

Abstract
Background:
National Health Insurance Scheme (NHIS) is one of the health financing options adopted by Nigeria for improved healthcare access especially to the low income earners. One of the key operators of the scheme is the health care providers, thus their uptake of the scheme is fundamental to the survival of the scheme. The study reviewed the uptake of the NHIS by private health care providers in a Local Government Area in Lagos State.
Objective:
To assess the uptake of the NHIS by private healthcare practitioners.
Materials and Methods:
This descriptive cross-sectional study recruited 180 private healthcare providers selected by multistage sampling technique with a response rate of 88.9%.
Result:
Awareness, knowledge and uptake of NHIS were 156 (97.5%), 110 (66.8%) and 97 (60.6%), respectively. Half of the respondents 82 (51.3%) were dissatisfied with the operations of the scheme. Major reasons were failure of entitlement payment by Health Maintenance Organisations 13 (81.3%) and their incurring losses in participating in the scheme 8(50%). There was a significant association between awareness, level of education, knowledge of NHIS and registration into scheme by the respondents P-value < 0.05.
Conclusions:
Awareness and knowledge of NHIS were commendable among the private health care providers. Six out of 10 had registered with the NHIS but half of the respondents 82 (51.3%) were dissatisfied with the scheme and 83 (57.2%) regretted participating in the scheme. There is need to improve payment modalities and ensure strict adherence to laid down policies.
Keywords: Knowledge, NHIS, private private healthcare providers, uptake
INTRODUCTION
The Nigerian Government took a definite step to establish a National Health Insurance Scheme (NHIS) in 1999 as a social tool towards attaining equity in health service delivery.1 A major increase in financial resources for health is needed to scale up health interventions and strengthen health delivery systems to ensure that these interventions are accessible, particularly for the poor.2 Health insurance scheme therefore holds the promise of ensuring a guaranteed pool of funds for health, improving the efficiency of management of health resources and protecting people against catastrophic expenditure for health.3 The uptake of the NHIS by healthcare providers and the beneficiaries is of crucial importance to the performance of the scheme. This informed the need to undertake a critical appraisal of the uptake of the scheme by these important stakeholders.
There have been different accounts of the uptake of the scheme by different stakeholders. However of importance is the uptake of the scheme by the health care providers who are the main operators of the scheme. In the South-East, Okaro et al study in 2010 reported that almost all the hospitals studied had registered with the scheme.4 Result from the study of Sanusi and Awe in 2009 showed that about 83% of the respondents have accepted the programme.5 However, the Olugbenga-Bello study of 2008 reported only 0.3%.6 and this is in contradistinction to the rate of uptake of the scheme in Lagos which increased from 4.5% in 2000 and 2003 to 13.6% in 2004, 27.6% in 2005 and 31.6% in 2006.7 The Federal mandate to the present NHIS administration is to achieve population coverage of 30% by 2015.8 This is in contrast to France which operates a health insurance policy that is compulsory.9 Ghana national health insurance act which was promulgated in 2003 with the aim of making health care available to all residents of Ghana recorded an uptake of 62% according to the 2009 annual report of the NHIS of Ghana. However, a decline of 34% in 2010 and 33% in 2011 were recorded in the respective annual NHIS Ghana reports.10,11,12
This study assessed the level of uptake of NHIS by private health care practitioners in a Local Government area of Lagos State. The objective was to assess the awareness, knowledge and uptake of NHIS among private health care providers.
MATERIALS AND METHODS
Multistage random sampling was used to recruit 180 participants with a response rate of 88.9% which was made up of 111 doctors and 49 nurses (160).
Stage 1
Stratification of health facilities into large (12), medium (127) and small (8) out of the 104 hospitals, 30 clinics and 26 maternity homes.
There were 12 big hospitals with an average of six healthcare providers (Doctors and Nurses), 127 medium hospitals with average of two healthcare providers (Doctors and Nurses) and eight small hospitals with average of two health care providers (only nurses). Total healthcare providers was (6 × 12) + (127 × 2) + (8 × 2) = 342.
Stage II
Proportionate allocation of sample to determine number of questionnaires for each stratum. This was calculated thus:

The estimated health care providers in all the health facilities were 342. For the Large health facility, the estimated number of health care providers was given as 72. The number interviewed was 72/342 × 160 = 34. The same procedure was carried out to obtain 119 for medium, and small gave 7 health facilities.
