

Abstract
Objective:
Different additives have been used to prolong brachial plexus block. We evaluated the effect of adding magnesium sulfate to ropivacaine for supraclavicular brachial plexus blockade. The primary endpoints were the onset and duration of sensory and motor block and duration of analgesia.
Methods:
One hundred patients (25–55 years) posted for elective forearm and hand surgeries under supraclavicular brachial plexus block were divided into two equal groups (Groups RM and RN) in a randomized, double-blind fashion. In group RM (n = 50), 30 ml 0.5% ropivacaine plus 150 mg (in 1 ml 0.9% saline) magnesium sulfate and in group RN (n = 50), 30 ml 0.5% ropivacaine plus 1 ml normal saline were administered in supraclavicular block. Sensory and motor block onset times and block durations, time to first analgesic use, total analgesic need, postoperative visual analog scale (VAS), hemodynamic variables, and side effects were recorded for each patient.
Findings:
Though with similar demographic profile and block (sensory and motor) onset time, the sensory and motor block duration and time to first analgesic use were significantly longer and the total need for rescue analgesics was lower in group RM (P = 0.026) than group RN. Postoperative VAS values at 24 h were significantly lower in group RM (P = 0.045). Intraoperative hemodynamics was comparable among two groups and no appreciable side effect was noted throughout the study period.
Conclusion:
It can be concluded from this study that adding magnesium sulfate to supraclavicular brachial plexus block may increase the sensory and motor block duration and time to first analgesic use, and decrease total analgesic needs, with no side effects.
Keywords: Magnesium sulfate, Ropivacaine, supraclavicular brachial plexus block
INTRODUCTION
In modern anesthesia practice, peripheral nerve block has a significant contributory role. Safety and unparalleled success rate have made this technique of anesthesia as very popular in ambulatory and inpatient anesthesia. Upper limb surgeries below the shoulder joint are mostly performed under peripheral blocks such as the brachial plexus block. Peripheral nerve blocks not only provide intraoperative anesthesia but also extend analgesia in the postoperative period without major systemic side effects by minimizing stress response and using minimal anesthetic drugs.[1]
Ropivacaine is an aminoamide local anesthetic that blocks the peripheral afferents acting on voltage dependent sodium channels. It is less cardiac and central nervous system (CNS) toxic than other long acting local anesthetics like bupivacaine.[2] Local anesthetics alone for supraclavicular brachial plexus block provide good operative conditions but have shorter duration of postoperative analgesia. Hence, various adjuvants like opioids,[3] clonidine,[4] neostigmine, dexamethasone,[5] midazolam,[6] etc., were added to local anesthetics in brachial plexus block to achieve quick, dense, and prolonged block, but the results are either inconclusive or associated with side effects.
Magnesium is the fourth most plentiful cation in the body and the second most plentiful intracellular cation after potassium. Magnesium is necessary for the presynaptic release of acetylcholine from nerve endings and may produce effects similar to calcium-entry-blocking drugs.[7] Anti-nociceptive effects of magnesium are due to regulation of calcium influx into the cell and antagonism of the N-methyl D-aspartate (NMDA) receptors.[8] Many clinical investigations have demonstrated that Mg administration during general anesthesia has reduced anesthetic requirement and postoperative analgesic consumption.[9,10] Magnesium has popularly been used as antihypertensive agent.[11] Thus, magnesium has long been used for its analgesic, antihypertensive, and anesthetic sparing effects.[12] Magnesium, after administration through epidural route, decreased postoperative opioid consumption.[9] Though magnesium has an analgesic property, it has not been studied well as an adjuvant to the local anesthetic agents during supraclavicular brachial plexus block.
Our current study was designed to test the hypothesis that magnesium when added as an adjuvant to ropivacaine in supraclavicular brachial plexus block may enhance the duration of sensory and motor block, duration of analgesia, and quality of block.
