiated a national emphasis program for recordkeeping [US Department of Labor, 2009]; and the BLS undertook its own studies and also funded extramural research projects to examine the nature of the observed undercount [Ruser, 2010].
The BLS intramural studies identified the SOII methodology as a source of incomplete case capture. Collecting employer reports of injuries and illnesses within a few months following the survey year hinders the reporting of certain cases including illnesses with long latencies, injuries that worsen over time, those that are difficult to attribute to work, and injuries reported after the survey year [Ruser, 2008; Nestoriak and Pierce, 2009].
Employer recordkeeping practices may be another source of SOII's incomplete case capture. In this study, we explored the relationships between employers' incomplete case reporting in SOII and compliance with OSHA recordkeeping requirements and company uses of injury and illness data.
METHODS
We conducted semi-structured interviews with workplace injury and illness record keepers from Washington State establishments that had participated in the 2008 SOII. To compare responses among establishments that reported to SOII all survey eligible WC claims (“complete reporters”) to those with unreported WC claims (“under-reporters”), we matched 2008 BLS SOII data to Washington WC claims data.
Data Sources
The BLS administers the SOII in partnership with participating states to estimate the incidence of work-related injuries and illnesses [US Department of Labor, 2012]. The SOII includes both public and private sector employment except for federal employees, private household workers, farms with fewer than 11 employees, and the self-employed.
Each year, the BLS selects a sample of establishments to participate in the survey. Establishments are drawn from unemployment insurance (UI) data, contacted prior to the survey year, and instructed to record all injuries and illnesses that occur during the survey year in accordance with OSHA record keeping regulations.1After the survey year has ended, establishments are required to provide the BLS with three types of data: (1) general establishment information including the average number of employees for the year; (2) summary OSHA injury and illness data like the total number of cases with days away from work; and (3) detailed case information on injuries and illnesses that occurred in the survey year and resulted in one or more calendar days away from work (DAFW) beyond the day of injury. The case information provided for DAFW injuries includes worker identifiers that allow for linking to other data sources.
Washington State SOII data for the 2008 survey year were obtained through a cooperative agreement between the BLS and the Washington State Department of Labor and Industries (L&I).
L&I regulates WC insurance for all non-federal employers operating in Washington State covered by the state's industrial insurance laws [Revised Code of Washington, 1972]. In addition, L&I administers the Washington state fund (SF) workers' compensation insurance program, which is the sole workers' compensation insurance provider for all employers in the state except those covered by an alternate workers' compensation system (e.g., Longshore and Harbor Workers' Compensation Act, Federal Employees' Compensation Act) or those who self-insure.
When a worker is entitled to compensation under the Washington Industrial Insurance laws, the worker files the application together with certification by the attending physician [Revised Code of Washington, 2005].2The claim is submitted to L&I who then informs the employer that a claim has been opened. The waiting period for wage replacement compensation is three calendar days following the day of injury; if the attending health care provider recommends work restrictions resulting in time loss from work beyond the 3-day waiting period, the claimant becomes eligible for wage replacement benefits.
SOII-WC Record Linkage
All filed WC claims (rejected, medical aid only, and claims eligible for indemnity payments for lost wages) with an injury date between October 31, 2007 and March 1, 2009 were eligible for linking to SOII cases reported for the 2008 survey year. Although, not all WC claims meet the SOII case reporting criteria, no exclusions were made prior to linking to allow for possible differences in classification across the two systems. SOII cases were linked to WC claims using worker name, sex, date of birth or age, date of injury, employer name, employer address, and a Washington State-assigned Uniform Business Identifier (UBI), which can be used to identify an employer across state data systems, including the UI and WC systems.
SOII sampled establishments were linked to WC businesses through the UBI, employer name and address, and, when available, a case-claim match. When the BLS sampled employment was less than the employer's entire workforce, the unit description from the SOII data was evaluated against the business location and accident location listed for the claim to determine whether the claimant was included in the workforce sampled for the SOII.
Data linkage was performed using the probabilistic linking software LinkPlus [US Department of Health and Human Services, 2007]. The program scores each potential pair to indicate the degree of similarity between the two records. Pairs with lower scores, reflecting a poorer match, were reviewed independently by two research staff to determine true links. Disagreements between the two researchers were settled by a third reviewer.
Having identified unlinked WC claims among SOII sampled establishments, we further limited claims to include only those that most likely met the SOII case reporting criteria, that is, an OSHA DAFW case. SOII case reporting criteria were approximated from the type of indemnity payments awarded (used to indicate work absence) and the dates associated with the claim (used to indicate whether the initial work absence occurred during the survey period or after). Unmatched WC claims eligible for time loss payments, total permanent disability, and those “kept on salary”3were considered SOII-eligible when the WC dates for injury, first medical treatment, claim establishment, disability, and initial benefit payment did not occur after the study period. Claims limited to payments for medical care, claims awarded benefits for loss of earning power (temporary partial disability), and rejected claims were assumed not to have met OSHA criteria as DAFW case. This assumption likely resulted in a conservative estimate of unlinked WC claims. Medical aid claims include injuries that resulted in some missed work; however, we could not distinguish injuries with work absence less than the waiting period for wage replacement benefits from those with no work absence. Among establishments instructed by BLS to report on a sub-sample of cases based on injury dates, unmatched claims with injury dates outside the requested timeframe were excluded from the group of claims considered SOII eligible. An overview of the record linkage process and identification of unreported WC claims is provided in Figure 1.
