

Abstract
Renal artery pseudoaneurysm (RAP) is a rare complication of partial nephrectomy, but is usually effectively managed with renal vessel embolisation. We report a particularly challenging case of a patient with chronic kidney disease (CKD) who developed a RAP following a laparoscopic heminephrectomy and was treated using superselective renal vessel coil embolisation with carbon dioxide (CO2) as the primary contrast agent for arteriographic localisation of the RAP and feeder artery. To the best our knowledge we report the first utilisation of CO2 arteriography in the definitive diagnosis and treatment of RAP following heminephrectomy in a patient with severe CKD.
Background
Renal artery pseudoaneurysm (RAP) is a relatively rare and potentially fatal complication of partial nephrectomy.1 2 The localisation and treatment of RAP traditionally involves selective arteriography using iodinated contrast.3 Acute renal injury has been reported in 62% of patients following arteriography in patients with pre-existing renal injury, or serum creatinine greater than 2 mg/dL, making management of RAP in this population a challenge.4 In patients with chronic kidney disease (CKD), carbon dioxide (CO2) has been reported as a non-nephrotoxic alternative to iodinated contrast for arteriography.5 This application has never been reported in the treatment of RAP.
Case presentation
An 82-year-old woman with controlled hypertension, congestive heart failure, diabetes mellitus and CKD (baseline glomerular filtration rate 39 mL/min/1.73 m2and creatinine 1.31 mg/dL) underwent robotic-assisted laparoscopic left heminephrectomy for a 5.8 cm lower pole Bosniak IV renal cyst that was diagnosed with ultrasound (US) during a work up for back pain. Intraoperatively, the renal hilum was controlled using bulldog clamps prior to excision of the renal mass. Collecting system closure was performed with running 2-0 Vicryl and Lapra-Ty clips and parenchymal closure with 2-0 Vicryl, Lapra-Ty and Weck, with intervening FloSeal and Fibrillar placement into the parenchymal defect prior to closure. Her postoperative course was uncomplicated, with stable haemoglobin and she was discharged on postoperative day (POD) 2 with a postoperative creatinine of 2.36 mg/dL and haemoglobin of 8.8 mg/dL. Histology revealed a clear cell renal carcinoma, Fuhrman’s nuclear grade 2 with focal areas of grade 3.
The patient returned to the emergency department on POD 11 following a fall, reported abdominal pain and gross haematuria. On presentation, her haemoglobin was 8 mg/dL, with a creatinine of 1.93 mg/dL, and she was haemodynamically stable. CT without contrast demonstrated a 3.4×5.0 cm fluid collection along the inferior aspect of the left kidney consistent with a perinephric haematoma (figure 1A). Her urine remained clear and haemoglobin stable during admission and she was discharged without need for transfusion. On POD 30 she returned due to recurrent haematuria with a haemoglobin of 6.3 mg/dL and a creatinine of 1.85 mg/dL, non-contrast angiogram (MRA) of the abdomen was unremarkable, but a subsequent duplex US revealed a 1.3×1.7 cm aneurysmal dilation in the left renal artery (figure 1B, C). Given her significant blood loss, acute kidney injury and associated abdominal pain, embolisation of the RAP was recommended.
Figure 1.
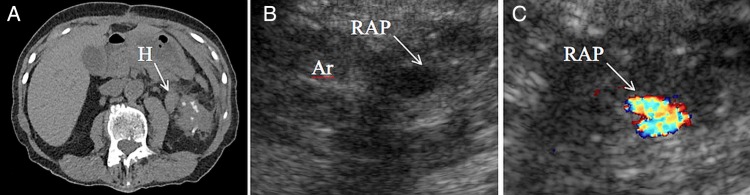
(A) Axial image of a non-contrast CT showing a perinephric collection, with soft tissue attenuation, consistent with a perinephric haematoma (H). (B) Ultrasound (US) depicting a hypoechoic cystic structure, a renal artery pseudoaneurysm (RAP), adjacent to a supplying artery (Ar). (C) Colour Doppler US demonstrating disorganised flow in the RAP.