METHODS
After obtaining permission from institutional ethics committee, written informed consent was taken. Totally, 100 adult patients were randomly allocated to two equal groups (n = 50 in each group) using computer-generated random number list. Patients with the American Society of Anesthesiologists’ (ASA) physical status I and II, aged between 25 and 55 years of both sexes undergoing elective orthopedic surgeries of elbow, forearm, and hand under supraclavicular brachial plexus block were enrolled in the study. Patients in group RN received 30 ml of 0.5% ropivacaine + 1 ml normal saline and patients in group RM received 30 ml 0.5% ropivacaine + 150 mg (in 1 ml 0.9% saline) magnesium sulfate for supraclavicular block.
Patient refusal, any known hypersensitivity or contraindication to ropivacaine, magnesium sulfate, pregnancy, lactating mothers, hepatic, renal or cardiopulmonary abnormality, alcoholism, diabetes, long-term analgesic therapy, bleeding diathesis, and local skin site infections were considered as exclusion criteria. Patients having history of significant neurological, psychiatric, or neuromuscular disorders were also excluded.
In preoperative assessment the patients were enquired about any history of drug allergy, previous operations or prolonged drug treatment. General examination, systemic examinations, and airway assessment were done. Preoperative fasting of minimum 6 h was ensured before operation. All patients received premedication of diazepam 10 mg orally, the night before surgery as per preanesthetic check-up direction to allay anxiety and apprehension and for sound sleep.
All patients were clinically examined in the preoperative period, when whole procedure was explained. Visual analog scale (VAS) (0, no pain and 10, worst pain imaginable) was also explained during preoperative visit. All patients are investigated for hemoglobin level, total leukocyte count, differential leukocyte count, erythrocyte sedimentation rate, platelet count, blood sugar, blood urea, serum creatinine, and liver function tests. A 12-lead electrocardiogram (ECG) and chest X-ray were also taken. On entering the patient in the operative room, standard intraoperative monitors like ECG, pulse oximeter, and noninvasive blood pressure were attached and baseline parameters were recorded. Intravenous (IV) infusion of Ringers’ lactate was started and oxygen was given at 3 L/min via face mask. All patients received midazolam 0.04 mg/kg before procedure.
After proper explanation of technique and positioning interscalene groove, a mark was made approximately 1.5–2.0 cm posterior to the mid-clavicle point. The stimulation frequency was set at 1 Hz and the intensity of the stimulating current was initially set to deliver 2 mA and was then gradually decreased. The 22-gauge 5 cm, insulated needle was used. The position of the needle was considered to be acceptable when an output current <0.5 mA still elicited a slight distal motor response in forearm and hand. On negative aspiration for blood, a total volume of 31 ml solution was injected slowly as per allotment of the group and drug. Not only the patients, but also the anesthesiologists performing supraclavicular block was unaware of the constituent of the drug and group allotments. Similarly, resident doctors keeping records of different parameters including VAS score were also unaware of group allotment and drug used in supraclavicular block. Thus, blinding was properly maintained.
Sensory and motor blockade were assessed every 2 min after completion of injection till 30 min and then every 30 min after the end of surgery till first 12 h, thereafter hourly until the block had completely worn off. Sensory blockade of each nerve was assessed by pinprick. Onset time of motor blockade was defined as the time interval between the end of local anesthetic injection and paresis in all of the nerve distributions. VAS was measured every hour after the end of surgery for 24 h.
The duration of sensory block was defined as the time interval between the onset of sensory block and the first postoperative pain. The duration of motor block was defined as the time interval between the onset of motor block and complete recovery of motor functions. After 30 min, if the block was considered to be adequate, surgery commenced. After operation was over, VAS score was measured hourly. Injection of 75 mg diclofenac sodium (rescue analgesic) was given intramuscularly (IM) when VAS ≥ 3 cm. Number of diclofenac injections given to each patient during the first 24 h of postoperative period was recorded (maximum two IM injections were given in 24 h duration).