Stage III
Selection of health care facilities: All the large health facilities (12) were included in the study while 64 and 4 were randomly selected from medium and small health facilities respectively using simple random sampling by balloting.
Stage IV
Selection of participants: Simple random sampling was used to select eligible respondents using balloting until the desired numbers were obtained.
Scoring system
Overall knowledge of the study participants about NHIS was assessed using the 31 responses in the knowledge section of the questionnaire. After assessing normality to the score using histogram, the composite score was dichotomised using mean as a cut-off value so that higher value coded as 1 showing higher overall knowledge of NHIS.
A score of one was given to correct responses, zero being used for incorrect/do not know responses. Based on the mean score of the composite variable (mean = 19.5), the responses were categorised into good (score above mean value) and poor (score below mean value) knowledge of NHIS.
Data was analysed using Microsoft Excel and SPSS, and presented in tabular form, level of significance of results was tested using Chi-square, with P-value set at ≤0.05.
Ethical clearance was obtained from the Ethics and Research Committee of the Lagos University Teaching Hospital. All ethical research protocols were strictly adhered to.
RESULTS
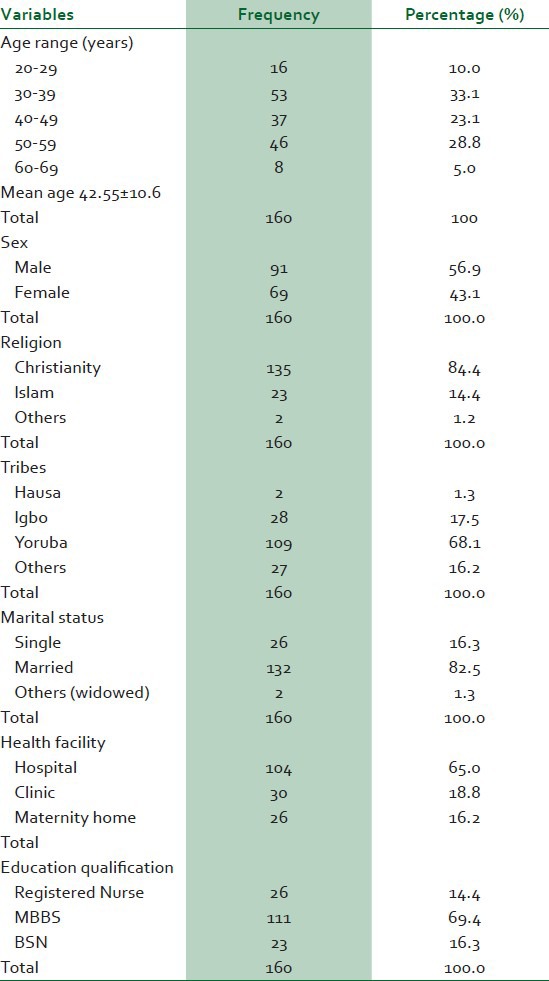
Up to 180 private health care practitioners were recruited into the study with a response rate of 88.9%. This predominantly Christian (135, 84.4%), married (132, 82.5%) respondents had a mean age of 42.55 ± 10.6 years. Majority (53, 33.1%) were of age 30-39 years. There were more males (91, 56.9%) than females and more doctors (111, 69.4%) than nurses [Table 1].
Table 1.