Figure 1.
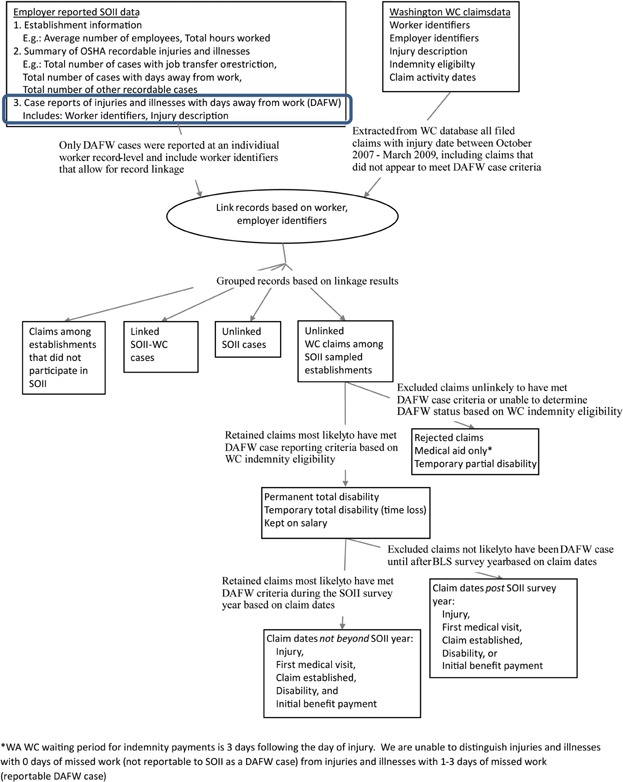
Overview of SOII-Washington Workers' compensation record linkage and identification of unreported SOII-eligible WC claims.
Selection of Interview Participants
Establishments were selected from the 2008 Washington BLS SOII respondents and stratified by four characteristics to provide a diverse pool of recordkeeping experiences: establishment size; industry; number of establishments operated by employer; and completeness of occupational injury and illness reporting. Based on the SOII data, establishments were classified as small (1–49 employees) or large (50 or more employees), fixed site industries or non-fixed (non-permanent worksite locations identified from four digit NAICS codes, primarily within construction and transportation), and the sole establishment operated by an employer or one of multiple establishments. The SOII-WC record linkage results were used to classify establishments as complete reporters or under-reporters. Although, the record linkage process identified both SOII cases not identified in WC and WC claims not reported in SOII, in this paper we focus on the reporting of WC claims and leave the unlinked SOII cases for a later discussion since the reasons for unreported WC claims likely differ from the reasons for unreported SOII cases.
Our preference was to interview the individual listed as the 2008 SOII contact. When that individual was no longer employed by the firm, we interviewed the person currently responsible for injury recordkeeping. Interviews were conducted by trained research staff at the respondent's place of business, lasted approximately 1 hr, and were recorded with the participant's consent. The semi-structured interviews covered a range of topics including: company injury and illness reporting process; compliance with the OSHA recordkeeping regulations; and company uses of injury and illness data. All interviews took place between April 2011 and December 2011.
Analysis of Data
Two research staff independently coded responses to open-ended questions. When disagreements in codes occurred, responses were discussed until consensus was reached. Given the exploratory nature of the study, descriptive statistics were used to summarize the data and examine relationships between select establishment characteristics and incomplete injury and illness reporting. Associations between select categorical variables were assessed using Pearson's chi-squared and Fisher's exact tests.
The research study was approved by the Washington State Institutional Review Board. The process of informed consent involved obtaining written consent from each study participant prior to conducting the interview. Participants were informed that their responses were confidential and would not be shared with the state OSHA program.
RESULTS
We contacted 271 Washington establishments that participated in the 2008 BLS SOII. Forty-seven percent (127 establishments) agreed to be interviewed, although 14 scheduled interviews were cancelled by the establishment, resulting in 113 completed interviews. Compared with interviewed establishments, a greater portion of contacted establishments that did not participate were small, in the construction or retail trade industries, and, in the 2008 SOII, reported zero injuries or illnesses resulting in one or more day of missed work (Table1). Three establishments were excluded from the analysis because someone other than the interviewee completed the OSHA recordkeeping forms and the respondent was unable to speak to the establishment's OSHA recordkeeping practices. Among the remaining 110 interviews, 80% of respondents had completed the 2008 SOII for the establishment.
I.
