

Abstract
Purpose
Internet support group (ISG) members benefit from receiving social support and, according to the helper therapy principle, by providing support to others. To test the mental health benefits of providing support to others, this trial compared the efficacy of a standard ISG (S-ISG) and an enhanced prosocial ISG (P-ISG).
Methods
A two-armed randomized controlled trial with 1-month pretest and post-test assessments was conducted with women (N = 184) diagnosed in the past 36 months with nonmetastatic breast cancer who reported elevated anxiety or depression. Women were randomly assigned to either the S-ISG or P-ISG condition. Both conditions included six professionally facilitated live chat sessions (90-minute weekly sessions) and access to an asynchronous discussion board; P-ISG also included structured opportunities to help and encourage others.
Results
Relative to the S-ISG, participants in the P-ISG condition exhibited more supportive behaviors (emotional, informational, and companionate support), posted more messages that were other-focused and fewer that were self-focused, and expressed less negative emotion (P < .05). Relative to the S-ISG, participants in the P-ISG condition had a higher level of depression and anxiety symptoms after the intervention (P < .05).
Conclusion
Despite the successful manipulation of supportive behaviors, the P-ISG did not produce better mental health outcomes in distressed survivors of breast cancer relative to an S-ISG. The prosocial manipulation may have inadvertently constrained women from expressing their needs openly, and thus, they may not have had their needs fully met in the group. Helping others may not be beneficial as a treatment for distressed survivors of breast cancer.
INTRODUCTION
Information and emotional support are associated with positive psychological adjustment in patients with breast cancer,1 but access to support is not universal.2 Internet support groups (ISGs) can increase access to psychosocial support, yet trials of cancer ISGs have yielded mixed results.3 Thus, there is a need to enhance the effectiveness of cancer ISGs to better serve patients. Cancer ISGs provide the benefit of access to support, but also provide opportunities to give support to others. The helper therapy principle4 asserts that helping others can enhance psychological and physical health in the helper.5 Theorists speculate that helping others may be a mechanism through which cancer support groups improve patient outcomes.6,7 On the basis of this theory, we hypothesized that an ISG that boosts opportunities for helping might be more effective at reducing distress symptoms than a standard ISG (S-ISG) that emphasizes support seeking through the expression of personal experiences and feelings.
Psychological distress is highly prevalent in patients with breast cancer.8,9 In a 5-year study of women with early-stage breast cancer, nearly half had depression, anxiety, or both 1 year after diagnosis, and 25% experienced depression and/or anxiety in the second, third, and fourth years.10 Managing distress is important in its own right, but it may be warranted for clinical reasons, too. Elevated distress in patients with cancer is associated with poorer quality of life, treatment adherence, surveillance, and self-care.8,9,11,12
Evidence on the efficacy of psychosocial interventions designed to reduce distress is growing.13–15 However, interventions that require one-on-one or face-to-face contact are costly and may not appeal to everyone, particularly those constrained by time, money, or mobility.16 Because ISGs are administered over the Internet, they are a relatively low-cost, low-stigma, and accessible mode of intervention.
Breast cancer ISGs are popular,17,18 but evidence on their efficacy is mixed.3 One randomized trial19 and one uncontrolled trial20 showed significant reductions in depression symptoms among patients with breast cancer participating in facilitated ISGs. Trials without a facilitator have shown less positive results. For example, a comparison of women randomly assigned to a nonfacilitated breast cancer ISG or to an Internet-based education control group revealed no group differences in distress.21 The mixed findings in this field warrant more research.
To our knowledge, this is the first trial to test the psychological benefits of increasing helping behaviors in cancer ISGs. We hypothesized that relative to patients assigned to an S-ISG, those assigned to a prosocial ISG (P-ISG) would have lower depression and anxiety after intervention. We predicted that P-ISG participants would exhibit more supportive behaviors than S-ISG participants. We also predicted that because the P-ISGs emphasized helping others, whereas the S-ISGs emphasized self-expression and self-help, the P-ISG group would use more other-focused language, less negative emotion, and more positive emotion. Observational studies suggest that would-be supporters of patients with cancer will often suppress negative thoughts and feelings.22 Finally, we predicted that the acceptability of the two interventions would be equivalent, as indicated by ratings of the intervention helpfulness and participation levels.