Socio-demographic characteristics of respondents
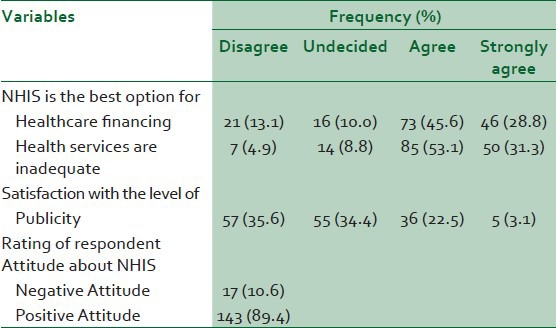
Almost all the respondents (97.5%) 156 had heard of NHIS, mainly through seminars and conferences (58.1%) 93; news papers (45.6%) 73; friends and colleagues (40.6%) 65 and television and radio (35%) 56. Up to 83.8% (134) cited funding, 60.0 % (96) insufficient health facilities, 48.8% (78) inadequate health manpower as the key problems meant to be addressed by the NHIS. Up to 95.6% (153) correctly indicated access to good healthcare, efficiency in healthcare services (68.8%) 110 and high quality of healthcare (62.5%) 100, as objectives of NHIS. More than half of the respondents 65.0% (104) and 61.9% (99) associated pooling of resources and sharing of risk with concepts of NHIS, respectively, 14.4% (23) with paying of tax and 30.6% (49) had no clue. As pertained to payment strategy, 68.1% (109) identified capitation, 23.8% (38) fee for service and 22.5% (36) case payment as provider payment mechanism. The overall knowledge was good as 68.8% of the respondents had good knowledge [Table 2]. A large proportion (74.4%) 119 believed that NHIS is the best healthcare financing option, 84.4% (135) agreed that healthcare services are inadequate in Nigeria. Up to 57 (35.6%) expressed dissatisfaction with level of NHIS publicity [Table 3].
Table 2.
Awareness and knowledge of NHIS among respondents
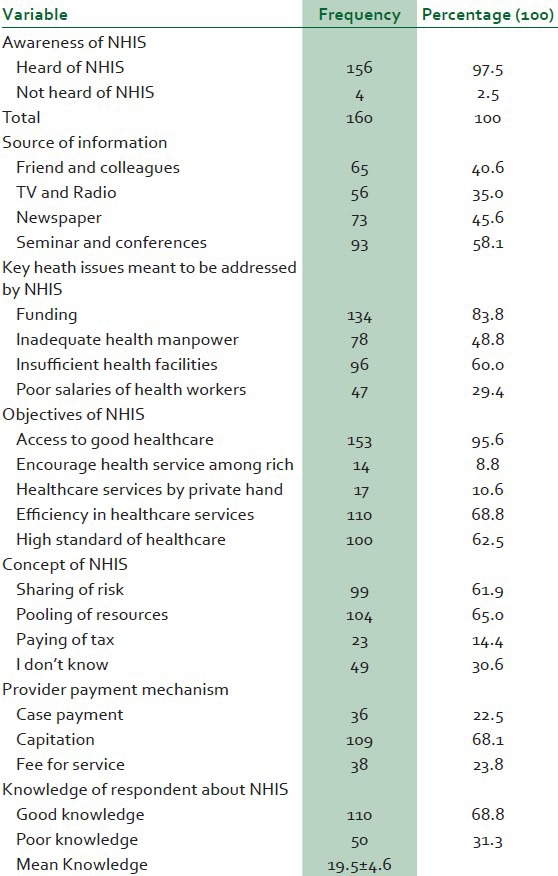
Table 3.
Attitudes toward NHIS among the respondents
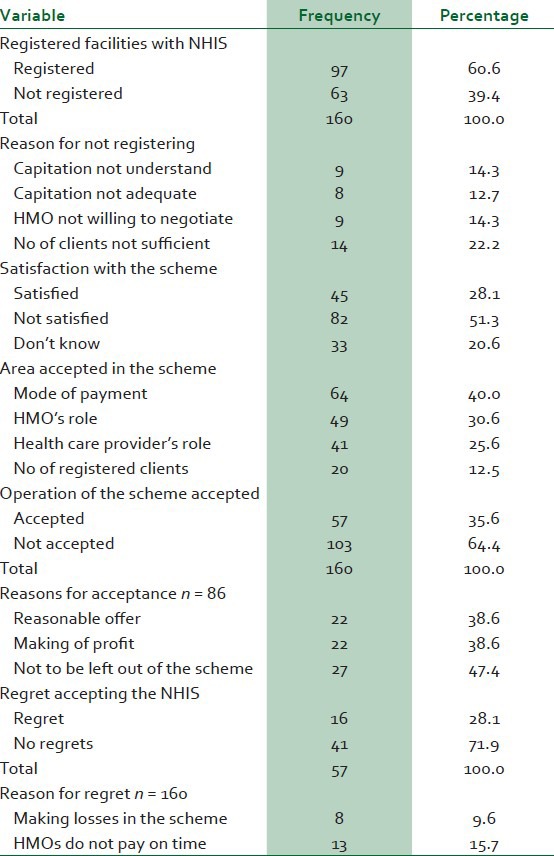
Almost two-third of the health facilities 97 (60.6%) had been registered with NHIS. Of the 63 (39.4%) that did not register, 9 (14.3%); 8 (12.7%) 14 (22.2%) cited capitation not understood; capitation not adequate and insufficient clients as reasons for not registering respectively. Almost one third 45 (28.1%) of the respondents were satisfied with the scheme. Fifty-seven (35.6%) accepted the operation of the scheme of which 16(28.1%) had regrets of accepting the NHIS. Reasons for regrets were making loses in the scheme 8(50.0%) and late payment by HMO13 (81.3%) [Table 4].