Select Characteristics of Washington Establishments Contacted for Interview (n = 271)
| Completed interviews* | Refusals** | |||
|---|---|---|---|---|
| Total | 113 | 100% | 158 | 100% |
| Establishment size | ||||
| 1–10 Emp | 3 | 3% | 26 | 16% |
| 11–24 Emp | 15 | 13% | 29 | 18% |
| 25–49 Emp | 30 | 27% | 35 | 22% |
| 50–99 Emp | 27 | 24% | 34 | 22% |
| 100–999 Emp | 29 | 26% | 32 | 20% |
| 1,000+ Emp | 9 | 8% | 2 | 1% |
| Industry | ||||
| Manufacturing | 27 | 24% | 28 | 18% |
| Construction | 16 | 14% | 38 | 24% |
| Agriculture, forestry, fishing, and hunting | 14 | 12% | 11 | 7% |
| Transportation, warehousing, and utilities | 13 | 12% | 12 | 8% |
| Health care and social assistance | 10 | 9% | 14 | 9% |
| Retail trade | 8 | 7% | 18 | 11% |
| Wholesale trade | 6 | 5% | 8 | 5% |
| Public administration | 5 | 4% | 2 | 1% |
| Educational services | 3 | 3% | 5 | 3% |
| Leisure and hospitality | 3 | 3% | 5 | 3% |
| Admin & support, waste mgmt & remediation srvs | 3 | 3% | 4 | 3% |
| Other | 5 | 4% | 13 | 8% |
| Total number of DAFW† cases reported to SOII | ||||
| 0 Cases | 19 | 17% | 48 | 30% |
| 1–2 Cases | 50 | 44% | 66 | 42% |
| 3 or More | 44 | 39% | 44 | 28% |
Data presented are number of establishments and column percentages.
Includes three interviews among establishments where someone other than the interviewee completed the OSHA recordkeeping forms. These three interviews are excluded from additional analysis.
Includes 83 establishments that refused to participate, 14 scheduled interviews canceled by the establishment, and 61 establishments that never returned calls requesting to schedule an interview.
†DAFW, one or more days away from work following the day of injury.
More than half of the interviews were conducted among establishments with 50 or more employees, 60% were from fixed site industries, and 50% were the sole unit operated by the employer. Sixty-eight establishments (62%) were classified as complete reporters and 42 establishments (38%) were considered under-reporters.
OSHA Recordkeeping Practices
OSHA recordkeeping forms were maintained in 97 of the 110 interviewed establishments. No OSHA records were maintained at 13 establishments. Seven of the 13 establishments that did not complete OSHA forms were partially exempt from OSHA recordkeeping requirements, requiring them to complete OSHA recordkeeping forms only during participation in the SOII; the other 6 establishments were required to maintain OSHA forms each year, regardless of BLS survey participation. These non-exempt establishments were among a range of industries including: manufacturing (2 establishments); transportation (1 establishment); construction (1 establishment); health care (1 establishment); and public administration (1 establishment). Five of the six establishments that lacked mandated OSHA records employed between 1 and 49 workers.
Respondents from the 97 establishments that maintained OSHA records did not fully understand what to record as a case, when to document a case, and how to classify it. Half of the establishments that maintained OSHA logs reported using the OSHA case definition to determine, which cases to record on the log, while the other half of respondents extended inclusion to all WC claims, all workplace injuries and illnesses that result in a medical visit, or all injuries reported to the respondent regardless of severity. Forty-four establishments did not record cases on the log within the timeframe required by the recordkeeping regulations and, instead, logged cases at some other time interval, such as the end of each year or upon receipt of workers' compensation paperwork or medical documentation. One in five respondents erroneously classified certain DAFW cases as days of job transfer or restriction only (DJTR) cases due to a misunderstanding of the classification criteria. For cases resulting in both missed work and restricted work or job transfers, these respondents classified the case as the outcome (DAFW or DJTR) with the greater number of days.
The responsibility of recording injuries among temporary workers was widely misunderstood. Fifty-three establishments utilized temporary help to augment their workforce and provided day-to-day supervision of the temporary workers. Among these 53 establishments that used temporary help, 19 respondents (36%) stated that injuries among temporary workers would be included on the establishment's OSHA 300 log as required by the recordkeeping regulations, while nearly half of the respondents would not include the injuries, either because they were omitted from the establishment's logs (21 respondents, 40%) or because temporary workers were used by an establishment where OSHA forms were not completed (5 respondents, 9%). The remaining eight respondents did not know whether to record temporary worker injuries. Some stated they would rely on the advice of the temporary staffing agency.
One in ten respondents (n = 11) complied with all four measured aspects of the OSHA recordkeeping regulations: using the OSHA case criteria to determine eligibility for OSHA records; recording cases with the required time limit; correctly assigning severity for DAFW and DJTR cases; and appropriately recording injuries among temporary workers.
Completeness of Injury and Illness Reporting in SOII compared With WC Data
Table2 presents OSHA injury and illness recordkeeping practices by completeness of injury reporting in SOII compared with WC data. Similar portions of complete reporters and under-reporters referred to the OSHA case criteria to determine, which events to record on the log. The greatest difference between complete reporters and under-reporters was found for the practice of logging all injuries and illnesses resulting in a visit to a health care provider, a case definition employed by 24% of complete reporters compared with 5% of incomplete reporters.
II.
