

Abstract
The early postpartum period lays important groundwork for later self-regulation as infants' dispositional traits interact with caregivers' co-regulatory behaviors to produce the earliest forms of self-regulation. Although emerging literature suggests that fetal exposure to maternal stress may be integral in determining child self-regulatory capacity, the complex pathways that characterize these early developmental processes remain unclear. The current study considers these complex, transactional processes in a low income, Mexican American sample. Data were collected from 295 Mexican American infants and their mothers during prenatal, 6- and 12-week postpartum home interviews. Mother reports of stress were obtained prenatally, and mother reports of infant temperament were obtained at 6 weeks. Observer ratings of maternal sensitivity and infant regulatory behaviors were obtained at the 6- and 12-week time points. Study results indicate that prenatal stress predicts higher levels of infant negativity and surgency, both of which directly or interactively predict later engagement in regulatory behaviors. Unexpectedly, prenatal stress also predicted more engagement in orienting, but not self-comforting behaviors. Advancing understandings about the nature of these developmental pathways may have significant implications for targets of early intervention in this high risk population.
Keywords: prenatal stress, temperament, regulation, maternal sensitivity
The study of self-regulation has been regarded as “the single most crucial goal for advancing an understanding of development and psychopathology” (Posner & Rothbart, 2000, p. 427). Self-regulation is believed to have roots in infancy, emerging as a result of interactions between infant dispositional regulation and caregiver co-regulatory functions (Calkins, 1994; Rothbart, 2011). Regulatory behaviors in turn have been linked to children's later social skills, academic competence, behavior problems, and even psychopathology in adulthood (Althoff, Verhulst, Rettew, Hudziak, & van der Ende, 2010; Eisenberg, Liew, & Pidada, 2004; Eisenberg, et al., 2009). Mexican American youths are at disproportionate risk for many of these adverse adjustment outcomes, and yet relatively little is known about the extent to which these risks may begin to accumulate as early as the prenatal period. Although prior studies have linked prenatal stressors to infant temperament and socioemotional development (e.g., Gutteling, et al., 2005), the nature of relations in Mexican American families remains relatively unexplored. The current study addresses these critical questions in a sample of low-income Mexican American mothers and infants.
1.1. Regulatory Behaviors in Infancy
Although scholars disagree about when children are first capable of purposeful self-regulation, behaviors such as orienting and self-comforting are thought to serve regulatory functions beginning in early infancy (Rothbart, Ziaie, & O'Boyle, 1992). Orienting, or direction of attention towards or away from distressing objects in the environment, is considered fundamental to the development of self-regulation (Ruff & Rothbart, 1996). Infants who can more readily disengage gaze from distressing objects are less susceptible to negative affect, are easier to soothe, and evidence greater capacities for later emotion regulation (Crockenberg & Leerkes, 2004; Morales, Mundy, Crowson, Neal, & Delgado, 2005). Given that infants' executive control over orienting behaviors is believed to emerge around 3 months of age (Haith & McCarty, 1990), identification of early caregiver and child contributions during this critical period may help clarify early pathways involved in their development. Self-comforting, or self-stimulating behaviors meant to elicit calming such as thumb-sucking, face rubbing, and self-clasping (Crockenberg & Leerkes, 2004), comprises another important set of regulatory strategies present in infancy. Self-comforting behaviors are observed at peak frequency around 3 months of age (Rothbart, et al., 1992), and are instrumental for modulating infants' experiences of emotional, physiological, and motoric arousal (Field, 1999; Stifter & Braungart, 1995).
1.2. Contributions of Infant Temperamental Reactivity
Temperament reflects constitutional differences in emotional, motor, and attentional reactivity to change as well as the regulation of this reactivity, and is believed to serve as a basis for children's later self-regulatory functioning (Rothbart, 2011). In fact, Feldman (1999) argues that the emergence of self-regulation can only be understood when infant temperament is considered. Two dimensions of temperament that may confer risk for regulatory capacity are negativity and surgency (Gartstein & Rothbart, 2003). Negativity encompasses general negative mood, fear, and anger responses, and may presuppose risk both by implicating the relative frequency of the infant's distress response and by creating more opportunities for negative responding by others (Belsky, 1997). These heightened levels of arousal may in turn interfere with children's capacities to self-regulate. Indeed, children higher in negativity are more likely to engage in less effective regulatory strategies (e.g., kicking, banging), and to fixate attention on the distressing objects (Calkins, Dedmon, Gill, Lomax, & Johnson, 2002).
Surgency includes components of both positive affectivity and high activity level, and has been implicated both as a risk and protective factor for regulation (Gartstein, Slobodskaya, Putnam, & Kinsht, 2009; Rothbart, et al., 1992). The high levels of intensity associated with surgency may exaggerate expressions of negativity (Rothbart, Derryberry, & Hershey, 2000), but the positive affect associated with surgency may promote positive infant-caregiver interactions that facilitate caregiver responsiveness (Molfese, et al., 2010). Because studies investigating contributions of surgency to infant regulatory capacity are limited, connections between the two remain to be clarified.
1.3. Maternal Sensitivity, Infant Temperament, and Infant Regulatory Capacity
Caregiver sensitivity is regarded as an important predictor of infant regulation. Sensitivity has been defined as the caregiver's availability, attentiveness, and responsiveness to infant cues according to the infant's age appropriate growth needs (Ainsworth, Blehar, Waters, & Wall, 1978). Sensitive caregiving has been found to predict increased consistency in infants' state regulation as early as the first ten days of life (Sander, Julia, Stechler, & Burns, 1972). Over time and across interactions, consistently sensitive caregiving may re-program infants' stress response in a way that further modulates negative reactivity over time (Braungart-Rieker, Hill-Soderlund, & Karrass, 2010; Feldman, 2010). Sensitive caregiving may also help to co-regulate infant states and thus to support infants' capacities to employ more sophisticated regulatory strategies (Conradt & Ablow, 2010).
1.4. Prenatal Stress and Infant Regulatory Capacity
Exposure to maternal prenatal stress during critical periods of fetal brain and body development may influence infants' subsequent capacities for regulation (see Weinstock, 1997 for a review). Hormonal imbalances associated with maternal prenatal stress are believed to interfere with the normal development of the infants' stress response system (Seckl, 2001), which then impairs later capacities for emotional and behavioral regulation. Mother self-reports of stress, anxiety and depression during pregnancy have been linked to dysregulated infant states and decreased regulatory capacity, even after controlling for birth weight, psychosocial risks, and maternal postnatal anxiety and depression (Huizink, Robles de Medina, Mulder, Visser, & Buitelaar, 2002; O'Connor, et al., 2007).
Maternal prenatal stress has also been associated with infant temperamental characteristics that confer risk for poor regulatory functioning. Infants prenatally exposed to maternal stress exhibit higher observational and mother reports of infant negativity even after controlling for maternal postnatal mood (Huizink, et al., 2002). Separate studies have linked maternal prenatal stress to infant temperament (Huizink, et al., 2002) and infant temperament to regulatory capacity (O'Connor, et al., 2007), but few studies to date have examined the extent to which infant temperament mediates the relations between maternal prenatal stress and infant regulatory capacity.