Table 4.
Uptake of NHIS among respondents
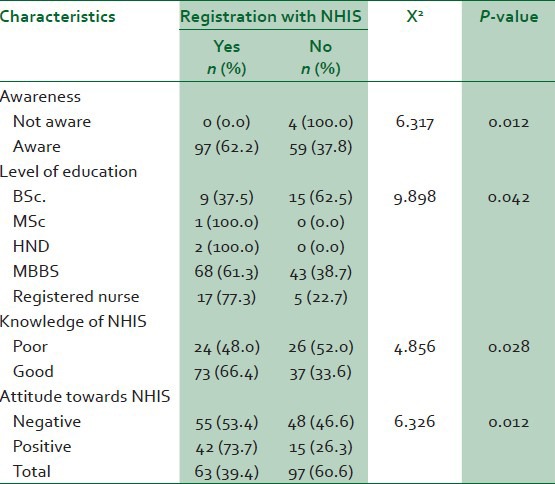
There was a statistically significant association between awareness, level of education, knowledge of NHIS, attitude and registration, P-value < 0.05 [Table 5].
Table 5.
Association between awareness of NHIS, educational qualification and registration
DISCUSSION
The sustainability and viability of a country's economic and social growth depend largely on vibrant healthcare sector of that nation, hence Nigerian National Health Insurance Scheme (NHIS) was launched with the major aim of improving accessibility and equity in healthcare delivery. This study revealed that 33.1% of respondents fell within the age bracket of 30-39 years. This implies that majority of respondents were within the (active age) working class of the population, relating closely with the 30-39 years (54%) obtained in Enugu study.4 The mean age of the respondents was 42.6 ± 10.6 years in line with the study subjects with active age group in the middle range.13 The high percentage of males (56.9%) in the study reflects the higher proportion of males in the parent population of study subjects (50.3%), as obtained by the 2005 National Population Census and the fact that men have traditionally constituted the bulk of the workforce, further buttressed by the 51.6% and 67.6% found in both Oyo and Enugu studies respectively.5,4,14 The above assertion is, however, not tantamount to 60.4% of respondents being females reported in the Minna study. An observation that can be attributed to 74.1% of respondents being nurses and/or midwives, a profession generally skewed towards the female gender.3 The married respondents of 82.5% obtained in this study is high, probably because the age bracket of the study is in reproductive age compared to 75.7% of Enugu study. The other demographic features of respondents also echo those of the parent population, with most (68.1%) being Yoruba by tribe and reverse for Christians (84.4%).14
The study revealed that 97.5% of the respondents had heard of the National Health Insurance Scheme. This is slightly close to a similar study in Enugu state carried out in 2009 by Okaro which showed an awareness level of 100%.4 This is as a result of the fact that the establishment of the scheme is almost running to 7 years now. Hence, awareness did translate to good uptake as many respondent 97 (60.6%) had registered with the scheme [Table 4]. There was a statistical significant association between awareness and registration of the scheme. The main sources of information were friends and colleagues 40.6%, radio/TV 35.0%, newspaper 45.6%, seminars and conferences 58.1%. Short intensive course of study (seminars and conferences) as the principal source of information about health insurance in this study is in contrast to the Niger and Lagos studies with 11.6% and 13.5%, respectively.15,16
Respondents in this study exhibited a high level of knowledge of NHIS. The knowledge of provider payment mechanism and capitation was higher (68.1%) than the studies in Niger and Osun states with 13.7% and 26.5%, respectively. The overall knowledge of the respondents in this study was high as demonstrated by the grading using the mean knowledge of 19.5 ± 4.6: good 110 (68.8%) and poor 50(31.3%) [Table 2].
