

Abstract
The use of the Sonopet Omni, an ultrasonic bone curette, has been discussed for ear, nose, and throat, neurosurgical, and maxillofacial procedures. Its use in oculoplastic and orbital surgery has not been extensively described. The Sonopet has a number of advantages that impart particular utility when operating in the orbit. We present three illustrative cases highlighting the unique advantages of the Sonopet: 1) the ability to spare critical soft tissues; 2) the facility to sculpt and restore the complex contour of the orbit; 3) the capability to biopsy infiltrative lesions that may not be as amenable to manipulation with conventional drills; and 4) a small footprint ideal for small operative fields such as the orbit.
The use of the Sonopet Omni Ultrasonic Surgical System (Stryker, Kalamazoo, MI) in oculoplastic surgery has received little attention. The Sonopet's use in orbital decompression (1), and more recently in dacryocystorhinostomy (2), has been documented; its application in orbital tumor excision has not been described. The Sonopet has a number of advantages: 1) it is less traumatic to soft tissues than conventional drills; 2) it allows for sculpting of bone into smooth or contoured shapes; 3) less force is required, allowing more controlled removal of bone, particularly bone that is infiltrated or abnormal; and 4) its relatively small footprint allows access to small operative fields. In this case series, we describe its use, advantages, and disadvantages with a focus on three orbital tumor cases.
The Sonopet unit used here comprised a power supply, foot switch, handpiece, and surgical tip. The footswitch has two pedals: the first engaging vibration with simultaneous irrigation and aspiration, and the second initiating irrigation alone. Several handpieces are currently available. The handpiece used for these cases weighs 110 g, is 140 mm long, and is 20 mm in diameter (Figures 1a, 1b). The longitudinal vibration amplitude varies from 120 to 365 um, at a frequency of 25 kHz. The 20°C irrigation fluid emerges through a sheath near the tip of the handpiece and has an adjustable rate between 3 and 40 mL/min. Aspiration occurs at the tip of the handpiece with a maximum aspiration pressure of 500 mm Hg. Eight surgical tips are currently available. The tip used here is in a Spetzler Claw shape designed for bone fragmentation and removal (Figure 1c).
Figure 1.
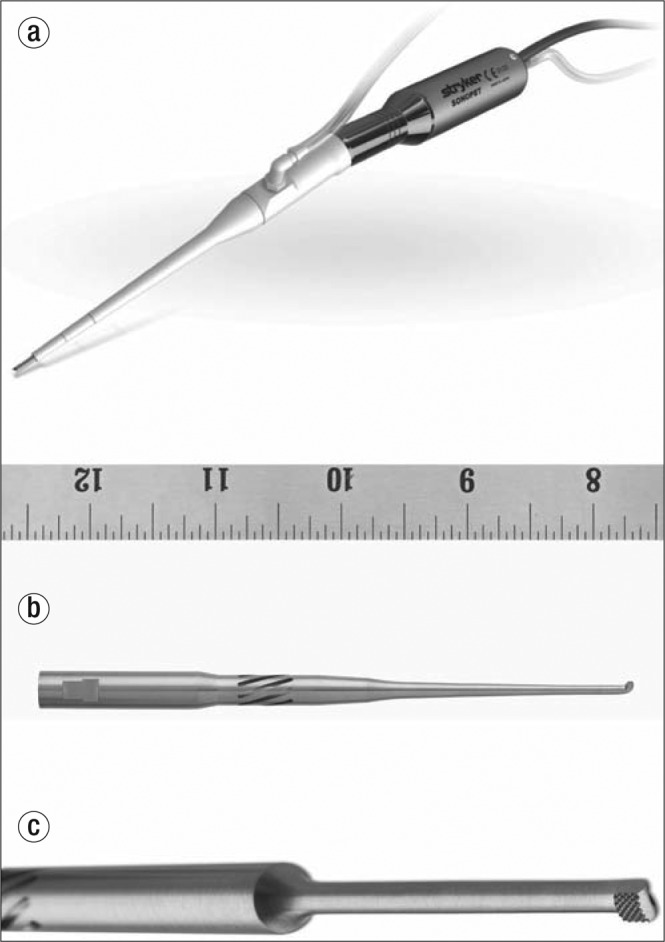
(a) The Sonopet unit, (b) its handpiece with scale in inches, and (c) its handpiece with the Spetzler claw head.