Treatment
Owing to the patient’s significant baseline CKD and acute kidney injury, CO2 arteriography supplemented with of 5 cc of iodinated iso-osmolar contrast was performed, defining the RAP and a point of arteriovenous fistula flow (figure 2A–C). Superselective coil embolisation of a branching left renal vessel was performed with resolution of the RAP and arteriovenous fistula (figure 3A–C).
Figure 2.
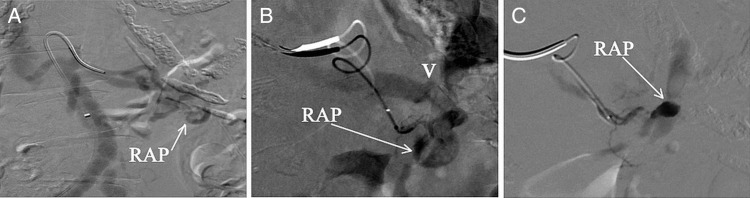
(A) Renal CO2 arteriogram demonstrating left renal arterial branch pseudoaneurysm. (B) Closeup of renal CO2 arteriogram demonstrating renal artery pseudoaneurysm (RAP) and early venous drainage due to arteriovenous fistula (V), after microguidewire and catheter are advanced distally into the feeder vessel. (C) Small amount of iodinated iso-osmolar contrast material is injected directly into the RAP.
Figure 3.
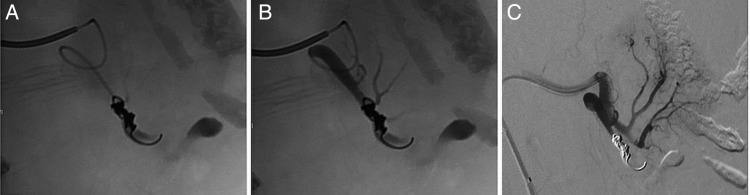
(A) Contrast arteriogram demonstrating successful deployment of embolisation coil into feeder artery proximal to the RAP. (B) Postembolisation contrast arteriogram demonstrates preservation of flow to branching vessels proximal to the coil and stagnant contrast distal to the coil. (C) Postembolisation contrast arteriogram demonstrates no further RAP perfusion or arteriovenous fistula flow and perfusion of remainder of the kidney.
Outcome and follow-up
Postembolisation, creatinine remained stable at 1.97 mg/dL. Additionally, serial haemoglobin and vital signs remained stable. After the procedure her haematuria did not recur and the patient was discharged home in stable condition 2 days after embolisation. She continues to do well at the time of last follow-up at 6 months, with complete resolution of abdominal pain, haemoglobin 11.9 mg/dL and creatinine 1.6 mg/dL.
Discussion
This case highlights the successful utilisation of CO2 in arteriography and embolisation for the treatment of RAP in the context of CKD, with no periprocedural acute kidney injury.
RAP is reported in 1–1.96% of patients after partial nephrectomy, presenting on average on POD 15, with gross haematuria in 87.3%.6 RAP is thought to result from disruption of the arterial wall with sustained arterial pressures dissecting into the adjacent tissues forming a sac that is contained by media or adventitia and communicates with the feeder artery.7
The diagnosis and treatment of RAP can be challenging in patients with CKD, in whom iodinated contrast may induce significant acute renal insufficiency requiring dialysis. Alternative diagnostic modalities include non-contrast CT, non-contrast MRA or US.7 Treatment options for RAP include observation, embolisation and rarely, nephrectomy. Embolisation is effective in 96% of patients6 but requires angiographic mapping of the renal vasculature with contrast.8 Iodinated contrast use in angiography and CT results in acute renal injury in 10% of patients with creatinine levels of 1.3–1.9 mg/dL, and up to 62% in those with levels greater than 2 mg/dL.4
Intra-arterial use of CO2 was first described by Hawkins9 and has been effectively used in a variety of diagnostic and interventional procedures.10 Unlike contrast, which mixes with blood, CO2 displaces blood, effectively reducing the attenuation of the blood vessel.11 Image quality using CO2 is typically reduced relative to iodinated contrast, but is sufficient for most procedures.11 In certain situations, small supplemental doses of contrast can assist in delineating the vasculature.10 One study has reported use of CO2 angiography in 700 patients with no significant decline in renal function in patients, including the subgroup with serum creatinine level ≥2 mg/dL.10
Although CO2 angiography avoids nephrotoxicity, certain complications have been described and theorised. In patients with respiratory failure, there is a theoretical risk of exacerbating CO2 retention. This can be prevented with reduced volume of CO2 and adequate time between injections.11 Another risk includes cerebral infarction, which can be prevented by avoiding use of CO2 above the diaphragm and in patients with a right-to-left intracardiac shunt.11 A phenomenon termed vapour lock, or trapping of gas in the non-dependent vasculature, has been reported in four case reports in the literature.10 It can be broken by changing the patient's position or by aspirating any trapped CO212 and prevented by using a closed CO2 injection system to avoid contamination with room air.10 Overall, CO2 is a safe, non-nephrotoxic alternative to traditional iodinated contrast angiography, with potential applications with RAP and CKD.
