

Abstract
Squamous cell carcinoma of the ovary is a rare condition and usually arises in mature cystic teratoma (MCT) or dermoid cyst of the ovary. The reported incidence of malignant transformation in MCT is approximately 2%. A case of squamous cell carcinoma arising in a dermoid cyst of the ovary presenting at an early stage is presented here. A 53-year-old postmenopausal lady, presented with the complaint of pain in right lower abdomen since one month and a large complex abdomino-pelvic mass on examination and investigations. Final histopathology was reported as squamous cell carcinoma of left ovary arising from dermoid cyst and a benign dermoid cyst in the right ovary. The patient was assigned to squamous cell carcinoma of the ovary arising in a mature cystic teratoma, surgical stage Ic2. In view of the poor prognosis, adjuvant chemotherapy was started.
Keywords: Chemotherapy, dermoid cyst, mature cystic teratoma, squamous cell carcinoma of the cervix, tumor markers
INTRODUCTION
Mature cystic teratomas (MCT; also called dermoid cysts) account for about 30-45% of all ovarian neoplasms and around 60% of all benign tumors arising in the ovary[1] with a 0.17-1.4% reported incidence of malignant transformation.[2,3] Squamous cell carcinoma in MCTs is most commonly seen in postmenopausal women.[4] There are no definitive clinical features, tumor markers are not often raised and imaging methods are many times not helpful. Hence, most cases are diagnosed postoperatively.[5] Tumors confined to the ovary usually have a better prognosis and patients with stage III or IV disease rarely survive five years.[6]
Here, we are presenting a case of squamous cell carcinoma of the ovary which was diagnosed at an early stage and was managed appropriately keeping in mind the poor prognosis of the condition.
CASE REPORT
A 53-year-old postmenopausal lady, gravida3para2 with 1 abortion, presented in the outpatient wing of gynecologic oncology department of Bhagwan Mahaveer Cancer Hospital & Research Centre, Jaipur, Rajasthan with the complaint of pain in right lower abdomen since one month. Her general condition was good. There was no visible or palpable evidence of any neck swelling, breast abnormality or lymphadenopathy. Her per abdominal examination showed a large firm to hard, non-tender, well-defined, mobile mass in right iliac and hypogastric region arising out of pelvis. Her pelvic exam revealed a mobile mass on right side moving with cervical movement. Routine and specific investigations were carried out. USG whole abdomen suggested the possibility of a dermoid cyst of the ovary (side not specified). MRI of the abdomen reported a large complex multicystic abdomino-pelvic mass with fat fluid levels. A Large solid component along right side of lesion was seen extending in right iliac fossa. Tumor markers were carried out and values were reported as follows:
CA 125: 143 U/ml.
CEA: 13.1ng/ml.
CA 19.9: 2350 U/ml.
Laparotomy was done on her. A large abdomino-pelvic, irregular, twisted and ruptured left ovarian mass was encountered on opening the abdomen. The mass was densely adherent to omentum, intestine, pelvic peritoneum and appendix. Adhesions were dissected and the mass along with appendix and part of the adherent omentum were sent for frozen section. Frozen section reported possibility of squamous cell carcinoma arising in a dermoid cyst and no malignancy in appendix. Complete surgical staging and primary cytoreduction was done.
Final histopathology was reported as squamous cell carcinoma of left ovary arising from dermoid cyst and a benign dermoid cyst in the right ovary [Figure 1]. Both fallopian tubes, parametrial tissues, peritoneal biopsies, uterus, cervix, omentum and pelvic lymph nodes were unremarkable. Peritoneal fluid was negative for malignant cells.
Figure 1.
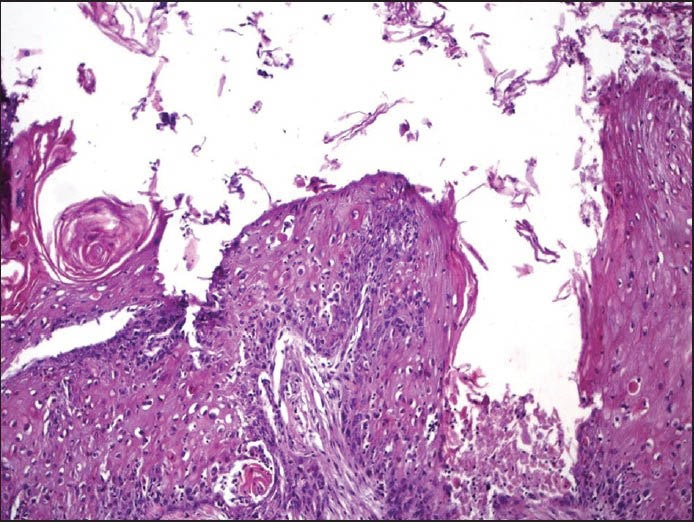
A dermoid cyst showing area of squamous cell carcinoma
For management, the patient was assigned to squamous cell carcinoma of the ovary arising in anMCT, surgical stage Ic2. Her postoperative period was uneventful. In view of poor prognosis, adjuvant chemotherapy (six cycles of Paclitaxel and Carboplatin) was started.
DISCUSSION
Squamous cell carcinoma of the ovary is quite rare and usually arises in MCT of the ovary (up to 2%).[7] Preoperative diagnosis is difficult. MRI may be helpful. CEA may be elevated. Other rare pathologies in MCT are adenocarcinoma and melanoma. Takagi et al have found CEA to be more useful than CA 125 and CA 19-9 in malignant transformation of MCT.[8] This entity carries very poor prognosis especially when diagnosed in advanced stage. Optimal cytoreduction is difficult to achieve in advanced disease.