The increasing trend of awareness to health insurance from the studies may be attributed to increased publicity of the NHIS following its formal launching in 2000 and commencement of operation in 2001.
Six out of 10 (60.6%) of the respondents in this study had registered with the scheme. This is slightly lower than a similar study by Sanusi and Awe in 2009 in Oyo state, where about 83% of the respondents were registered. Just about half (53.4%) accepted the operation of the scheme, and reasons for acceptance of the operation ranged from; reasonable offer (13.85), making of profit (13.87%) and not to be left out of the scheme (16.95%). However, as high as 57.2% expressed their regrets of accepting the scheme, major reasons for regret bordered on finance; in terms of failure of payment by HMOs (59.4%) and making losses in the scheme (30.6%).
CONCLUSION AND RECOMMENDATION
The study revealed that private healthcare providers in the Local Government Area were aware of the existence of NHIS in Nigeria. There was good demonstration of adequate knowledge with regards to principles of operation of health insurance scheme. However, more than half of the participants regretted keying into the scheme mainly due to late payment by HMOs and running the scheme at a loss. There is therefore need to improve the financial payment system.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Federal Government of Nigeria. National Health Insurance Scheme Decree No 35 of 1999 [Google Scholar]
- 2.WHO. Macro-economic and health: Investing in economic development. 2001. [Last cited on 2011 Feb 05]. Available from: http://who.int/macrohealth .
- 3.Osibogun AO, Ojo K. Com Health Nig Ltd; 2006. Health Insurance Schemes in Nigeria: Lesson from the Field; pp. 23–5. [Google Scholar]
- 4.Okaro AO, Ohagwu CC, Njoku J. Awareness and perception of National Health Insurance scheme (NHIS) among radiographers in south East Nigeria. Am J Sci Res. 2010:18–25. [Google Scholar]
- 5.Sanusi RA, Awe AT. An assessment of awareness level of NHIS among health consumers in Oyo State, Nigeria. Soc Sci J. 2009;4:143–8. [Google Scholar]
- 6.Olugbenga-Bello A, Adebimpe WO. Knowledge and attitudes of civil servants in Osun state, south West Nigeria towards the national health insurance scheme. Niger J Clin Pract. 2010;13:421–6. [PubMed] [Google Scholar]
- 7.Ibiwoye A, Adeleke AA. Vol. 33. WHO;The Geneva Papers; 2008. Does National Health insurance promote access to quality healthcare? pp. 219–33. [Google Scholar]
- 8.New secretary of NHIS vows to increase enrolment to above 30% [Last cited on Feb 5th 2014]. Available from: http://www.nhis.gov.ng .
- 9.Rodwin VG. The healthcare system under French national heath insurance: Lesons for health reform in the United States. Am J Public Health. 2003;91:31–7. doi: 10.2105/ajph.93.1.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.NHIS Annual Report of Ghana. 2009. [Last accessed on 2014 Feb 05]. Available from: http://www. Nhis.gov.gh .
- 11.NHIS Annual Report of Ghana 20010. [Last accessed on 2014 Feb 05]. Available from: http://www Nhis.gov.gh .
- 12.NHIS Annual Report of Ghana 20011. [Last accessed on 2014 Feb 05]. Available from: http://www Nhis.gov.gh .
- 13.Parks K. 21st ed. India: Banarsidas Bhanot Publishers; 20011. Park's Textbook of Preventive and Social Medicine; pp. 834–5. [Google Scholar]
- 14.Monitoring and evaluation office Alimosho primary health care centre. Alimosho LGA Lagos state Nigeria. Publication of the list of health care providers in Alimosho LGA Lagos state. 2011 Feb 5;:1–5. Obtained. [Google Scholar]
- 15.Sabitu K, James H. Attitudes and opinions of health-care providers in Minna town towards the NHIS. Ann Med. 2005;2:9–13. [Google Scholar]
- 16.Awosobi A. Knowledge, Attitude and Perception of NHIS among private HCPs in Surban LGAs of Lagos. A Master degree Project. 2008:7–8. [Google Scholar]