1.5. The Development of Self-Regulation in a High-Risk Context
Although regulatory processes emerging in the early childhood period are now widely recognized as important predictors of children's socioemotional adjustment, understanding about the development of self-regulation in minority groups at heightened risk for adjustment problems is limited. Specifically, Mexican American youth are at disproportionate risk for experiencing a range of poor adjustment outcomes compared to White and many other ethnic minority groups (Cauce, Cruz, Corona, & Conger, 2011), and yet little is known about the extent to which these risks may begin to accumulate beginning even before infants are born. Additionally, although Mexican American mothers are believed to experience higher rates of postpartum distress compared to their White counterparts (Gress-Smith, Luecken, Lemery-Chalfant, & Howe, 2012), less is known about whether these disparities may also apply to prenatal distress, and further whether prenatal distress may exert subsequent cascades of influence on infant regulatory capacity.
1.7. Current Study
The current study explores paths linking maternal prenatal stress to infants' regulatory capacity in a low-income, Mexican American sample. The study evaluated mother and infant behaviors during a highly stimulating mother-infant interaction task (Peek-A-Boo) at 6- and 12-weeks postpartum. Three hypotheses were addressed: first, infant engagement in self-comforting and orienting behaviors at 12 weeks was expected to correlate with decreases in distress across the same interaction task. Second, maternal prenatal stress was hypothesized to predict fewer infant regulatory behaviors, and infant temperamental characteristics were expected to mediate their relations. Specifically, higher levels of prenatal stress were expected to predict more negativity and surgency at 6 weeks, and both negativity and surgency were hypothesized to predict fewer regulatory behaviors at 12 weeks. Finally, maternal sensitivity was expected to moderate relations between infant temperament at 6 weeks and engagement in infant regulatory behaviors at 12 weeks, such that higher infant negativity and surgency would predict fewer regulatory behaviors at low levels of maternal sensitivity, but would not be related to regulatory behaviors at high levels of maternal sensitivity.
1. Methods
2.1. Participants
The current study included a subset of data collected from a larger prospective longitudinal study. Participants were 295 mother-infant dyads from low-income, Mexican American families recruited during pregnancy through a health clinic in the southwestern United States. Of women who were approached and eligible, 56% agreed to schedule a home visit, at which time informed consent was obtained. Eligibility criteria included fluency in either Spanish or English, self-identification as Mexican American, anticipated delivery of a singleton (based on ultrasound results). Low-income status was determined by eligibility for Medicaid or Federal Emergency Services coverage, or self-reported annual income below $25,000. Demographic characteristics are displayed in Table 1.
Table 1. Demographic and Descriptive Characteristics.
| Infant | Range; Mean (sd) |
|---|---|
| Gender (% male) | 50.3% |
| Gestational Age | 26-42; 39.2 (1.5)a 1190-4935; |
| Birth Weight (grams) | 3397.4 (467.1)b |
| 5 minute APGAR | 5-10; 8.9 (.5) |
| # Days in Hospital | 0-13; 2.3 (1.5) |
|
| |
| Family | |
|
| |
| Mother's mean age | 18-42; 27.9 (6.3) |
| Country of Origin | |
| % United States | 14.2% |
| % Mexico | 85.1% |
| % Other | 0.7% |
| Preferred Language (% Spanish) | 81.7% |
| Marital Status (% Married or Living Together) | 78.4% |
| Mother's level of education (% high school degree) | 39.3% |
| Median annual income | $10,001 - 15,000 |
| Mean # of people supported by income | 1-14; 4.3 (2.0) |
| % Diagnosed Medical Condition | 22.0% |
|
| |
| Key Study Variables | |
|
| |
| Mean # Family Stressors Endorsed | 0-6; .8 (1.3) |
| Maternal Sensitivity (6 weeks; n=134) | 1-5; 2.4 (1.1) |
| Child Temperament: Negativity (6 weeks; n=257) | 0.6-5.2; 2.4 (.7) |
| Child Temperament: Surgency (6 weeks; n=257) | .2-5.9; 2.3 (1.1) |
| Proportion of task engaged in self-comforting (12 weeks; n=58) | 0-1; .17 (.3) |
| Proportion of task averting gaze (12 weeks; n=58) | 0 - .87; .14 (.2) |
| Change in Distress across task (12 weeks; n=78) | -.28 - .45; .00 (.1) |
Note. Listwise deletion was used; n's were 295 unless otherwise noted.
9 infants were born premature (< 37 weeks gestation). Of these, 1 was born at 26 weeks, and 8 were born at 36 weeks; all remaining infants were full-term.
The same infant born at 26 weeks was the only one born very low birth weight (< 1500g).
2.2. Procedures
Participation in the larger longitudinal study involved one prenatal home visit (21-42 weeks gestation), four home visits within the first six postpartum months (6, 12, 18 and 24 weeks), and one laboratory visit at 12 months. Families were compensated for their participation. Data collection time points were corrected for infant gestational age when infants were born prior to 37 weeks gestation (n=9; one infant was born at 26 weeks, and 8 were born at 36 weeks. Because there was no evidence that the infant born at 26 weeks suffered health problems or was an outlier, the infant was retained for analyses). Because the larger longitudinal study employs a planned missingness design (Graham, Taylor, Olchowski, & Cumsille, 2006), all participants were expected to complete the prenatal, 6-week, and 12-month interviews, but each participant was randomly assigned to miss one of the data collection points at 12-, 18- or 24-weeks. In planned missingness designs, data are systematically Missing At Random (MAR; Rubin, 1978) to afford the opportunity to collect data from more participant families by allowing fewer data collections while only minimally affecting power (Graham, et al., 2006). For the current study, data were drawn from three study time points that spanned pregnancy to infant age 12 weeks (prenatal, 6, and 12 weeks), and corrected for planned missingness using Full Information Maximum Likelihood (FIML; Allison, 2003).
2.2.1. Home Interviews
Interviews were conducted in participants' homes in participants' choice of Spanish (82%) or English (18%). Questions were read aloud to reduce error variance due to participant literacy. The structured interviews contain self-report measures as well as structured mental-health assessments.
2.2.2. Interaction tasks
Observational data were obtained from structured mother-infant interactions during the 6- and 12-week home visits that were recorded with two high-definition cameras for later coding. The current study focused on data obtained during a peek-a-boo interaction task. Mothers were given a shield (e.g., book, blanket) to hide behind, and instructed to play peek-a-boo with their infants. This task was chosen because it is a stimulating activity expected to induce arousal and thus elicit infant regulation and maternal sensitivity to infant cues.
2.2.3. Coding of data
Observational data were obtained for a subsample of participants. Infant gaze (n=58), self-comforting (n=58), and emotional expressions (n=78) were coded using an adaptation of Tronick's Monadic Phases (Tronick, Als, & Brazelton, 1980) by four teams of two independent observers trained and supervised by a graduate research assistant. Inter-observer reliability was calculated for 20% of coded episodes by examining second-by-second agreement and calculating percent agreement and kappa reliability statistics following the stringent procedure established by Cohn and Tronick (1987). Maternal sensitivity (n=134) was coded using a subscale of the Parent-Child Interaction Rating Scales (PCIRS; Belsky, Crnic, & Gable, 1995) by two independent coders supervised by a graduate research assistant. Coders were trained to consensus and reliability was calculated for 20% of episodes.