OSHA Recordkeeping Practices Among Interviewed Establishments by Differences in Injury and Illness Reporting (n = 110)
| Total | Complete reporters | Under-reporters | ||||
|---|---|---|---|---|---|---|
| Total | 110 | 100% | 68 | 100% | 42 | 100% |
| What respondent records on OSHA log | ||||||
| Injuries meeting the OSHA case definition | 49 | 45% | 30 | 44% | 19 | 45% |
| Injuries resulting in a workers' compensation claim | 23 | 21% | 12 | 18% | 11 | 26% |
| Injuries resulting in medical visit | 18 | 16% | 16 | 24% | 2 | 5% |
| Injuries reported to company regardless of severity | 7 | 6% | 3 | 4% | 4 | 10% |
| Establishment does not keep OSHA logs | 13 | 12% | 7 | 10% | 6 | 14% |
| When respondent records cases on OSHA log | ||||||
| Within 7 days | 53 | 48% | 35 | 51% | 18 | 43% |
| End of year | 15 | 14% | 11 | 16% | 4 | 10% |
| Other time interval | 11 | 10% | 5 | 7% | 6 | 14% |
| After receiving documents (e.g., WC or medical) | 18 | 16% | 10 | 15% | 8 | 19% |
| Establishment does not keep OSHA logs | 13 | 12% | 7 | 10% | 6 | 14% |
| How respondent classifies cases on OSHA log as DAFW*, DJTR**, Other | ||||||
| Follows OSHA's definition of most severe | 78 | 71% | 46 | 68% | 32 | 76% |
| Classifies as outcome with greatest total days | 19 | 17% | 15 | 22% | 4 | 10% |
| Establishment does not keep OSHA logs | 13 | 12% | 7 | 10% | 6 | 14% |
| Whether respondent records temporary worker injuries on OSHA log | ||||||
| Yes, respondent records | 19 | 17% | 14 | 21% | 5 | 12% |
| No, respondent does not record | 21 | 19% | 14 | 21% | 7 | 17% |
| DK, respondent unsure whether they record | 8 | 7% | 3 | 4% | 5 | 12% |
| Supervises temp workers, does not keep OSHA logs | 5 | 5% | 4 | 6% | 1 | 2% |
| Does not host or supervise temps | 57 | 52% | 33 | 49% | 24 | 57% |
Data presented are number of establishments and column percentages.
DAFW, a case with one or more days away from work following the day of injury.
DJTR, a case with one or more days of restricted work or transfer to another job following the day of injury.
In a simple bivariate analysis of complete reporting by each of the four aspects of OSHA recordkeeping in which values were grouped into one of two response options (follows regulation, does not follow regulation), no association with underreporting was found for following any individual aspect of the regulation including: uses the OSHA case criteria (χ2 = 0.01, P = 0.91); records within 7 days (χ2 = 0.77, P = 0.38); correctly classifies severity (χ2 = 0.92, P = 0.34); or records injuries among temporary workers (χ2 = 0.77, P = 0.38).
Table3 presents select business characteristics by complete reporting of WC claims in SOII. Compared with establishments that reported all WC claims in SOII, a greater portion of under-reporters operated multiple shifts (71% of underreports compared with 43% of complete reporters, P < 0.01) or used injury and illness data as a measure of job performance for supervisors or injury and illness record keepers (33% compared with 13%, P < 0.05). Underreporting of WC claims in SOII was more common among establishments instructed to provide detailed case information for a sample of DAFW cases compared with establishments expected to detail all DAFW cases. Among the seven establishments instructed to submit only cases that occurred within dates defined by BLS, all seven had unreported WC claims that met the SOII sub-sampling criteria, whereas 40% of the 103 establishments instructed to report all cases had unreported WC claims (P < 0.001). Directing injured employees to a health care provider selected by the employer was more common among complete reporters (48%) than under-reporters (26%). No statistical difference between complete reporters and under-reporters was found for the use of injury and illness data to award prizes in safety competitions or including injury and illness data in bids for contacts or subcontracts.
III.
Select Establishment Characteristics Among Interviewed Establishments by Differences in Injury and Illness Reporting
| Total | Complete reporters | Under-reporters | P-value* | ||||
|---|---|---|---|---|---|---|---|
| Total | 110 | 100% | 68 | 100% | 42 | 100% | |
| Cases requested by BLS | 0.001 | ||||||
| All cases at sampled unit | 103 | 94% | 68 | 100% | 35 | 83% | |
| Cases with BLS-specified injury dates | 7 | 6% | 0 | 0% | 7 | 17% | |
| Total** | 109 | 100% | 67 | 100% | 42 | 100% | |
| Work shifts operated by establishment | 0.004 | ||||||
| Multiple shifts | 59 | 54% | 29 | 43% | 30 | 71% | |
| Single shift | 50 | 46% | 38 | 57% | 12 | 29% | |
| Company uses of establishment injury and illness data | |||||||
| Used to measure supervisors' or respondent's job performance | 23 | 21% | 9 | 13% | 14 | 33% | 0.013 |
| Not used as measure of job performance | 86 | 79% | 58 | 87% | 28 | 67% | |
| Used as metric in worker safety award program | 22 | 20% | 12 | 18% | 10 | 24% | 0.455 |
| Not used as metric in worker safety award program | 87 | 80% | 55 | 82% | 32 | 76% | |
| Included in bids for contracts or subcontracts | 24 | 22% | 16 | 24% | 8 | 19% | 0.786 |
| Not included in bids, or does not bid for contracts, subcontracts | 71 | 65% | 42 | 63% | 29 | 69% | |
| Participates in bids, did not know whether data was included | 14 | 13% | 9 | 13% | 5 | 12% | |
| Choice of health care provider | 0.025 | ||||||
| Employer chooses health care provider | 43 | 39% | 32 | 48% | 11 | 26% | |
| Injured worker chooses health care provider | 66 | 61% | 35 | 52% | 31 | 74% | |
| Unionization | 0.193 | ||||||
| Unionized workforce | 41 | 38% | 22 | 33% | 19 | 45% | |
| Workforce not unionized | 68 | 62% | 45 | 67% | 23 | 55% | |
Data presented are number of establishments and column percentages.