Suspicious features (clinical and on MRI) include:[6,9]
Postmenopausal women (mean age-55years vs. 37.5 years for benign dermoid cysts).
Larger size of tumor (mean- 152mm vs. 88 mm for benign).
Solid areas within the cyst.
Invasion of adjacent organs/capsule.
A systematic review and analysis of published data was done by Hackethal et al.[4] Sixty-four suitable studies provided information on 277 patients. It was observed that squamous cell carcinoma in MCT was mainly found in women above 50 years of age, having a high concentration of CA 125 and ovarian tumors more than 10 cm in size. They also found that FIGO stage Ia had better survival than those with advanced disease. Complete resection with advanced disease followed by adjuvant chemotherapy was seen to be associated with higher survival. According to them adjuvant radiotherapy did not improve survival.
A case series and review of literature was published in European Oncology and Hematology, 2013.[10] In this retrospective review conducted over 24 years between 1986 and 2010, they found six women treated for squamous cell carcinoma in MCT, all stage III/ IV. They found that durable responses were difficult to achieve but best treatment response was seen in a woman who had partial response to chemo-radiotherapy (survival 19 months). According to them, concurrent chemo-radiation could be considered for disease confined to pelvis. However, median survival in their series was only 12.5 months.
Sporadic case reports have been published by Indian authors on this subject.[11,12] These reports are similar to our case. However, Khajuria et al[13] and Santwani et al[14] have reported squamous cell carcinoma in dermoid cyst at younger ages i.e., 37 years and 40 years, respectively.
CONCLUSION
Keeping in view the rarity and poor prognosis of squamous cell carcinoma of the ovary arising in a mature cystic teratoma, it is very essential for a gynecologic oncologist to be aware of this condition and be equipped to deal with it.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kong CS, Longacre TA, Hendrickson MR. Vol. 38. Philadelphia: Lippincott, Williams & Wilkins; 2012. Gynaecologic Oncology; pp. 176–78. [Google Scholar]
- 2.Comerci JT, Jr, Licciardo F, Bergh PA, Gregori C, Breen JL. Mature cystic teratoma: A clinicopathologic evaluation of 517 cases and review of the literature. Obstet Gynecol. 1994;84:22–8. [PubMed] [Google Scholar]
- 3.Ayhan A, Bukulmez O, Genc C, Karamursel BS, Ayhan A. Mature cystic teratomas of the ovary: Case series from one institution over 34 years. Eur J Obstet Gynecol Reprod Biol. 2000;88:153–7. doi: 10.1016/s0301-2115(99)00141-4. [DOI] [PubMed] [Google Scholar]
- 4.Hackethal A, Brueggmann D, Bohlmann MK, Franke FE, Tinneberg HR, Münstedt K. Squamous cell carcinoma in mature cystic teratoma of the ovary: Systematic review and analysis of published data. Lancet Oncol. 2008;9:1173–80. doi: 10.1016/S1470-2045(08)70306-1. [DOI] [PubMed] [Google Scholar]
- 5.Hurwitz JL, Fenton A, McCluggage WG, McKenna S. Squamous cell carcinoma arising in a dermoid cyst of the ovary: A case series. BJOG. 2007;114:1283–7. doi: 10.1111/j.1471-0528.2007.01478.x. [DOI] [PubMed] [Google Scholar]
- 6.Kikkawa F, Nawa A, Tamakoshi K, Ishikawa H, Kuzuya K, Suganuma N, et al. Diagnosis of squamous cell carcinoma arising from mature cystic teratoma of ovary. Cancer. 1998;82:2249–55. doi: 10.1002/(sici)1097-0142(19980601)82:11<2249::aid-cncr21>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- 7.Pins MR, Young RH, Daly WJ, Scully RE. Primary squamous cell carcinoma of the Ovary. Report of 37 cases. Am J Surg Pathol. 1996;20:823–33. doi: 10.1097/00000478-199607000-00005. [DOI] [PubMed] [Google Scholar]
- 8.Takagi H, Ichigo S, Murase T, Ikeda T, Imai A. Early diagnosis of malignant — Transformed ovarian mature cystic teratoma: Fat-suppressed MRI findings. J Gynecol Oncol. 2012;23:125–8. doi: 10.3802/jgo.2012.23.2.125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kido A, Togashi K, Konishi I, Kataoka ML, Koyama T, Ueda H, et al. Dermoid cysts of the ovary with malignant transformation: MR appearance. AJR Am J Roentgenol. 1999;172:445–9. doi: 10.2214/ajr.172.2.9930800. [DOI] [PubMed] [Google Scholar]
- 10.Powell JR, Haldar K. Squamous cell carcinoma arising in a mature cystic teratoma of ovary: A case series and review of literature. Eur Oncol Hematol. 2013;9:17–20. [Google Scholar]
- 11.Mardi K, Sharma S. Squamous cell carcinoma arising in an ovarian mature cystic teratoma. Clin Cancer Investig J. 2014;3:96–8. [Google Scholar]
- 12.Madan M, Bhagat R, Agarwal AP, Sharma S. Squamous cell carcinoma arising in mature cystic teratoma: A rare case. Indian J Cancer. 2010;47:346–7. doi: 10.4103/0019-509X.64708. [DOI] [PubMed] [Google Scholar]
- 13.Khajuria R, Bagotra M, Bhat R, Dubey VK. Squamous cell carcinoma arising in a cystic teratoma. J K Sci. 2000;2:110–2. [Google Scholar]
- 14.Santwani PM, Trivedi DP, Vachhani JH, Trivedi NJ. Coexistence of squamous cell carcinoma with dermoid cyst of ovary. Indian J Pathol Microbiol. 2008;51:81–2. doi: 10.4103/0377-4929.40409. [DOI] [PubMed] [Google Scholar]