Sample size was estimated using first rescue analgesic requirement among two groups as the main primary variable. After conducting a pilot study on 15 patients, the average duration of analgesia was found to be 400 min. Furthermore, detecting a difference of 10% (i.e. 40 min), at the P < 0.05 level, with a probability of detecting a difference this large, if it exists, of 80% (1-beta = 0.80), were considered. On the basis of previous study assuming within group standard deviation of 68 min, we needed to study at least 46 patients per group to be able to reject the null hypothesis that the population means of the groups are equal with probability (power) of 0.80. We had taken 52 patients in each group for this prospective study. Raw data were entered into a MicroSoft Excel spreadsheet and analyzed using standard statistical software SPSS, version 18.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were analyzed using the Pearson's Chi-square test. Normally distributed continuous variables were analyzed using the independent sample t-test and P < 0.05 was considered statistically significant.
RESULTS
We recruited 52 subjects per group, more than the calculated sample size. There were no dropouts. However, having excluding subjects who failed blocks, 50 patients in the Magnesium sulfate group (RM) and 50 in the normal saline group (RN) were eligible for effectiveness analysis. The difference in the number of valid blocks in the two groups was not statistically significant.
The age, sex distribution, body weight, ASA status, and duration of surgery in the two groups were found to be comparable [Table 1]. Indications for different upper limb orthopedic surgeries were also similar and have no clinical significance (data not shown). Onset of both sensory and motor block was statistically comparable among two groups [Table 2] and was clinically insignificant (P = 0.46, and P = 0.30, respectively). Whereas Table 2 shows that sensory and motor block durations were statistically greater in the group receiving Magnesium sulfate (RM) (P = 0.001, and P = 0.012, respectively) than group RN.
Table 1.
Comparison of demographic data between the two study groups

Table 2.
Onset time and duration of sensory and motor block; and rescue analgesic requirement in postoperative period (time and number of intramuscular diclofenac sodium injections)
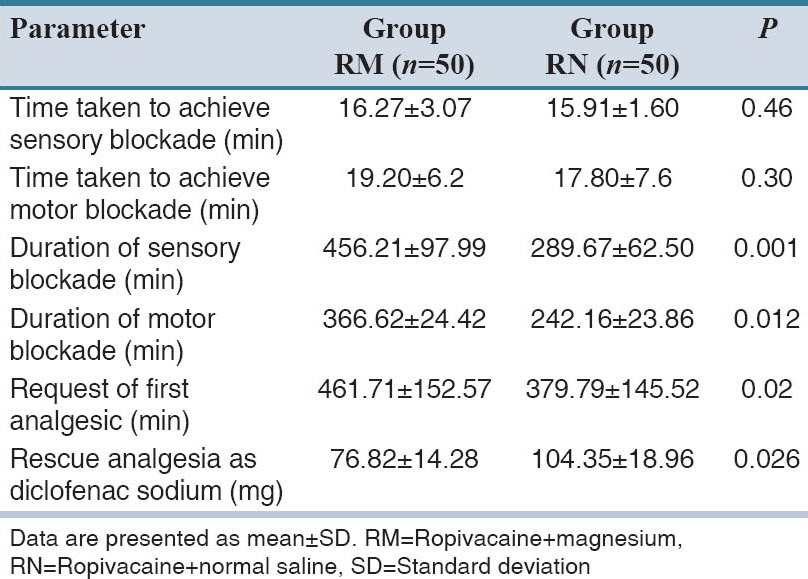
The mean time from block placement to first request for pain medication, that is, the duration of analgesia was 461.71 min in the Magnesium sulfate group but 379.79 min in the normal saline group. This difference (about 81.92 min) was statistically significant (P = 0.02) [Table 2].
Table 2 shows that group RM required less amount of diclofenac sodium injection as rescue analgesics than patients in group RN (saline group) in first 24 h of postoperative period, and the difference is statistically highly significant (P = 0.026).