Learning points.
Renal artery pseudoaneurysm (RAP) is a rare complication of partial nephrectomy, which presents with haematuria, on an average of 15 days after surgery.
Superselective renal vessel coil embolisation is the first-line treatment for RAP.
CO2 is a safe, non-nephrotoxic alternative to traditional iodinated contrast arteriography, for the definitive treatment of RAP in patients with chronic kidney disease.
Footnotes
Contributors: All authors made contributions to acquisition of data, however, MAS primarily accomplished this. SAR contributed the majority of the images. All members contributed to drafting the manuscript, and there was major input regarding the revisions from all authors. All the authors have thoroughly reviewed the final draft and checked to be accurate to the best of their knowledge.
Competing interests: None.
Patient consent: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Parsons JK, Schoenberg MP. Renal artery pseudoaneurysm occurring after partial nephrectomy. Urology 2001;58:105. [DOI] [PubMed] [Google Scholar]
- 2.Pan H, Xia D, Wang S et al. . Embolization of renal artery pseudoaneurysm following laparoscopic partial nephrectomy for central renal tumor: a report of two cases. Oncol Lett 2014;7:2118–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bui BT, Oliva VL, Peloquin F et al. . Correction of deteriorating renal function by superselective embolization of an arcuate renal artery pseudoaneurysm. J Urol 1994;152:2087–8. [DOI] [PubMed] [Google Scholar]
- 4.Hall KA, Wong RW, Hunter GC et al. . Contrast-induced nephrotoxicity: the effects of vasodilator therapy. J Surg Res 1992;53:317–20. [DOI] [PubMed] [Google Scholar]
- 5.Kariya S, Tanigawa N, Kojima H et al. . Efficacy of carbon dioxide for diagnosis and intervention in patients with failing hemodialysis access. Acta Radiol 2010;51:994–1001. [DOI] [PubMed] [Google Scholar]
- 6.Jain S, Nyirenda T, Yates J et al. . Incidence of renal artery pseudoaneurysm following open and minimally invasive partial nephrectomy: a systematic review and comparative analysis. J Urol 2013;189:1643–8. [DOI] [PubMed] [Google Scholar]
- 7.Saad NE, Saad WE, Davies MG et al. . Pseudoaneurysms and the role of minimally invasive techniques in their management. Radiographics 2005;25(Suppl 1):S173–89. [DOI] [PubMed] [Google Scholar]
- 8.Loffroy R, Rao P, Kwak BK et al. . Transcatheter arterial embolization in patients with kidney diseases: an overview of the technical aspects and clinical indications. Korean J Radiol 2010;11:257–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hawkins IF. Carbon dioxide digital subtraction arteriography. AJR 1982;139: 19–24. [DOI] [PubMed] [Google Scholar]
- 10.Moos JM, Ham SW, Han SM et al. . Safety of carbon dioxide digital subtraction angiography. Arch Surg 2011;146:1428–32. [DOI] [PubMed] [Google Scholar]
- 11.Shaw DR, Kessel DO. The current status of the use of carbon dioxide in diagnostic and interventional angiographic procedures. Cardiovasc Intervent Radiol 2006;29:323–31. [DOI] [PubMed] [Google Scholar]
- 12.Nadolski GJ, Stavropoulos SW. Contrast alternatives for iodinated contrast allergy and renal dysfunction: options and limitations. J Vasc Surg 2013;57:593–8. [DOI] [PubMed] [Google Scholar]