CASE 1
A 51-year-old woman with a history of multiple intracranial meningiomas presented to our practice with left-sided proptosis, exposure keratopathy with pain, and limited extraocular motility. Magnetic resonance imaging revealed a left orbital apex meningioma with proptosis. The patient was taken to the operating room where a bicoronal flap and anterior craniotomy was created to expose the orbital roof. An en bloc excision of the orbital roof was accomplished, followed by subperiosteal dissection of the superior orbit. The periorbita was opened and the mass was identified in the orbital apex.
The oculomotor nerve was noted to be coursing over the mass and was firmly adherent to it. Using the Sonopet, the oculomotor nerve was dissected free from the mass and left intact throughout the procedure. This was accomplished by the unique ability of the Sonopet to spare the relatively soft oculomotor nerve while emulsifying the surrounding firm tumor. The oculomotor nerve was carefully retracted and dissected as the mass was gradually emulsified by the torsional emulsification of the Sonopet.
CASE 2
A 50-year-old woman with no significant past medical or surgical history presented with right-sided orbital pain, proptosis, diplopia, and blurred vision. A computed tomography (CT) scan demonstrated a right orbital mass consistent with fibrous dysplasia impinging on the lateral rectus muscle and the orbital contents (Figure 2a). The patient was taken to the operating suite, where a lateral canthotomy and cantholysis was used to expose the lateral orbital wall. A sagittal saw was used to remove a portion of the lateral orbital wall, and subperiosteal dissection was performed to identify the lesion. Intraoperative navigation was used to identify the extent of the mass, and the Sonopet was used to remove the mass as it extended into the orbital apex, care being taken to identify and preserve the orbital contents. Additional aspects of the mass were exposed and excised along the greater wing of the sphenoid.
Figure 2.

Case 2. (a) Axial CT scan demonstrating orbital fibrous dysplasia involving the greater wing of the sphenoid on the right. (b) Postoperative axial CT scan demonstrating improved proptosis and orbital decompression following excisional surgery with the Sonopet.
The lesion was reduced using the Sonopet to restore the normal contour of the lateral orbital wall (Figure 2b). This was accomplished by gradually sculpting the lateral orbital wall by emulsifying minute layers of bone in a painting fashion, as one might imagine buffing a floor. Small circular movements were used to emulsify the lateral orbital wall to restore the concave shape, allowing for appropriate decompression of the orbital contents.
CASE 3
A 51-year-old woman presented with progressive left-sided enophthalmos and retrobulbar pain. CT scan revealed a left orbit mass with a lobulated consistency as well as left globe retraction (Figure 3). The decision was made to proceed with biopsy given concerning features such as globe retraction and the appearance on CT scan. The patient was taken to the operating room where a Krönlein orbitotomy was performed with dissection into the lateral orbit. The lateral rim was removed with a sagittal saw. Intraoperative CT-guided navigation was used to localize the mass, which appeared to infiltrate the bone in the lateral and superior orbit, producing a mottled effect.
Figure 3.

Case 3: Axial CT scan demonstrating left retrobulbar mass with globe retraction.
The Sonopet was used to biopsy the mass by retracting the mass from the lateral orbital wall and gradually passing the Sonopet between the mass and the infiltrated bone. The Sonopet's unique ability to emulsify bone but not the softer mass was critical in separating the mass from the bone to enable a biopsy. Moreover, the Sonopet's small footprint and relative tissue specificity enabled a biopsy that did not necessitate removal of a large portion of the lateral orbital wall, thus maintaining the volume and shape of the orbit.