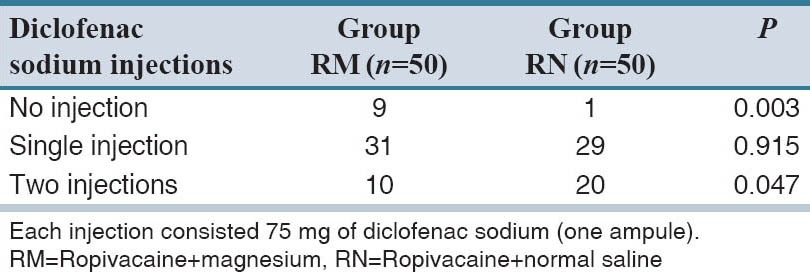
In Table 3, the number of diclofenac sodium injections consumed by each patient has been described and compared among the two groups. Group RM when compared with RN, received less amount of rescue analgesic which was statistically significant.
Table 3.
Postoperative rescue analgesic requirement (number of intramuscular diclofenac sodium injections) in the first 24 hours
Regarding the side effects encountered throughout the study, group RM suffered from slightly more nausea and hypotension, however, it was statistically insignificant (P = 0.39, and P = 0.12, respectively) when compared with group RN. Figure 1 shows that VAS score was of much lower value in group RM than group RN.
Figure 1.
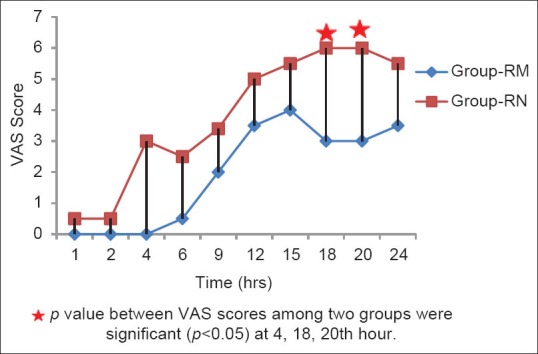
Comparison of visual analog scale score between the study groups (RM: Ropivacaine + magnesium; RN: Ropivacaine + normal saline)
DISCUSSION
Supraclavicular blocks have been administered at the level of nerve trunk of the brachial plexus. The sole sensory, motor, and sympathetic supply of upper limb are conducted by three nerve trunk contained in a very small, compact but easily accessible and relatively superficial area. As a result of this block, a prompt onset of foreseeable and profound anesthesia is achieved with high level of certainty.[13] Local anesthetics alone for supraclavicular brachial plexus block provide good operative conditions but have shorter duration of postoperative analgesia.
Magnesium sulfate has analgesic, antihypertensive, anesthetic sparing effects when used in systemic route.[9,10,11,12] Use of magnesium sulfate as an adjuvant mixed with local anesthetics has been performed with neuraxial anesthesia in both spinal and epidural routes, even with different doses.[13,14,15,16] Mixing magnesium sulfate as adjuvant with local anesthetics during peripheral nerve and nerve plexus blockade has recently been practiced by anesthesiologists.[17,18]
In this prospective, randomized, double-blinded trial, we had compared the effect of 1 ml of Magnesium sulfate (150 mg) in normal saline solution and same volume of placebo as an adjuvant to 30 ml 0.50% ropivacaine in supraclavicular brachial plexus block, on the onset time and duration of sensory and motor block as well as on the postoperative rescue analgesic (diclofenac sodium injection) requirement.
The demographic profile of patients, which was statistically insignificant between two groups, was quite similar with other research investigations,[19] and provided us the uniform platform to evenly compare the results obtained. A study on the role of magnesium for prolongation of postoperative analgesia was conducted by Gunduz et al. in a total of 60 patients yielded similar results.[19] The mean duration of surgery and tourniquet time were almost comparable in both groups with no significant statistical difference [Table 1].
The onset time of sensory block (P = 0.46) and of motor block (P = 0.30) was also comparable among the two groups [Table 2]. Nath et al.[14] found that the use of intrathecal magnesium caused a delay in onset of sensory and motor block, but it was statistically insignificant. Similar results were observed by Khezri et al.[20] and Malleeswaran et al.[21] However, Ekmekci et al.[22], while performing femoral nerve block, found significantly delayed onset of sensory block in the levobupivacaine, magnesium group than in the levobupivacaine group.