2.3. Measures
2.3.1. Prenatal Stress
Mothers' self-report of family stressors were obtained during the prenatal home visit using the cultural/family conflict subscale of the Hispanic Stress Inventory (HSI; Cervantes, Padilla, & Salgado de Snyder, 1990). Sample items include: “Some members of your family have become too focused on themselves and less concerned about the family”, “you have been separated from family because of money or immigration problems”, and “your personal goals have been in conflict with family goals”. When mothers reported experiencing family stressors, they reported that stressors were anywhere from “not at all stressful” to “extremely stressful”, but most often reported perceiving family stressors to be “a little” or “moderately” stressful. Scores were formed by summing the count of family stressors (out of ten) that mothers reported experiencing in the last three months. The HSI family stress subscale was selected because it has demonstrated sensitivity for capturing chronic stressors that are particularly poignant to Mexican American women and that tend not to be captured by other stress scales developed primarily for use with White samples (Goodkind, Gonzales, Malcoe, & Espinosa, 2008), and its predictive and concurrent validity has been established in a number of Hispanic samples (e.g., Cervantes, Padilla, & Salgado de Snyder, 1991). Examinations of concurrent validity with other stress scales commonly used with White samples (i.e., daily hassles, r=.31, p<.01; perceived stress, .29, p<.01, negative life events, r=.48, p<.01; depression, r=.34, p<.01) within the current sample yielded medium to strong associations. Alpha scale reliability in the current sample was .63.
2.3.2. Infants' Regulatory Behaviors
Microcoded ratings of infant engagement in self-comforting or orienting regulatory behaviors were obtained at the 12-week home visits. Self-comforting was defined as infant engagement in one more of the following behaviors at any given time during the interaction: mouthing of self, object or mother, touching self, self-clasping, or rocking behaviors. Orienting was defined as infants' visual attention to any task unrelated object (i.e., looking away from mom or any objects used). Duration scores for each of the regulatory behaviors were obtained using the Observer XT 9.0 program to capture the amount of time infants engaged in self-comforting and orienting regulatory behaviors, and scores reflecting the proportion of time infants were engaged in each of the regulatory behaviors were calculated by dividing duration scores by total coded task time. Average percent agreement for self-comforting was 98%; Kappa reliability statistics could not be computed for self-comforting behaviors because the self-comforting codes were programmed as start-stop codes that were not mutually exclusive. Average percent agreement for infant gaze codes was 94% (kappa=.69).
2.3.3. Infant Distress
Microcoded ratings of infant emotional expressions were obtained at the 12-week home visits to verify the regulatory function of the aforementioned regulatory behaviors. Infant distress was defined as infant's displays of negative emotional expressions including sadness, fear/worry, frustration/anger, or grimace/disgust. Interobserver reliability for the scale was 96% agreement (kappa= .57). Though kappa reliability statistics tend to offer more precision in estimation about interobserver agreement, large discrepancies between achieved percent agreement and achieved kappa as observed here are sometimes indicative of the unreliability of the kappa statistic for capturing low frequency observations (Sim & Wright, 2005). In this case, the moderate kappa score likely reflected the relative infrequency of positive emotional expressions. Change scores representing the overall increase, decrease, or constant state of distress across the interaction were calculated by subtracting the proportion of distress observed during the first half of the task from the proportion of infant distress observed during the second half of the task. Change scores ranged from - .28 to .45. The criterion established a priori for corroborating regulatory function was that infant regulatory behaviors should be associated with negative distress change scores.
2.3.4. Infant Temperamental Reactivity
Maternal ratings of infant temperament were obtained at the 6-week time point using the negativity and surgency dimensions of the Infant Behavior Questionnaire-Revised (IBQ-R, Gartstein & Rothbart, 2003). Three of the total original 40 items comprising the surgency dimension were omitted due to programming errors (items 28-30). All remaining items were assessed for relevance to 6-week-old infants and were determined a priori to be applicable if they received greater than 50% response rates following recommendations by Gartstein (2011) all items received greater than 50% response rates, and thus were included in the computation of final scale scores. Scores for each of the dimensions were formed by averaging item scores for each of the subscales, and then by averaging subscale scores within each dimensions following practices by Gartstein & Rothbart (2003). Alpha scale reliabilities for the surgency and negativity dimensions for the current sample were .88 and .61, respectively. Alpha scale reliability for the negativity dimension improved to .73 when the “falling rate of reactivity” subscale was omitted, but the negativity dimension was kept intact to afford comparability to other studies.
2.3.5. Maternal Sensitivity
Observer ratings of maternal sensitivity were obtained at the 6-week time point during the peek-a-boo task using the sensitivity scale of the Parent-Child Interaction Rating Scales (PCIRS; Belsky, et al., 1995). Maternal sensitivity was defined as parent attunement and responsiveness to child needs, mood, interests, and capabilities, and was rated on a 5-point scale (1= almost no signs of parent sensitivity, 5= highly sensitivity/responsive). 100% of ratings fell within 1 scale point; and 50% of observations were coded to exact agreement. Because mother-infant interactions could not occur when infants were sleeping, data were coded as missing if infants were asleep for more than 2 minutes during the 3-minute task (n=44).
2.3.5. Potential Covariates
Demographic information and mother and infant health variables were considered as possible covariates in the present study. Demographic and mother health information (medical condition) was obtained prenatally either during recruitment or at the prenatal home interview. Infant birth outcomes (gestational age, birth weight, 5-minute APGAR, days in hospital, and gender) were obtained from hospital birth records. Variables were entered as covariates if they were significantly correlated with both the outcome variables and their predictors, as specified in the model.
2.4. Data Analytic Plan
2.4.1. Hypothesis Testing
Hypothesis 1 was tested using Pearson correlations. All remaining hypotheses were tested with a path analysis model using structural equation modeling (SEM) in Mplus 6.2 (Muthén & Muthén, 2010). Following Cohen, Cohen, West and Aiken (2003), all continuous predictors were centered and all categorical variables were dummy coded to reduce nonessential multicollinearity. Model fit was tested using χ2 test of fit, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and the comparative fit index (CFI). Good fit was defined a-priori as χ2 test probability value >.05, RMSEA values ≤ .06, SRMR values ≤ .08, and CFI values ≥ .95 (Hu & Bentler, 1999). Tests of the mediated effects were analyzed using bootstrapping (Shrout & Bolger, 2002). The interaction effects between maternal sensitivity and infant temperament dimensions were probed in simple slope analyses by using the model constraint command in Mplus 6.12.
2.4.2. Missing Data
Missingness for the current study was believed to be attributed to: planned missingness design, the status of data collection (i.e., not all participants had completed all timepoints), random assignment of video observations to be coded, or, in the case of coded observations for maternal sensitivity, infants' wakefulness during the interaction task. Therefore, data were treated as Missing At Random (MAR; Rubin, 1976) and corrected for using FIML. Finally, to avoid bias introduced by listwise deletion techniques while also maximizing power, full model analyses run in Mplus 6.12 included all available data points (Schafer & Graham, 2002). The benefits of using FIML over other methods increases as the missing data rate increases, and simulation studies with missing data rates up to 50% have been found to yield unbiased results (Enders, 2010).
2. Results
2.1. Preliminary analyses
Descriptive statistics for demographics, infant and mother health characteristics, and key study variables are presented in Table 1. Relations between demographics, health-related variables that may influence the prenatal environment or postnatal outcomes, infant temperament, maternal sensitivity, and infant regulatory behaviors were tested using Pearson correlations (see Table 2). Because mother's country of origin (0= US, 1=Mexico or Other) and preferred language (0=English, 1=Spanish) were related to both prenatal stress and infant temperamental characteristics, they were considered as covariates. However, because mother's country of origin became non-significant when entered simultaneously into the model with mother's preferred language (β = -.00, p=.99), mother's country of origin was dropped from analyses.