Tests are Fisher's exact test or Pearson's chi-squared test.
One respondent was excluded from the analysis because he could not speak to certain business practices. He was not an employee of the company but rather the company's contracted Third Party Administrator for workers' compensation account management, and provided injury and illness recordkeeping services including completing the SOII.
DISCUSSION
The SOII requires survey participants to report information on injuries and illnesses in accordance with the OSHA recordkeeping regulations. However, 90% of the SOII respondents we interviewed failed to comply with one or more of the required components through either a misunderstanding of or a disregard for the OSHA recordkeeping regulations. This included 12% of interviewed establishments where no OSHA injury and illness records were maintained. Non-compliance with OSHA recordkeeping regulations extended to: (a) the criteria used to determine, which incidents were recorded on the OSHA 300 logs; (b) the scope of the workforce covered by the establishment's records; (c) when incidents were documented on OSHA forms; and (d) how to classify the incident in terms of severity. While earlier research also found a failure of companies, especially smaller companies, to maintain OSHA records [Seligman et al., 1988] and identified misconceptions among company managers and health and safety personnel regarding the criteria used to determine, which cases to record on the OSHA log [Pransky et al., 1999], this is the first study we know to assess injury and illness recordkeeping compliance for the current OSHA recordkeeping regulations, implemented in 2002.
Many of the observed recordkeeping practices that did not comply with the OSHA regulations were connected to WC administrative practices; OSHA recordable cases were equated with WC claims, and often OSHA forms were not completed until WC paperwork was received or until a claim ruling had been made. Although, there is some overlap between OSHA recordable cases and WC claims, each system has distinct independent eligibility criteria. Despite the BLS's attempt to standardize national injury estimates and decouple the data from WC by replacing the WC-based Supplementary Data System with the current SOII [Abraham et al., 1996], in Washington State the relationship persists. When respondents equate SOII cases with WC claims, SOII estimates of injuries and illnesses become a reflection of the state-based WC system, rather than a standard definition employed nation-wide. Waiting periods for wage replacement eligibility, restrictions related to coverage of conditions, choice of health care provider, and benefit adequacy are among the variable aspects of state-specific WC systems that may impact a worker's decision to file a claim [Azaroff et al., 2002]. It is these characteristics that may explain some portion of the differences in state-specific estimates of occupational injuries and illnesses published by the BLS rather than true differences in injury rates [Boden and Ruser, 2003; Boden and Ozonoff, 2008; Mendeloff and Burns, 2013]. The degree of dependence between SOII and WC data may vary by state, further complicating the comparability of the SOII estimates across states.
This dependence between OSHA cases and WC claims was most evident in the practice of recording injuries among temporary workers. The host or client employers frequently expressed the erroneous belief that the responsibility for recording injuries among temporary workers was aligned with the liability for the WC claim and would thus fall to the temporary staffing agency. Phipps and Moore [2010], in interviews conducted with Washington DC metropolitan area SOII respondents, found strikingly similar results for recording temp worker injuries, despite interviewing a more knowledgeable group of respondents. Our interviews suggest that injuries among temporary workers are not captured in the national surveillance system since many respondents believe the temporary agency to be responsible for logging the incident on the forms used in data collection. Confusion surrounding the responsibility to record injuries among temporary workers may have substantial impact on the accuracy of employer-reported injuries and illnesses, especially as temporary help services continue to provide an attractive alternative to hiring permanent employees [Luo et al., 2010].
For many employers in Washington State, the WC claims data are a readily available source of injury and illness data and medical care information, accessible online through the WC Claim and Account Center. Yet, equating OSHA log recording criteria with WC claim status did not result in complete reporting of all SOII-eligible WC claims. The WC data system requires some amount of effort to isolate all claims for a given time frame, and complete case ascertainment within the system may require more resources than those dedicated by respondents who reported using WC claims data for reports of workplace injuries and illnesses. Additionally, some respondents may have claimed to use WC data because interviewers were employees of the same state agency that operates the WC insurance program. Stated reliance on WC data may be an indication of absent or disorganized recordkeeping, suggesting that respondents who lack an injury tracking system may instead gather whatever injury data are available when completing the SOII.