In our study, the duration of sensory block (456.21 ± 97.99 min in group RM, vs. 289.67 ± 62.50 min in group RN) was significantly longer in the magnesium group than in the control group (P = 0.001). The duration of motor block (366.62 ± 24.42 min in RM group, vs. 242.16 ± 23.86 min in RN group) was also significantly longer in the magnesium group than in the control group (P = 0.012). These findings lend support to the observations of various earlier studies by Nath et al.,[14] Malleeswaran et al.,[21] Ekmekci et al.[22] and Lee et al.[23]
In our study, mean duration of sensory block (analgesia) and motor block in the magnesium plus ropivacaine (RM) group were 7.60 h (456.21 min) and 6.11 h (366.62 min), respectively. While mean duration of analgesia and motor block after intrathecal bupivacaine, fentanyl plus magnesium group were 4.85 h and 4.01 h, respectively, in the study conducted by Nath et al.[14] Again the median duration of sensory and motor block in the bupivacaine, fentanyl plus magnesium group in intrathecal route were 3.82 h and 3.33 h, respectively, in the study by Malleeswaran et al.[21] Sensory and motor block duration after interscalene nerve block with bupivacaine, epinephrine plus magnesium sulfate were 10.6 h and 11.06 h respectively in the original work by Lee et al.[23]
In our study, patients of RM group required significantly less number of diclofenac sodium injection in first 24 h of postoperative period than the patients in RN group (P = 0.026). This finding correlates with the studies of Lee et al.[23] During interscalene block, they found that 16 patients of bupivacaine plus normal saline group required IV meperidine 0.5 mg/kg as rescue analgesic, whereas 14 patients in magnesium plus bupivacaine group required same drug as rescue analgesic, but the result was not statistically significant.[19] Reduced requirement of rescue analgesic in the magnesium group during the first 24 h of postoperative period is certainly due to prolonged duration of sensory block.
ELShamaa et al. also experienced that statistically much less amount (35.6 mg vs. 113.6 mg) of diclofenac sodium was administered as rescue analgesic in bupivacaine plus magnesium group, while comparing with bupivacaine plus normal saline group during femoral nerve block.[24] They also found that less number of patients (9 vs. 30) in magnesium sulfate group asked for rescue analgesia.
Nausea was observed in four and two patients in group RM and RN, respectively. They needed no active management except increasing the fluid transfusion rate. Two patients of RM group vomited and managed with slow IV metoclopramide 10 mg. No patients in RN group suffered from vomiting. Both results were statistically insignificant (P = 0.24). Choi et al.[18] also found similar side effects (nausea, vomiting, dizziness, headache), whereas the difference between magnesium and normal saline group was also not significant (P = 0.62). Hypotension was observed in five patients in RM group and two patients in RN group, but the difference was not statistically significant. Only one patient in RM group required IV mephentermine for hypotension management.
Magnesium and Ropivacaine dose was chosen as per recommendation in the text book as well as experience of our previous researchers.[17,18,19,22,23,25,26,27] While writing this discussion, we have found the reference of lowest possible volume (10 ml) and concentration (0.375%) of ropivacaine for postoperative analgesia by Iwata et al.[28] However, we had used a higher concentration and much higher volume for intra- as well as postoperative analgesia.