Table 2. Correlations.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Demographics | |||||||||||||||||||||
| 1. Mother's Age | - | .31 | .16 | .38 | -.18 | -.28 | .08 | .20 | .06 | -.10 | .08 | .02 | -.04 | -.04 | -.07 | -.10 | -.09 | -.12 | .09 | .13 | .17 |
| 2. Country of Origin | - | .18 | .66 | -.18 | -.19 | -.04 | .06 | .07 | -.01 | .04 | .09 | -.04 | .11 | -.11 | -.14 | -.17 | .02 | .16 | -.02 | .04 | |
| 3. Years in US | - | -.24 | .14 | -.06 | -.01 | .29 | -.02 | -.03 | .02 | -.04 | .07 | -.07 | -.09 | -.19 | -.13 | -.11 | .02 | .26 | -.06 | ||
| 4. Preferred Language | - | -.19 | -.23 | -.03 | .19 | -.01 | .04 | .03 | .19 | -.19 | .09 | -.15 | -.11 | -.15 | .02 | .14 | -.03 | -.08 | |||
| 5. Marital Status | - | .03 | -.17 | -.07 | -.13 | -.06 | -.07 | .01 | .02 | -.09 | .16 | .12 | .08 | .01 | -.00 | .12 | -.15 | ||||
| 6. Mother's Education | - | .24 | -.17 | .02 | -.02 | -.10 | -.06 | .03 | .09 | .14 | .11 | .03 | .06 | .07 | -.05 | .04 | |||||
| 7. Family's Annual Income | - | .03 | .09 | -.03 | -.07 | -.08 | .16 | .09 | -.07 | .01 | .08 | .11 | -.08 | -.01 | -.10 | ||||||
| 8. # Supported by Income | - | -.04 | -.03 | .03 | -.03 | -.09 | -.04 | -.09 | -.15 | -.09 | .02 | -.01 | -.15 | .12 | |||||||
| Infant and Mother Health | |||||||||||||||||||||
| 9. Infant Gender | - | .03 | .01 | -.05 | .09 | -.03 | -.03 | .03 | .01 | -.03 | .10 | .03 | .12 | ||||||||
| 10. Gestational Age | - | .50 | -.07 | -.06 | .06 | .02 | -.11 | -.07 | .03 | .07 | .04 | -.18 | |||||||||
| 11. Birth Weight | - | -.04 | -.03 | -.05 | .06 | -.08 | -.03 | .03 | .28 | .20 | -.12 | ||||||||||
| 12. 5 Minute APGAR | - | -.26 | .05 | .06 | .02 | -.02 | .08 | .10 | .09 | -.03 | |||||||||||
| 13. # Days in Hospital | - | -.02 | -.04 | -.03 | .08 | -.03 | .09 | .02 | -.03 | ||||||||||||
| 14. Mother Medical Condition | - | .00 | .00 | -.11 | .08 | .01 | -.36 | -.13 | |||||||||||||
| Key Study Variables | |||||||||||||||||||||
| 15. HSI family stress | - | .22 | .22 | -.03 | -.11 | .26 | -.03 | ||||||||||||||
| 16. Temperamental Surgency | - | .42 | -.05 | -.06 | .04 | -.04 | |||||||||||||||
| 17. Temperamental Negativity | - | -.03 | -.26 | .03 | -.15 | ||||||||||||||||
| 18. Maternal Sensitivity | - | -.04 | -.03 | .12 | |||||||||||||||||
| 19. Self-Comforting Behaviors | - | .08 | -.08 | ||||||||||||||||||
| 20. Orienting Behaviors | - | -.21 | |||||||||||||||||||
| 21. Change in Distress | - | ||||||||||||||||||||
Note. Bolded values are significant at the p<.05 level. Pairwise deletion was used; n's ranged from 41 to 295. Variables were coded as follows: Country of origin, 0=US, l=Other; Preferred Language, 0=English, l=Spanish; Marital Status, 0=Married or Living together, l=other; Infant gender, 0=Boy, 1=Girl.
2.2. Regulatory Function of Self-Comforting and Orienting Behaviors
Small and moderately small effect sizes emerged for correlations between self-comforting and orienting behaviors and changes in infant displays of distress (see Table 2), though neither of these associations was statistically significant (see Figure 1). Discrepancies between observed p-values and effect sizes were likely due to the small numbers of microcoded data available for these analyses (n's=51, 52). Because p-values are highly sample size dependent and have been demonstrated to yield higher rates of Type II error in small samples, interpretation of effect sizes was deemed more appropriate for these analyses (Hubbard & Lindsay, 2008).
Figure 1.
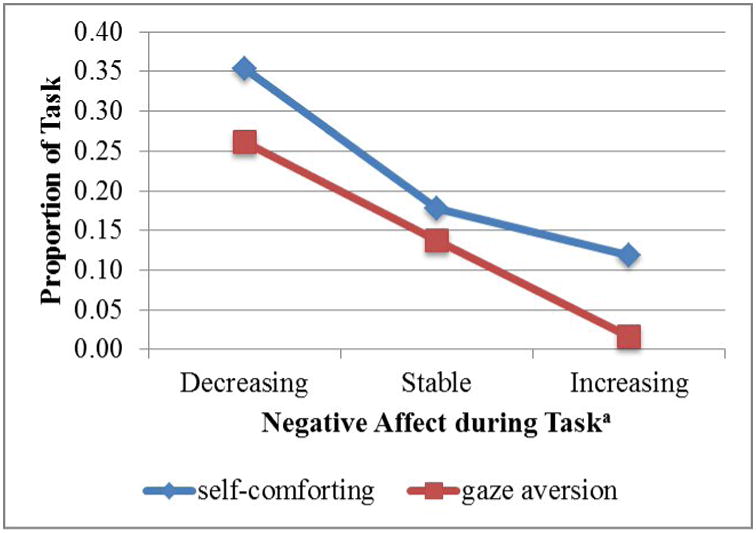
Infants' Engagement in Regulatory Strategies and Simultaneous Changes in Distress.
aInfants with positive change scores greater than one standard deviation above the mean were considered to experience escalations in distress across the interaction task; infants with negative change scores less than one standard deviation below the mean were considered to experience reductions in distress; and infants with change scores within one standard deviation above or below the mean were said to maintain constant levels of distress throughout the interaction.
2.3. Direct and Indirect Relations between Prenatal Stress and Infant Regulation
The full SEM model examined the direct paths between prenatal stress and infant regulatory behaviors at 12 weeks, as well as the indirect pathways through infant temperament and maternal sensitivity at 6 weeks (see Figure 2). Covariances between each of the mediating variables, as well as between both of the regulatory behaviors, were also estimated in the full model, but only significant covariances are shown for readability. Goodness of fit tests indicated that the full model fit the data well: χ2 (14) = 17.50, p = .23; RMSEA=.03; CFI = .97; SRMR = .04. The model was also run in Maximum Likelihood Robust to correct for non-normality (Yuan & Bentler, 2000). However, because results were not substantially different, results from the initial analyses are presented here.
Figure 2.

Model Results. Standardized estimates shown are above; only significant paths are shown here for readability. Mother's preferred language (β=-.151, p=.008) was entered as a covariate. The full model estimated covariations between each of the mediating variables as well as between the regulatory behaviors, but only significant covariations are shown here. Maternal sensitivity was not significantly predicted by prenatal stress, did not predict either of the regulatory behaviors, and did not significantly covary with any of the mediating variables. Alpha significance is notated as follows: * p < .05, ** p < .01, *** p < .001.