DISCUSSION
The Sonopet's primary mechanism of action is torsional oscillation of a metal bone rasp at 25 kHz. This frequency is ideal, as the microenvironment created cuts only mineralized tissue, while soft tissues are cut at frequencies ≥34 kHz (3). This mechanism, as compared to traditional drills, results in less soft tissue damage and less torque-induced bone fragment displacement in our experience. These features are particularly important when one considers the proximity of critical and fragile tissues in small anatomic spaces such as the orbital apex and lacrimal system. The ability to easily sculpt bone into a contoured shape is particularly advantageous in orbital surgery. Additionally, simultaneous irrigation and aspiration is applied to the surgical field, allowing one-handed use and obviating the need for separate irrigation and aspiration. Moreover, bone removal can be accomplished with minimal manual pressure.
The three orbital tumor cases described, summarized in Table 1, highlight these advantages of the Sonopet. In the first case, it was critical to remove the meningioma without damaging the adherent oculomotor nerve. The unique ability of the Sonopet to preserve soft tissues was critical here. In the second, not only was the Sonopet used in the orbital apex where vital soft tissue structures are in close proximity, but the lateral orbit and greater wing of the sphenoid were reshaped to both decompress the orbit and to restore the normal contour of the lateral orbit. Sculpting the concave lateral orbit by removing minute layers of bone would be quite difficult with a tool such as a sagittal saw. In the third case, the Sonopet was used to carefully dissect and biopsy a mass that was infiltrating the bony lateral orbit while minimizing any change in shape or volume of the orbit. Again, the ability of the Sonopet to emulsify bone while preserving softer tissues allowed the dissection of the mass from the bone it was infiltrating. Moreover, the Sonopet allowed for this dissection while preserving the majority of the lateral wall, thus maintaining the contour and volume of the orbit.
Table 1.
Three orbital tumor cases where the Sonopet was used
| Variable | Case 1: Orbital apex meningioma | Case 2: Greater sphenoid wing fibrous dysplasia | Case 3: Infiltrative mass |
|---|---|---|---|
| Critical tissue spared by Sonopet | Oculomotor nerve | Lateral rectus | None |
| Additional operative time | None | None | None |
| Preoperative exophthalmos | Present | Present | Enophthalmos present |
| Postoperative exophthalmos | None | None | None |
| Preoperative keratopathy | Present | Present | None |
| Postoperative keratopathy | None | None | None |
The Sonopet is less suited for large bony resections when compared with traditional instruments, as it removes a comparatively small amount of bone per amount of time. For example, in the second and third cases, a saw, rather than the Sonopet, was used to remove the lateral orbital rim. Additionally, the cost of the unit is significant, which may limit its availability to large centers or institutions where the unit can be shared among surgical subspecialists.
References
- 1.Cho RI, Choe CH, Elner VM. Ultrasonic bone removal versus high-speed burring for lateral orbital decompression: comparison of surgical outcomes for the treatment of thyroid eye disease. Ophthal Plast Reconstr Surg. 2010;26(2):83–87. doi: 10.1097/IOP.0b013e3181b8e614. [DOI] [PubMed] [Google Scholar]
- 2.Murchison AP, Pribitkin EA, Rosen MR, Bilyk JR. The ultrasonic bone aspirator in transnasal endoscopic dacryocystorhinostomy. Ophthal Plast Reconstr Surg. 2013;29(1):25–29. doi: 10.1097/IOP.0b013e318272d2d1. [DOI] [PubMed] [Google Scholar]
- 3.Samy RN, Krishnamoorthy K, Pensak ML. Use of a novel ultrasonic surgical system for decompression of the facial nerve. Laryngoscope. 2007;117(5):872–875. doi: 10.1097/MLG.0b013e318033f984. [DOI] [PubMed] [Google Scholar]