Several hypothesized mechanisms of action have been suggested to explain the analgesic effect of Magnesium. This cation has emerging role in anesthesia due to its analgesic activity chiefly exerted by NMDA receptor antagonism in a noncompetitive manner but at the same time blocking competitively the entry of calcium in presynaptic endings leading to reduced release of acetylcholine.[29] Thus, magnesium administration is strongly associated with reduced post synaptic activity of slow conducting unmyelinated C-fibers which are chiefly afferent fibers conveying input signals from periphery to CNS.[30] Magnesium prevents the activation of NMDA receptors which causes calcium and sodium influx into the cell with an efflux of potassium and initiation of central sensitization and wind-up leading to propagation of peripheral nociceptive stimulation.[29,30,31] This antagonist prevent and abolish hypersensitization once it is established by blocking dorsal horn NMDA receptor activation induced by excitatory amino acid transmitters, such as glutamate and aspartate.[31] Though non selective but magnesium and ketamine; NMDA receptor antagonists; are still now good option for opioid independent analgesic regimen.[32] Magnesium is the second most abundant intracellular cation and physiological calcium channel antagonist. In animal models of pain, calcium channel antagonists have been demonstrated to provide analgesia,[33] and in chronic pain situations, they synergistically potentiate opioid-induced antinociception.[34]
Finally, unsuccessful block was encountered in two patients (4%) in each group in our study which is quite comparable to previous studies using nerve stimulator guided approaches to supraclavicular brachial plexus blockade.[35]
We do conclude that addition of 150 mg magnesium sulfate to ropivacaine 0.50% solution in supraclavicular brachial plexus block prolongs the duration of sensory and motor blockade and reduces the requirement of rescue analgesic in postoperative period but slightly delays the onset time of sensory and motor blockade.
AUTHORS’ CONTRIBUTION
KM: Planning and Study Design, AD: Manuscript writing and Editing, SRB: Data collection and analysis, PM: Statistical analysis and consult with experts, AM: Study design analysis and Data Collection.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bruce BG, Green A, Blaine TA, Wesner LV. Brachial plexus blocks for upper extremity orthopaedic surgery. J Am Acad Orthop Surg. 2012;20:38–47. doi: 10.5435/JAAOS-20-01-038. [DOI] [PubMed] [Google Scholar]
- 2.Vainionpää VA, Haavisto ET, Huha TM, Korpi KJ, Nuutinen LS, Hollmén AI, et al. A clinical and pharmacokinetic comparison of ropivacaine and bupivacaine in axillary plexus block. Anesth Analg. 1995;81:534–8. doi: 10.1097/00000539-199509000-00019. [DOI] [PubMed] [Google Scholar]
- 3.Bazin JE, Massoni C, Groslier D, Fenies V, Bittar M, Schoeffler P. Brachial plexus block: Effect of the addition of sufentanil to local anesthetic mixture on postoperative analgesia duration. Ann Fr Anesth Reanim. 1997;16:9–13. doi: 10.1016/s0750-7658(97)84271-2. [DOI] [PubMed] [Google Scholar]
- 4.Kohli S, Kaur M, Sahoo S, Vajifdar H, Kohli P. Brachial plexus block: Comparison of two different doses of clonidine added to bupivacaine. J Anaesthesiol Clin Pharmacol. 2013;29:491–5. doi: 10.4103/0970-9185.119147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yadav RK, Sah BP, Kumar P, Singh SN. Effectiveness of addition of neostigmine or dexamethasone to local anaesthetic in providing perioperative analgesia for brachial plexus block: A prospective, randomized, double blinded, controlled study. Kathmandu Univ Med J (KUMJ) 2008;6:302–9. doi: 10.3126/kumj.v6i3.1704. [DOI] [PubMed] [Google Scholar]