Prenatal stress was significantly and positively related to infant orienting behaviors at infant 12 weeks of age, but not to infant self-comforting behaviors. Prenatal stress also showed significant, positive prediction to both infant temperamental negativity and surgency at infant 6 weeks of age. Infant surgency, however, was not significantly associated with infant self-comforting or orienting behaviors. Infant negativity showed a significant, negative relation with self-comforting, but no relation to orienting behaviors. Although maternal sensitivity at 6 weeks was not directly related to either infant self-comforting or orienting behaviors at 12 weeks, a significant interaction between maternal sensitivity and infant surgency emerged in the prediction of later orienting behaviors. Because significant paths were found that linked prenatal stress, infant negativity at 6 weeks, and infant engagement in self-comforting behaviors at 12 weeks, additional mediation analyses were conducted using bootstrapping with 2000 iterations in Mplus 6.12. Results from the bootstrapping analyses indicated that the indirect effect was not significant (95% CI [-.03, .01]).
2.4. Interaction between Maternal Sensitivity and Infant Surgency
The interaction between maternal sensitivity and surgency in the prediction of infant orienting behaviors was further probed using simple slope analyses in Mplus 6.12 using the model constraint command. Simple slopes of the relations between surgency and orienting were estimated at the mean, as well as at one standard deviation above and below the mean of maternal sensitivity, following steps described in Aiken and West (Aiken & West, 1991). A plot of the simple slopes for the interaction between maternal sensitivity and infant surgency is displayed in Figure 3. Infant surgency was a significant and negative predictor of orienting behaviors at low levels of maternal sensitivity (β = -0.13, p =.02), but not at high levels (β = 0.07, p =.12) or mean levels of maternal sensitivity (β = -0.03, p =.40).
Figure 3.
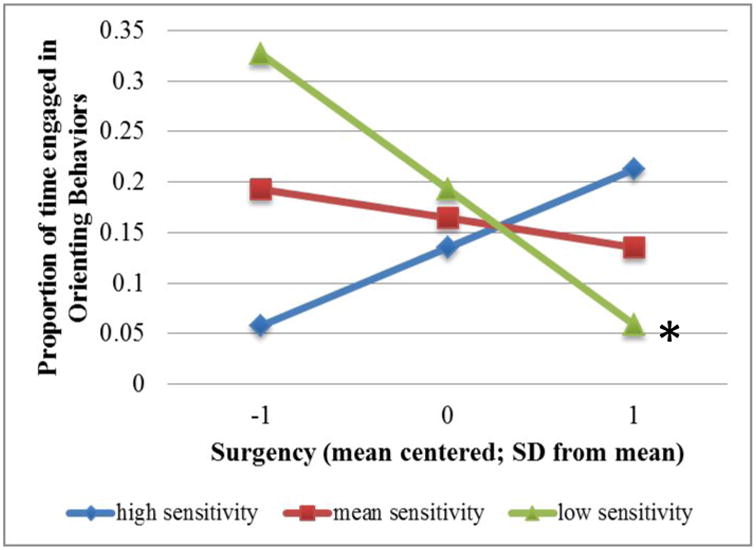
Relations between Maternal Sensitivity, Infant Surgency, and Orienting Behaviors.
*Alpha significance was at the p < .05 level.
3. Discussion
The current study investigated infant and mother characteristics contributing to the development of self-regulation across the first 12 weeks of life in a low-income, Mexican American sample. Findings support the notion that infants are capable of initiating behaviors to modulate distress as early as 12 weeks postpartum. Further, exposure to maternal prenatal stress may exert cascades of influence on infants' regulatory capacity, both by influencing orienting regulatory behaviors and dispositional characteristics that confer risk for later regulatory difficulties.
3.1. Regulatory Function of Self-Comforting and Orienting Behaviors
Self-comforting and orienting behaviors were expected to serve regulatory functions, such that more engagement in those behaviors would predict decreases in distress across the same interaction task. The associations between each of the putative regulatory behaviors and changes in distress achieved small and moderately small effects by Cohen's norms. Specifically, the more time infants engaged in either self-comforting or orienting behaviors, the more likely they were to experience decreasing levels of distress across the task. These trends are consistent with the extant literature and further extend the regulatory value of self-comforting and orienting behaviors to infants as young as three months old. For example, Crockenberg & Leerkes (2004) found that 6-month-old infants' orienting and self-comforting behaviors were observed more often during periods of decreasing distress. Similarly, Field (1981) found that 4-month-old infants looked away from their mothers when they became more aroused (i.e., increased heart rate), and looking away in turn helped to reduce arousal.
3.2. Maternal Prenatal Stress and Infant Regulatory Behaviors
Prenatal stress was expected to predict less engagement in self-comforting and orienting regulatory behaviors, but these relations were hypothesized to be fully mediated by infant temperamental negativity and surgency; this hypothesis was only partially supported. Prenatal stress was linked with infants' engagement in both self-comforting and orienting behaviors, but the paths linking prenatal stress and each of the regulatory behaviors varied in nature and in direction, suggesting that relations between prenatal stress and infant regulation are complex.
3.2.1. Self-comforting behaviors
Paths linking prenatal stress, infant temperamental negativity, and subsequent engagement in self-comforting behaviors suggested that infant exposure to prenatal stress predicted greater infant negativity, which predicted less engagement in self-comforting behaviors. These findings are consistent with other studies that have drawn links between prenatal stress and infant negativity (Huizink, et al., 2002); and infant negativity and impaired regulatory capacity (Calkins, et al., 2002). Moreover, that these relations emerged in the same study provides initial evidence to suggest that influences of prenatal stress on infant negativity may be one mechanism through which prenatal stress may compromise infant regulatory functions.
However, bootstrapping tests of the total indirect effect did not reach statistical significance for the mediated effect. One possible explanation for intermediate pathways of influence in the absence of a mediated effect may be that the observed relations between prenatal stress, infant negativity, and infant regulatory behaviors are better explained by their ties to some unmeasured fourth variable not considered here. For example, the fetal programming hypothesis posits that fetal exposure to excess maternal glucocorticoids may interfere with the normal development of infants' physiological stress response system (Seckl, 2001). Indeed, maternal prenatal stress has been found to predict infant physiological dysregulation (McCormick, Smythe, Sharma, & Meaney, 1995; Tollenaar, Beijers, Jansen, Riksen-Walraven, & de Weerth, 2011), and physiological dysregulation to predict infant emotional reactivity (Fortunato, Dribin, Granger, & Buss, 2008). It is conceivable that physiological dysregulation may also impede infants' abilities to coordinate motoric actions necessary for enlisting self-comforting behaviors. However, the extent to which prenatal stress may predict unique or shared variance in physiological and temperamental reactivity remains to be explicated, as well as the extent to which physiological reactivity may impede infants' engagement in regulatory behaviors.
3.2.2. Orienting Behaviors
Prenatal stress appeared to have both direct and cascading influences on infant orienting, as infants exposed to greater levels of prenatal stress engaged in more orienting at twelve weeks, but also showed greater temperamental surgency. The finding that prenatal stress predicted more engagement in orienting behaviors was surprising and contrasted with previous research suggesting that exposure to prenatal stress predicts lower durations of orienting and less attentional control in general (Huizink, et al., 2002; Lundy, et al., 1999). One conceivable explanation for these anomalous findings might be that infant attentional control may have benefitted from exposure to the moderate levels of stress reported in the current sample. Although few or no studies have found benefits of exposure to prenatal stress specific to infants' attentional control, some studies of low-risk samples have yielded findings suggestive that exposure to mild and moderate levels of distress may child developmental outcomes (e.g., DiPietro, Novak, Costigan, Atella, & Reusing, 2006). However, because this was the only anomalous finding that emerged from this study and because higher levels of prenatal stress also predicted greater temperamental risk, the suggestion that prenatal stress may enhance regulatory function in this high-risk sample should be considered with caution. Further studies investigating these relations within high-risk samples are needed.