Of the business characteristics examined for a possible association with injury reporting, those related to communication appeared to be integral to reporting, namely communication between the injured worker and the establishment record keeper, between the record keeper and the health care provider, and between the record keeper and the BLS data collection staff. For instance, multiple work shifts present a barrier to communication between the injured worker and the record keeper. Internal injury reporting systems may not be adequate for capturing incidents that occur outside the hours worked by the primary record keeper, leading to discrepancies between SOII case reports and WC claims among establishments that operate multiple shifts. This is a non-trivial finding given the association between non-day shift work and increased risk of occupational injury [Dembe et al., 2006; Mustard et al., 2013]. Health care providers provide many of the data elements captured in injury recording systems. Directing injured employers to a specific health care provider may help facilitate communication between the record keeper and the health care provider regarding treatment provided, estimated return to work dates, and opportunities for job modifications. This relationship between the health care provider and the establishment is then reflected in enhanced establishment recordkeeping. Limited communication between the BLS data collection staff and survey respondents can also pose problems; all seven of the interviewed establishments instructed by BLS to report on cases occurring within a specified timeframe (to limit the response burden to approximately fifteen cases) were found to have unreported WC claims with BLS-requested injury dates. While some discrepancies in case reporting may be due to differences in the classification of injury dates between the employer and WC, in most cases a difference of a few days would not be sufficient to exclude the case from the eligible time frame. Instead, respondents appear not to follow the instructions provided by BLS defining the sub-sample of injuries to be reported.
Of the three uses of company injury and illness data we explored that are widely believed to incentivize underreporting [Pransky et al., 1999; US Government Accountability Office, 2012], WC claims not reported in SOII were found more often among establishments using injury and illness data as a measure of the respondent's job performance. This practice directly impacts respondents, rewarding the record keeper for low injury rates and giving unfavorable performance reviews when rates are high. In response to this practice, individuals who control the company's injury data exercise discretion when deciding, which cases to report and to make recordkeeping decisions independent of WC claims data.
It is important to note that other practices, including the use of injury and illness data in workplace safety awards programs, may also discourage reporting but an effect would not be seen when measured against WC claims data. Whereas rewarding record keepers for low injury rates may have little impact on a worker's decision to file a WC claim, directly rewarding workers for low injury rates (through safety incentive programs) may be an effective method of dissuading a worker from reporting the injury to the employer and as well as from filing a WC claim. Because we evaluated the completeness of the SOII data against the WC claims data, we would not identify incomplete reporting among establishments that sponsor such practices.
While we found evidence of under-reporting, there were also examples of over-reporting, that is, reporting injuries and illnesses that did not meet the OSHA case criteria. Certain recordkeeping practices such as recording all injuries and illnesses that result in a medical visit regardless of whether the services provided meet the OSHA definition of medical treatment and recording all injuries captured by the company's injury reporting system regardless of severity likely result in the recording of more cases than required. Because this practice was not observed in all establishments, it presents another challenge to comparing SOII data across establishments, artificially inflating the rate of injuries and illnesses among establishments who over-report, likely because they have no business incentive to minimize the number of cases reported, compared to establishments engaged in such activities.
Additional employer characteristics may be associated with under-reporting but were masked by the selection criteria used to recruit interviewees. It is outside the scope of this study to assess the relationship between incomplete reporting and industry, employer size, or number of worksites, which would require a representative sample of SOII eligible Washington State establishments. Also, a larger sample would allow for multivariate analyses. The bivariate analyses presented here, while contributing to our understanding of employer injury and illness recordkeeping, do not address potential correlation among variables. For example, companies that operate multiple shifts may also tend to have a sufficient number of injuries to be asked by the BLS to report a sub-sample of injuries based on the date of injury. Including these factors in a multivariate model would explore the effect of each, independent of the other. The bivariate statistics suggest topics to explore in future studies.
There are several possible approaches to the classification of reporting completeness. Based on our SOII case-WC claim record linkage, most establishments with incomplete reporting were found to underreport by one claim. We therefore chose to define “under-reporters” as any establishment with at least one unreported WC claim. Another approach would be to look at degrees of underreporting, separating those with minimal underreporting from those with more substantial underreporting. This could be achieved by evaluating unreported cases as a portion of total cases, or by using the distribution of unreported claims among groups of similar establishments to create categories of reporting completeness (e.g., above or below the median number of unreported claims within each size and industry grouping). This would highlight the practices of the worst reporters, but possibly obscure the practices that differentiate the complete reporters from the majority of under-reporters with few missed cases.
There are several limitations to this study. First, findings may have been affected by recall and self-reported data. OSHA logs completed by the establishment were not reviewed during the course of the interview and respondents may have answered with what they considered to be socially desirable responses, since violations of the standards discussed during the interview are punishable under the law. Respondents in establishments that had not experienced an injury or illness in years had difficultly answering procedure-related questions. Also, respondents were asked to discuss typical injury and illness reporting practices, although, it may be the atypical scenarios that explain a portion of the discrepancy between the SOII and WC data.