- 6.Jarbo K, Batra YK, Panda NB. Brachial plexus block with midazolam and bupivacaine improves analgesia. Can J Anaesth. 2005;52:822–6. doi: 10.1007/BF03021776. [DOI] [PubMed] [Google Scholar]
- 7.Sirvinskas E, Laurinaitis R. Use of magnesium sulfate in anesthesiology. Medicina (Kaunas) 2002;38:695–8. [PubMed] [Google Scholar]
- 8.Agrawal A, Agrawal S, Payal YS. Effect of continuous magnesium sulfate infusion on spinal block characteristics: A prospective study. Saudi J Anaesth. 2014;8:78–82. doi: 10.4103/1658-354X.125945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Telci L, Esen F, Akcora D, Erden T, Canbolat AT, Akpir K. Evaluation of effects of magnesium sulphate in reducing intraoperative anaesthetic requirements. Br J Anaesth. 2002;89:594–8. doi: 10.1093/bja/aef238. [DOI] [PubMed] [Google Scholar]
- 10.Koinig H, Wallner T, Marhofer P, Andel H, Hörauf K, Mayer N. Magnesium sulfate reduces intra- and postoperative analgesic requirements. Anesth Analg. 1998;87:206–10. doi: 10.1097/00000539-199807000-00042. [DOI] [PubMed] [Google Scholar]
- 11.Panda NB, Bharti N, Prasad S. Minimal effective dose of magnesium sulfate for attenuation of intubation response in hypertensive patients. J Clin Anesth. 2013;25:92–7. doi: 10.1016/j.jclinane.2012.06.016. [DOI] [PubMed] [Google Scholar]
- 12.Do SH. Magnesium: A versatile drug for anesthesiologists. Korean J Anesthesiol. 2013;65:4–8. doi: 10.4097/kjae.2013.65.1.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pascual-Ramírez J, Gil-Trujillo S, Alcantarilla C. Intrathecal magnesium as analgesic adjuvant for spinal anesthesia: A meta-analysis of randomized trials. Minerva Anestesiol. 2013;79:667–78. [PubMed] [Google Scholar]
- 14.Nath MP, Garg R, Talukdar T, Choudhary D, Chakrabarty A. To evaluate the efficacy of intrathecal magnesium sulphate for hysterectomy under subarachnoid block with bupivacaine and fentanyl: A prospective randomized double blind clinical trial. Saudi J Anaesth. 2012;6:254–8. doi: 10.4103/1658-354X.101217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Banwait S, Sharma S, Pawar M, Garg R, Sood R. Evaluation of single epidural bolus dose of magnesium as an adjuvant to epidural fentanyl for postoperative analgesia: A prospective, randomized, double-blind study. Saudi J Anaesth. 2012;6:273–8. doi: 10.4103/1658-354X.101221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jabalameli M, Pakzadmoghadam SH. Adding different doses of intrathecal magnesium sulfate for spinal anesthesia in the cesarean section: A prospective double blind randomized trial. Adv Biomed Res. 2012;1:7. doi: 10.4103/2277-9175.94430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dogru K, Yildirim D, Ulgey A, Aksu R, Bicer C, Boyaci A. Adding magnesium to levobupivacaine for axillary brachial plexus block in arteriovenous fistule surgery. Bratisl Lek Listy. 2012;113:607–9. doi: 10.4149/bll_2012_136. [DOI] [PubMed] [Google Scholar]
- 18.Choi IG, Choi YS, Kim YH, Min JH, Chae YK, Lee YK, et al. The Effects of Postoperative Brachial Plexus Block Using MgSO (4) on the Postoperative Pain after Upper Extremity Surgery. Korean J Pain. 2011;24:158–63. doi: 10.3344/kjp.2011.24.3.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gunduz A, Bilir A, Gulec S. Magnesium added to prilocaine prolongs the duration of axillary plexus block. Reg Anesth Pain Med. 2006;31:233–6. doi: 10.1016/j.rapm.2006.03.001. [DOI] [PubMed] [Google Scholar]
- 20.Khezri MB, Yaghobi S, Hajikhani M, Asefzadeh S. Comparison of postoperative analgesic effect of intrathecal magnesium and fentanyl added to bupivacaine in patients undergoing lower limb orthopedic surgery. Acta Anaesthesiol Taiwan. 2012;50:19–24. doi: 10.1016/j.aat.2012.03.001. [DOI] [PubMed] [Google Scholar]