It is also possible that other protective postnatal environmental factors not captured in the current study mediated the positive relations between prenatal stress and orienting behaviors. For example, researchers puzzled by similarly unexpected findings of better birth outcomes among high-risk Mexican American mothers relative to their White counterparts have suggested the presence of an “epidemiological paradox”, in which factors associated with enculturation in Mexican culture are believed to protect infants against the multiple risk factors they experience (Jahromi, Umaña-Taylor, Updegraff, & Lara, 2012; Padilla, Hamilton, & Hummer, 2009). Additional caregiving and/or cultural factors both in the prenatal and postnatal environment that may help to counteract the deleterious effects of prenatal stress or even promote infants' attentional control remain to be identified.
A cascading pathway of influence linking prenatal stress, infant temperamental surgency, and orienting behaviors also emerged. Similar to the results for self-comforting, exposure to more prenatal stress predicted more temperamental surgency, which in turn influenced subsequent orienting behaviors. Though it may seem counterintuitive at first that exposure to prenatal stress would predict a temperamental characteristic encompassing positive mood, surgency more accurately captures a quality of positive reactivity, which comprises both elements of positive mood and activity level. Though no research has examined relations between prenatal stress and infant surgency, some studies have found links between prenatal stress and fetal activity in-utero. In fact, fetuses of depressed mothers are nearly twice as active as those of non-depressed mothers (Dieter, et al., 2001). Relations between fetal activity and subsequent activity level are unclear, yet. Nonetheless, the positive associations between prenatal stress and higher levels of both infant negative and positive reactivity may reflect influences of prenatal stress on of infant general reactivity that is reflected in both temperamental negativity and surgency.
Evidence suggestive of a shared underlying reactivity component between negativity and surgency is growing. Studies that have addressed the connection between surgency and physiological reactivity have paralleled those that have emerged between negativity and physiological reactivity, with both negativity and surgency predicting heightened physiological reactivity (Davis, Donzella, Krueger, & Gunnar, 1999; Donzella, Gunnar, Krueger, & Alwin, 2000). Moreover, negativity and surgency have similarly been implicated as risk factors for externalizing behavior problems (Martel, Gremillion, & Roberts, 2012). It is feasible that negativity and surgency may share an underlying physiological reactivity component—a component that may be heightened in infants prenatally exposed to stress.
3.3. Interactions between Maternal Sensitivity and Infant Surgency
In contrast to direct relations that emerged between negativity and self-comforting behaviors, surgency was not directly related to orienting, but rather interacted with maternal sensitivity to predict varying levels of orienting. As predicted, infants high in surgency engaged in more orienting at higher levels of maternal sensitivity, and less orienting at lower levels of maternal sensitivity compared to their low-surgency counterparts. An unexpected finding was that infants lower in surgency engaged in less orienting at high levels of maternal sensitivity, and the most orienting at low levels of maternal sensitivity. These findings may reflect true relations between orienting regulation and maternal sensitivity for infants lower in surgency, or may alternatively be capturing their lower thresholds for high intensity stimulation. Specifically, infant regulatory behaviors were assessed in the context of a dyadic interaction task that may have elicited the most distress when mothers engaged in more overstimulating or intrusive behaviors (i.e., when mothers were less sensitive to infants' needs for stimulation). In this case, it is conceivable that the moderately high levels of orienting away behaviors observed in high sensitivity-high surgency mother-infant dyads reflected the regulatory agility of infants engaged in interaction with their mothers, whereas the very high levels of orienting away behaviors observed in low sensitivity-low surgency dyads reflected infant general disengagement from their overly stimulating mothers. It may be important for future studies considering infant orienting behaviors to distinguish between different forms of orienting away behaviors (i.e., gaze aversion, disengagement, distractibility, etc.) and to interpret their meanings in the contexts within which they are observed.
3.4. Study Limitations
Although there were multiple design and methodological strengths, several limitations should be noted. Infant regulatory behaviors were assessed in the context of a dyadic interaction task, and accuracy in measuring infants' capacities to regulate through distress was contingent on infants' experience of distress during a task otherwise intended to promote pleasurable dyadic interaction. Moreover, because infant orienting was defined as infant looking away from mother or task-related objects, purposeful gaze aversions with regulatory intent could not easily be distinguished from the infants' general lack of interest or inability to focus gaze in social interactions with their mothers. Future studies should consider infants' engagement in regulatory behaviors in infant-only tasks designed to elicit frustration, or explore contrasts between infants' purposeful gaze aversion and other looking away behaviors.
Another limitation was that because assessments of maternal postnatal family stress were not obtained at the 6-week time point, the current study could not control for and rule out the possibility that observed effects were a function of maternal postnatal, and not prenatal stress. However, other studies have found that influences of prenatal stress hold even after controlling for maternal postnatal stress (Huizink, et al., 2002). Related, it is important to note that both assessments of maternal prenatal stress and infant temperament were obtained via mother self-report, and thus could possibly reflect a negative reporting bias. However likewise, other studies have found that indices of prenatal stress predict both mother- and observer-reports of infant temperament (Huizink, et al., 2002). Finally, because the current study did not include indices of maternal temperament, personality, or genetic contribution, genetic transmission of negativity and/or surgency cannot be ruled out as explanation for associations between prenatal stress and infant temperament. Studies on the heritability of temperament have suggested that anywhere from 50 to 80% of variation in parents' reports of children's temperament may be attributable to genes (Goldsmith, Gottesman, & Lemery, 1997). Nonetheless, studies examining influences of prenatal stress on infant developmental outcomes have found relations even in unrelated mother-infant dyads (Rice, et al., 2010).
3.5. Summary and Conclusions
The current study provides evidence that maternal stress may exert cascades of influence on infants' developmental and mental health outcomes in a sample of Mexican American mother-infant dyads. Study findings were suggestive that prenatal stress may exert influences on infants' general reactivity, as reflected both in higher levels of infant temperamental negativity and surgency. However, the extent to which such connections converge or diverge over time remains to be clarified. The anomalous finding that prenatal stress was associated with higher levels of infant orienting warrants further exploration, especially to consider possible protective and/or promotive influences of postnatal factors not considered here. Advancing knowledge about the extent to which prenatal stress may exert both negative and positive cascades of influence on infant developmental outcomes may lend important information for the targets of intervention in this high-risk sample.
Highlights.
Prenatal stress exerts direct and indirect effects on infant regulatory behaviors.
Prenatal stress predicted more temperamental negativity and surgency at 6 weeks.
Infant negativity predicted more self-comforting at 12 weeks.
Infant surgency and maternal sensitivity (6 wks) predict orienting (12 wks).