Second, completeness of injury reporting was assessed using only SOII and WC data, two data sources likely correlated, meaning, if a case was reported in SOII, it is probable that a WC claim was also filed. Another data source for occupational injuries, such as a worker survey, would have presented an opportunity to reconsider our classification of establishments as complete reporters and under-reporters. However, reasons for data discrepancies between SOII data and WC claims data may differ from reasons for data discrepancies when compared with a third data source. Another constraint of linked SOII and WC data is the inability to verify SOII reports of injuries among temporary workers. Although, we can identify claims among temp workers within the WC data, we cannot determine whether the injury occurred while on assignment at an establishment participating in the SOII, nor can we determine whether the establishment provided supervision of the temporary help work and thus, whether the injury was eligible for inclusion on the client company's OSHA 300 log.
Third, the generalizability of our findings is limited. Because state-specific WC insurance regulations and administrative practices potentially impact recordkeeping, our results may not hold in other states. Also, the findings should be viewed cautiously given the study response rate of 42%. The recordkeeping practices of establishments that did not agree to participate may be sufficiently different from participants to alter the observed relationships. This is of particular concern since the characteristics of participants differed from non-participants; smaller establishments and the construction industry were less likely to participate than others. These establishments may have deficient recordkeeping practices or actively discourage injury reporting and were reluctant to participate because of anticipated disapproval of their practices. It is reasonable to expect someone aware of their substandard or dubious practices to refuse to participate in a voluntary study; we did, however, interview many who were unaware of their non-compliance.
CONCLUSIONS
This study identified several employer misconceptions and non-compliant practices related to the OSHA recordkeeping requirements. Many of the recordkeeping practices discussed suggest a limited comparability of BLS data across employers, industries, or states. While some establishments report cases in accordance with the OSHA recordkeeping regulations, others report cases gleaned from WC data. To improve compliance with the regulations, OSHA should increase outreach and improve the training they provide, especially regarding injuries among temporary workers. However, education may not be sufficient with no requirement to participate in recordkeeping training. Revised OSHA forms or instructions that accompany the forms to clarify the requirements are another option, and would reach a wider audience than education efforts alone. The BLS could echo such efforts, emphasizing in their survey instructions the responsibility to record injuries among temporary workers and augmenting the survey forms to ease the reporting of these incidents.
Beyond maintaining logs in compliance with the regulations, complete and accurate SOII data are dependent on the transfer of information between many parties: injured worker, establishment record keeper, health care provider, and BLS data collection staff. A barrier or breakdown in communication between any two parties can lead to unreported cases. The BLS can work to improve communication with SOII respondents, but other aspects of employer recordkeeping must be addressed at the level of the individual establishment.
Finally, participation in the SOII is likely inconsequential for many respondents. By design, the average time required to complete the SOII is estimated to be 24 min, and there are no penalties for inaccurate responses. This motivates some respondents to complete the survey with whatever data are convenient rather than reviewing the year's incidents to determine eligibility. Without providing employers a reason for becoming more fully engaged in the data collection process, modifications to data collection forms and procedures may be limited to a marginal impact on data quality.
Acknowledgments
Grant sponsor: Bureau of Labor Statistics (BLS); Grant number: OS20358-11-75-J-53. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the views of the BLS. We thank Polly Phipps for graciously sharing the interview guide she developed for similar interviews and Cody Spann, Nicole Reister, Michael Foley, Nanette Yragui, and Whitney Johnson for assistance with the interviews. We also thank Polly Phipps and Leslie Boden for their thoughtful comments on the manuscript.
Notes
All establishments selected for participation in the SOII are required to maintain OSHA injury and illness records for the duration of the survey year, including establishments partially exempt from OSHA recordkeeping requirements based on industry or number of employees. The recordkeeping requirements in Washington, an OSHA state plan state, are identical to the federal regulations except in the lists of industries partially exempt from the recordkeeping requirements. Federal regulations exempt offices and clinics of health care providers and dentists and public educational services except elementary and secondary schools and public libraries from recordkeeping requirements (unless required in writing to do so by OSHA or BLS). In Washington, these establishments are required to comply with the regulations Washington Administrative Code, 2008. § 246-27-00105. Accessed at http://apps.leg.wa.gov/wac/default.aspx?cite=296-27-00105 on March 20, 2013.
Claims for workplace injuries must be filed within one year of the date of injury; claims for occupational diseases must be filed within 2 years following the physician's written notification to the worker of the presence of an occupational disease and eligibility to file a claim for disability benefits.
‘Kept on salary’ is a practice in which the employer can lower their WC claim costs by retaining the injured worker on the company's payroll. For the limited period of time the attending health care provider has recommended work restrictions, the worker continues to receive their full pay from the employer in lieu of receiving indemnity benefits through WC.