- 21.Malleeswaran S, Panda N, Mathew P, Bagga R. A randomised study of magnesium sulphate as an adjuvant to intrathecal bupivacaine in patients with mild preeclampsia undergoing caesarean section. Int J Obstet Anesth. 2010;19:161–6. doi: 10.1016/j.ijoa.2009.08.007. [DOI] [PubMed] [Google Scholar]
- 22.Ekmekci P, Bengisun ZK, Akan B, Kazbek BK, Ozkan KS, Suer AH. The effect of magnesium added to levobupivacaine for femoral nerve block on postoperative analgesia in patients undergoing ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013;21:1119–24. doi: 10.1007/s00167-012-2093-4. [DOI] [PubMed] [Google Scholar]
- 23.Lee AR, Yi HW, Chung IS, Ko JS, Ahn HJ, Gwak MS, et al. Magnesium added to bupivacaine prolongs the duration of analgesia after interscalene nerve block. Can J Anaesth. 2012;59:21–7. doi: 10.1007/s12630-011-9604-5. [DOI] [PubMed] [Google Scholar]
- 24.ELShamaa HA, Ibrahim M, Eldesuky HI. Magnesium sulfate in femoral nerve block, does postoperative analgesia differ? A comparative study. Egypt J Anaesth. 2014;30:169–73. [Google Scholar]
- 25.Berde CB, Strichartz GR. Local anesthetics. In: Miller RD, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Young WL, editors. Miller's Anesthesia. 7th ed. Philadelphia: Churchill Livingstone Elsevier; 2010. pp. 913–36. [Google Scholar]
- 26.Duggan E, El Beheiry H, Perlas A, Lupu M, Nuica A, Chan VW, et al. Minimum effective volume of local anesthetic for ultrasound-guided supraclavicular brachial plexus block. Reg Anesth Pain Med. 2009;34:215–8. doi: 10.1097/AAP.0b013e31819a9542. [DOI] [PubMed] [Google Scholar]
- 27.Yang CW, Kwon HU, Cho CK, Jung SM, Kang PS, Park ES, et al. A comparison of infraclavicular and supraclavicular approaches to the brachial plexus using neurostimulation. Korean J Anesthesiol. 2010;58:260–6. doi: 10.4097/kjae.2010.58.3.260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Iwata T, Nakahashi K, Inoue S, Furuya H. Low-dose ropivacaine for supraclavicular brachial plexus block combined with general anesthesia for successful postoperative analgesia: A case series. Saudi J Anaesth. 2013;7:37–9. doi: 10.4103/1658-354X.109806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Woolf CJ, Thompson SW. The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain. 1991;44:293–9. doi: 10.1016/0304-3959(91)90100-C. [DOI] [PubMed] [Google Scholar]
- 30.Ascher P, Nowak L. Electrophysiological studies of NMDA receptors. Trends Neurosci. 1987;10:284–8. [Google Scholar]
- 31.Woolf CJ, Chong MS. Preemptive analgesia – treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg. 1993;77:362–79. doi: 10.1213/00000539-199377020-00026. [DOI] [PubMed] [Google Scholar]
- 32.Liu HT, Hollmann MW, Liu WH, Hoenemann CW, Durieux ME. Modulation of NMDA receptor function by ketamine and magnesium: Part I. Anesth Analg. 2001;92:1173–81. doi: 10.1097/00000539-200105000-00019. [DOI] [PubMed] [Google Scholar]
- 33.Miranda HF, Bustamante D, Kramer V, Pelissier T, Saavedra H, Paeile C, et al. Antinociceptive effects of Ca2+channel blockers. Eur J Pharmacol. 1992;217:137–41. doi: 10.1016/0014-2999(92)90833-p. [DOI] [PubMed] [Google Scholar]
- 34.Santillán R, Maestre JM, Hurlé MA, Flórez J. Enhancement of opiate analgesia by nimodipine in cancer patients chronically treated with morphine: A preliminary report. Pain. 1994;58:129–32. doi: 10.1016/0304-3959(94)90192-9. [DOI] [PubMed] [Google Scholar]
- 35.Franco CD, Vieira ZE. 1,001 subclavian perivascular brachial plexus blocks: Success with a nerve stimulator. Reg Anesth Pain Med. 2000;25:41–6. doi: 10.1016/s1098-7339(00)80009-7. [DOI] [PubMed] [Google Scholar]