Acknowledgments
This study was funded by the National Institute of Mental Health (R01 MH083173-01). Special thanks to the mothers and infants who participated in the project, as well as to Kathryn Lemery-Chalfant and David MacKinnon, whose thoughtful feedback helped to advance the conceptual and methodological development of this study.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA, US: Sage Publications, Inc; 1991. [Google Scholar]
- Ainsworth MDS, Blehar MC, Waters E, Wall S. Patterns of attachment: A psychological study of the strange situation. Oxford, England: Lawrence Erlbaum; 1978. [Google Scholar]
- Allison PD. Missing Data Techniques for Structural Equation Modeling. The Journal of Abnormal Psychology. 2003;112:545–557. doi: 10.1037/0021-843X.112.4.545. [DOI] [PubMed] [Google Scholar]
- Althoff RR, Verhulst FC, Rettew DC, Hudziak JJ, van der Ende J. Adult outcomes of childhood dysregulation: A 14-year follow-up study. Journal of the American Academy of Child & Adolescent Psychiatry. 2010;49:1105–1116. doi: 10.1016/j.jaac.2010.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belsky J. Variation in susceptibility to environmental influence: An evolutionary argument. Psychological Inquiry. 1997;8:182–186. [Google Scholar]
- Belsky J, Crnic K, Gable S. The determinants of coparenting in families with toddler boys: Spousal differences and daily hassles. Child Development. 1995;66:629–642. [PubMed] [Google Scholar]
- Braungart-Rieker JM, Hill-Soderlund AL, Karrass J. Fear and anger reactivity trajectories from 4 to 16 months: The roles of temperament, regulation, and maternal sensitivity. Developmental Psychology. 2010;46:791–804. doi: 10.1037/a0019673. [DOI] [PubMed] [Google Scholar]
- Calkins SD. Origins and outcomes of individual differences in emotion regulation. Monographs of the Society for Research in Child Development. 1994;59:53–72. 250–283. [PubMed] [Google Scholar]
- Calkins SD, Dedmon SE, Gill KL, Lomax LE, Johnson LM. Frustration in infancy: Implications for emotion regulation, physiological processes, and temperament. Infancy. 2002;3:175–197. doi: 10.1207/S15327078IN0302_4. [DOI] [PubMed] [Google Scholar]
- Cauce AM, Cruz R, Corona M, Conger R. Health disparities in youth and families: Research and applications. New York, NY, US: Springer Science + Business Media, New York, NY; 2011. The face of the future: Risk and resilience in minority youth; pp. 13–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cervantes RC, Padilla AM, Salgado de Snyder N. Reliability and validity of the Hispanic Stress Inventory. Hispanic Journal of Behavioral Sciences. 1990;12:76–82. [Google Scholar]
- Cervantes RC, Padilla AM, Salgado de Snyder N. The Hispanic Stress Inventory: A culturally relevant approach to psychosocial assessment. Psychological Assessment: A Journal of Consulting and Clinical Psychology. 1991;3:438–447. [Google Scholar]
- Cohen J, Cohen P, West SG, Aiken LS. Applied multiple regression/correlation analysis for the behavioral sciences. 3rd. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers; 2003. [Google Scholar]
- Cohn JF, Tronick EZ. Mother-Infant Face-to-Face Interaction: The Sequence of Dyadic States at 3, 6, and 9 Months. Developmental Psychology. 1987;23:68-68–77. [Google Scholar]
- Conradt E, Ablow J. Infant physiological response to the still-face paradigm: Contributions of maternal sensitivity and infants' early regulatory behavior. Infant Behavior & Development. 2010;33:251–265. doi: 10.1016/j.infbeh.2010.01.001. [DOI] [PubMed] [Google Scholar]
- Crockenberg SC, Leerkes EM. Infant and Maternal Behaviors Regulate Infant Reactivity to Novelty at 6 Months. Developmental Psychology. 2004;40:1123–1132. doi: 10.1037/0012-1649.40.6.1123. [DOI] [PubMed] [Google Scholar]
- Davis EP, Donzella B, Krueger WK, Gunnar MR. The start of a new school year: Individual differences in salivary cortisol response in relation to child temperament. Developmental Psychobiology. 1999;35:188–196. doi: 10.1002/(sici)1098-2302(199911)35:3<188::aid-dev3>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- Dieter JNI, Field T, Hernandez-Reif M, Jones NA, Lecanuet JP, Salman FA, Redzepi M. Maternal depression and increased fetal activity. Journal of Obstetrics & Gynaecology. 2001;21:468–473. doi: 10.1080/01443610120072009. [DOI] [PubMed] [Google Scholar]
- DiPietro JA, Novak MFSX, Costigan KA, Atella LD, Reusing SP. Maternal Psychological Distress During Pregnancy in Relation to Child Development at Age Two. Child Development. 2006;77:573–587. doi: 10.1111/j.1467-8624.2006.00891.x. [DOI] [PubMed] [Google Scholar]
- Donzella B, Gunnar MR, Krueger WK, Alwin J. Cortisol and vagal tone responses to competitive challenge in preschoolers: Associations with temperament. Developmental Psychobiology. 2000;37:209–220. doi: 10.1002/1098-2302(2000)37:4<209::aid-dev1>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Liew J, Pidada SU. The Longitudinal Relations of Regulation and Emotionality to Quality of Indonesian Children's Socioemotional Functioning. Developmental Psychology. 2004;40:790–804. doi: 10.1037/0012-1649.40.5.790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Valiente C, Spinrad TL, Cumberland A, Liew J, Reiser M, Zhou Q, Losoya SH. Longitudinal relations of children's effortful control, impulsivity, and negative emotionality to their externalizing, internalizing, and co-occurring behavior problems. Developmental Psychology. 2009;45:988–1008. doi: 10.1037/a0016213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK. Applied missing data analysis. Guilford Press; New York, NY: 2010. [Google Scholar]
- Feldman R. The relational basis of adolescent adjustment: Trajectories of mother-child interactive behaviors from infancy to adolescence shape adolescents' adaptation. Attachment & Human Development. 2010;12:173-173–192. doi: 10.1080/14616730903282472. [DOI] [PubMed] [Google Scholar]
- Feldman R, Greenbaum CW, Yirmiya N. Mother–infant affect synchrony as an antecedent of the emergence of self-control. Developmental Psychology. 1999;35:223–231. doi: 10.1037//0012-1649.35.1.223. [DOI] [PubMed] [Google Scholar]
- Field T. Infant gaze aversion and heart rate during face-to-face interactions. Infant Behavior & Development. 1981;4:307–315. [Google Scholar]
- Field T. Sucking and massage therapy reduce stress during infancy. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers; 1999. [Google Scholar]
- Fortunato CK, Dribin AE, Granger DA, Buss KA. Salivary alpha-amylase and cortisol in toddlers: Differential relations to affective behavior. Developmental Psychobiology. 2008;50:807–818. doi: 10.1002/dev.20326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gartstein, M. A. (2011). e-mail. In K. Lemery-Chalfant (Ed.), (e-mail communication ed.).