REFERENCES
- Abraham KG, Weber WL, Personick ME. Improvements in the BLS safety and health statistical system. Mon Labor Rev. 1996;119:3–9. [Google Scholar]
- Azaroff LS, Levenstein C, Wegman DH. Occupational injury and illness surveillance: Conceptual filters explain underreporting. Am J Public Health. 2002;92:1421–1429. doi: 10.2105/ajph.92.9.1421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boden LI, Ozonoff A. Capture-recapture estimates of nonfatal workplace injuries and illnesses. Ann Epidemiol. 2008;18:500–506. doi: 10.1016/j.annepidem.2007.11.003. [DOI] [PubMed] [Google Scholar]
- Boden LI, Ruser JW. Workers' compensation “reforms,” choice of medical care provider, and reported workplace injuries. Rev Econ Stat. 2003;85:923–929. [Google Scholar]
- Dembe AE, Erickson JB, Delbos RG, Banks SM. Nonstandard shift schedules and the risk of job-related injuries. Scand J Work Environ Health. 2006;32:232–240. doi: 10.5271/sjweh.1004. [DOI] [PubMed] [Google Scholar]
- Leigh JP, Marcin JP, Miller TR. An estimate of the U.S. Government's undercount of nonfatal occupational injuries. J Occup Environ Med. 2004;46:10–18. doi: 10.1097/01.jom.0000105909.66435.53. [DOI] [PubMed] [Google Scholar]
- Luo T, Mann A, Holden R. The expanding role of temporary help services from 1990 to 2008. Mon Labor Rev. 2010;133:3–16. [Google Scholar]
- Mendeloff J, Burns R. States with low non-fatal injury rates have high fatality rates and vice-versa. Am J Ind Med. 2013;56:509–519. doi: 10.1002/ajim.22047. [DOI] [PubMed] [Google Scholar]
- Mustard CA, Chambers A, McLeod C, Bielecky A, Smith PM. Work injury risk by time of day in two population-based data sources. Occup Environ Med. 2013;70:49–56. doi: 10.1136/oemed-2012-100920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nestoriak N, Pierce B. Comparing workers' compensation claims with establishments' responses to the SOII. Mon Labor Rev. 2009;132:8. [Google Scholar]
- Oleinick A, Zaidman B. The law and incomplete database information as confounders in epidemiologic research on occupational injuries and illnesses. Am J Ind Med. 2010;53:23–36. doi: 10.1002/ajim.20763. [DOI] [PubMed] [Google Scholar]
- Phipps P, Moore D. 2010. Employer interviews: Exploring differences in reporting work injuries and illnesses in the survey of occupational injuries and illnesses and state workers' compensation claims, Paper presented at: 2010 Joint Statistical Meetings, Vancouver, BC, Canada.
- Pransky G, Snyder T, Dembe A, Himmelstein J. Under-reporting of work-related disorders in the workplace: A case study and review of the literature. Ergonomics. 1999;42:171–182. doi: 10.1080/001401399185874. [DOI] [PubMed] [Google Scholar]
- Revised Code of Washington. 1972. § 51.12.010. Accessed at http://apps.leg.wa.gov/rcw/default.aspx?cite=51.12.010 on March 20, 2013.
- Revised Code of Washington. 2005. § 51.28.020. Accessed at http://apps.leg.wa.gov/rcw/default.aspx?cite=51.28.020 on March 20, 2013.
- Rosenman KD, Kalush A, Reilly MJ, Gardiner JC, Reeves M, Luo Z. How much work-related injury and illness is missed by the current national surveillance system. J Occup Environ Med. 2006;48:357–365. doi: 10.1097/01.jom.0000205864.81970.63. [DOI] [PubMed] [Google Scholar]
- Ruser J. Examining evidence on whether BLS undercounts workplace injuries and illnesses. Mon Labor Rev. 2008;131:13. [Google Scholar]
- Ruser JW. 2010. Allegations of undercounting in the BLS survey of occupational injuires and illnesses, Paper presented at: 2010 Joint Statistical Meetings, Vancouver, BC, Canada.
- Seligman PJ, Sieber WK, Pedersen DH, Sundin DS, Frazier TM. Compliance with OSHA record-keeping requirements. Am J Public Health. 1988;78:1218–1219. doi: 10.2105/ajph.78.9.1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- US Department of Health and Human Services; Centers for Disease Control and Prevention; National Center for Chronic Disease Prevention and Health Promotion. 2007. Link Plus. Accessed at http://www.cdc.gov/cancer/npcr/ on September 28, 2012.
- US Department of Labor. 2009. Occupational Safety and Health Administration: Injury and illness recordkeeping national emphasis program. Accessed at http://www.osha.gov/OshDoc/Directive_pdf/CPL_02_09-08.pdf on March 20, 2013.
- US Department of Labor, Bureau of Labor Statistics. 2012. BLS Handbook of Methods, Chapter 9. Occupational Safety and Health Statistics. Accessed at http://www.bls.gov/opub/hom/pdf/homch9.pdf on March 20, 2013.
- US Government Accountability Office. 2009. Workplace Safety and Health: Enhancing OSHA's records audit process could improve the accuracy of worker injury and illness data. GAO- 10-10. Accessed at http://www.gao.gov/products/GAO-10-10 on March 20, 2013.
- United States Government Accountability Office. 2012. Workplace safety and health: Better guidance needed on safety incentive programs. GAO- 12-329. Accessed at http://www.gao.gov/assets/590/589961.pdf on March 20, 2013.
- Washington Administrative Code. 2008. § 246-27-00105. Accessed at http://apps.leg.wa.gov/wac/default.aspx?cite=296-27-00105 on March 20, 2013.