- Gartstein MA, Rothbart MK. Studying infant temperament via the revised infant behavior questionnaire. Infant Behavior & Development. 2003;26:64–86. [Google Scholar]
- Gartstein MA, Slobodskaya HR, Putnam SP, Kinsht IA. A cross-cultural study of infant temperament: Predicting preschool effortful control in the United States of America and Russia. European Journal of Developmental Psychology. 2009;6:337–364. [Google Scholar]
- Goldsmith HH, Gottesman II, Lemery KS. Epigenetic approaches to developmental psychopathology. Development and Psychopathology. 1997;9:365–387. doi: 10.1017/s0954579497002095. [DOI] [PubMed] [Google Scholar]
- Goodkind JR, Gonzales M, Malcoe LH, Espinosa J. The Hispanic Women's Social Stressor Scale: Understanding the multiple social stressors of U.S.- and Mexico-born Hispanic women. Hispanic Journal of Behavioral Sciences. 2008;30:200–229. [Google Scholar]
- Graham JW, Taylor BJ, Olchowski AE, Cumsille PE. Planned missing data designs in psychological research. Psychological Methods. 2006;11:323–343. doi: 10.1037/1082-989X.11.4.323. [DOI] [PubMed] [Google Scholar]
- Gress-Smith JL, Luecken LJ, Lemery-Chalfant K, Howe R. Postpartum depression prevalence and impact on infant health, weight, and sleep in low-income and ethnic minority women and infants. Maternal and Child Health Journal. 2012;16:887–893. doi: 10.1007/s10995-011-0812-y. [DOI] [PubMed] [Google Scholar]
- Gutteling BM, de Weerth C, Willemsen-Swinkels SHN, Huizink AC, Mulder EJH, Visser GHA, Buitelaar JK. The effects of prenatal stress on temperament and problem behavior of 27-month-old toddlers. European Child & Adolescent Psychiatry. 2005;14:41–51. doi: 10.1007/s00787-005-0435-1. [DOI] [PubMed] [Google Scholar]
- Haith MM, McCarty ME. Stability of visual expectations at 3.0 months of age. Developmental Psychology. 1990;26:68–74. [Google Scholar]
- Hu Lt, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Hubbard R, Lindsay RM. Why P Values Are Not a Useful Measure of Evidence in Statistical Significance Testing. Theory & Psychology. 2008;18:69–88. [Google Scholar]
- Huizink AC, Robles de Medina PG, Mulder EJH, Visser GHA, Buitelaar JK. Psychological measures of prenatal stress as predictors of infant temperament. Journal of the American Academy of Child & Adolescent Psychiatry. 2002;41:1078–1085. doi: 10.1097/00004583-200209000-00008. [DOI] [PubMed] [Google Scholar]
- Jahromi LB, Umaña-Taylor AJ, Updegraff KA, Lara EE. Birth characteristics and developmental outcomes of infants of Mexican-origin adolescent mothers: Risk and promotive factors. International Journal of Behavioral Development. 2012;36:146–156. doi: 10.1177/0165025411430777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lundy BL, Jones NA, Field T, Nearing G, Davalos M, Pietro PA, Schanberg S, Kuhn C. Prenatal depression effects on neonates. Infant Behavior & Development. 1999;22:119–129. [Google Scholar]
- Martel MM, Gremillion ML, Roberts B. Temperament and common disruptive behavior problems in preschool. Personality and Individual Differences. 2012;53:874–879. doi: 10.1016/j.paid.2012.07.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCormick CM, Smythe JW, Sharma S, Meaney MJ. Sex-specific effects of prenatal stress on hypothalamic-pituitary-adrenal responses to stress and brain glucocorticoid receptor density in adult rats. Developmental Brain Research. 1995;84:55–61. doi: 10.1016/0165-3806(94)00153-q. [DOI] [PubMed] [Google Scholar]
- Molfese VJ, Rudasill KM, Beswick JL, Jacobi-Vessels JL, Ferguson MC, White JM. Infant temperament, maternal personality, and parenting stress as contributors to infant developmental outcomes. Merrill-Palmer Quarterly: Journal of Developmental Psychology. 2010;56:49–79. [Google Scholar]
- Morales M, Mundy P, Crowson MM, Neal AR, Delgado CEF. Individual differences in infant attention skills, joint attention, and emotion regulation behaviour. International Journal of Behavioral Development. 2005;29:259–263. [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. 6. Los Angeles: Muthén & Muthén; 2010. [Google Scholar]
- O'Connor TG, Caprariello P, Blackmore ER, Gregory AM, Glover V, Fleming P. Prenatal mood disturbance predicts sleep problems in infancy and toddlerhood. Early Human Development. 2007;83:451-451–458. doi: 10.1016/j.earlhumdev.2006.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Padilla YC, Hamilton ER, Hummer RA. Beyond the epidemiological paradox: The health of Mexican-American children at age Five. Social Science Quarterly. 2009;90:1072–1088. doi: 10.1111/j.1540-6237.2009.00647.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Posner MI, Rothbart MK. Developing mechanisms of self-regulation. Development and Psychopathology. 2000;12:427–441. doi: 10.1017/s0954579400003096. [DOI] [PubMed] [Google Scholar]
- Rice F, Harold GT, Boivin J, van den Bree M, Hay DF, Thapar A. The links between prenatal stress and offspring development and psychopathology: Disentangling environmental and inherited influences. Psychological Medicine: A Journal of Research in Psychiatry and the Allied Sciences. 2010;40:335–345. doi: 10.1017/S0033291709005911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothbart MK. Becoming Who We Are: Temperament and Personality in Development. New York: Guilford Publications; 2011. [Google Scholar]
- Rothbart MK, Derryberry D, Hershey K. Stability of temperament in childhood: Laboratory infant assessment to parent report at seven years. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers; 2000. [Google Scholar]
- Rothbart MK, Ziaie H, O'Boyle CG. Self-regulation and emotion in infancy. San Francisco, CA, US: Jossey-Bass; 1992. [DOI] [PubMed] [Google Scholar]
- Rubin DB. Inference and missing data. Biometrika. 1976;63:581–592. [Google Scholar]
- Ruff HA, Rothbart MK. Attention in early development: Themes and variations. New York, NY, US: Oxford University Press; 1996. [Google Scholar]
- Sander LW, Julia HL, Stechler G, Burns P. Continuous 24-hour interactional monitoring in infants reared in two caretaking environments. Psychosomatic Medicine. 1972;34:270–282. doi: 10.1097/00006842-197205000-00009. [DOI] [PubMed] [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Seckl JR. Glucocorticoid programming of the fetus; adult phenotypes and molecular mechanisms. Molecular and Cellular Endocrinology. 2001;185:61–71. doi: 10.1016/s0303-7207(01)00633-5. [DOI] [PubMed] [Google Scholar]
- Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods. 2002;7:422–445. [PubMed] [Google Scholar]
- Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Physical therapy. 2005;85:257–268. [PubMed] [Google Scholar]
- Stifter CA, Braungart JM. The regulation of negative reactivity in infancy: Function and development. Developmental Psychology. 1995;31:448–455. [Google Scholar]
- Tollenaar MSM, Beijers RR, Jansen JJ, Riksen-Walraven JMAJ, de Weerth CC. Maternal prenatal stress and cortisol reactivity to stressors in human infants. Stress (Amsterdam, Netherlands) 2011;14:53–65. doi: 10.3109/10253890.2010.499485. [DOI] [PubMed] [Google Scholar]
- Tronick E, Als H, Brazelton TB. Monadic phases: A structural descriptive analysis of infant–mother face to face interaction. Merrill-Palmer Quarterly: Journal of Developmental Psychology. 1980;26:3–24. [Google Scholar]
- Weinstock M. Does prenatal stress impair coping and regulation of hypothalamic-pituitary-adrenal axis? Neuroscience and biobehavioral reviews. 1997;21:1–10. doi: 10.1016/s0149-7634(96)00014-0. [DOI] [PubMed] [Google Scholar]
- Yuan KH, Bentler PM. Three Likelihood-Based Methods For Mean and Covariance Structure Analysis With Nonnormal Missing Data. Sociological Methodology. 2000;30:165–200. [Google Scholar]