METHODS
Study Population
The sampling frame was generated in conjunction with a State Cancer Tumor Registry, targeting women meeting age and diagnostic criteria. Advance letters were sent to random women on the registry list. Respondents were screened for eligibility and consented via phone. Eligibility inclusion criteria included the following: stage I or II breast cancer in past 36 months; age 21 to 65 years; Internet access; fluency in English; and distressed (scoring above normal [≥ 8] for levels of depression or anxiety on the Hospital Anxiety and Depression Scale [HADS]).23 The study was conducted between 2011 and 2012.
Procedures
A two-group, randomized controlled trial design with 1-month pretest and post-test measures was used. Temple University's Institutional Review Board approved the protocol. Data were collected via structured telephone interviews by researchers who were blind to condition. Because age relates to Internet use24 and distress in patients with cancer,25 age-stratified permuted block random assignment (< v ≥ 51 years) was used. The Stata 13.1 (STATA Corp, College Station, TX) random number generator was used to create random sequence. Allocations were recorded on paper sealed in opaque envelopes controlled by the project director. Participants who completed a baseline interview were referred to the project director, who opened the next randomization envelope, added the participant to the allocated group roster, and e-mailed the roster to the facilitator. The project director e-mailed participants an ISG user's guide, a chat schedule, and a handout of tips on getting support in an ISG. Groups varied from 14 to 17 members (median, 15 members). Twelve groups were run, half S-ISG and half P-ISG.
There were two facilitators per condition. Postintervention debriefing interviews confirmed that facilitators were blind to study hypotheses. Facilitators managed operations and participation. These graduate-level health professionals had ≥ 10 years experience running ISGs. Trained researchers used checklists to review each weekly chat transcript to code facilitators' treatment fidelity on eight intervention components. Co-investigators, both PhD-level clinical psychologists with experience supervising ISGs, conducted weekly online facilitator supervision.
Interventions
Interventions were manualized and shared many features. In both conditions, groups had weekly, 90-minute live (synchronous) chats for 6 weeks. The facilitator introduced chat topics, which included the following: pain, fatigue, and lymphedema; self-esteem and body image; problems in physical activities; intimacy and sexuality; depression, anxiety, and recurrence fear; and health challenges (eg, diet, exercise, surveillance). Chat transcripts were posted within 24 hours so participants could review the sessions. The discussion board was always available for asynchronous text communication.
S-ISG intervention.
The S-ISG condition was based on empirically validated facilitated ISGs,19,20 which emphasized the exchange of information and emotional support between peers, normalization of experiences, and promotion of skills and confidence to effect positive life changes. In addition, as a control for the helpful blog activity in the P-ISG condition (see next paragraph), participants were asked to select one chat topic to write about in a private journal as a way to organize their thoughts and feelings. As an attention control for the e-card outreach activity in the P-ISG condition (see next paragraph), participants received a breast cancer informational flyer.
P-ISG intervention.
The P-ISG intervention included all elements of the S-ISG but with critical additions. Participants received written tips on how to recognize and respond to others' needs for support online. They received weekly e-mails describing chat topics (eg, fatigue) along with instructions to prepare one to two sentences on how their experiences with the chat topic might help others to cope. The facilitator promoted helping by doing the following: highlighting group members' requests for support; encouraging helping behaviors; and praising helping behaviors. Participants also were asked to post to the discussion board a helpful blog on any chat topic. They could offer information and advice or simply share their experience as a way to normalize others' experience. Finally, the P-ISG promoted helping through a breast cancer awareness outreach activity that required sending a mammogram e-card developed by the Centers for Disease Control and Prevention to women friends.
Measures
At each assessment, distress was measured using the HADS measure of anxiety and depression, which has been validated with breast cancer populations.26 The HADS provides continuous measures of symptoms of depression (seven items; α = .83) and anxiety (seven items; α = .83).
At follow-up assessment, perceived helpfulness of the interventions was assessed using nine face-valid questions with 5-point Likert-type scales (1 = not at all to 5 = very much), with three items on helpfulness of received support (α = .91), three items on helpfulness of being able to provide support (α = .91), and three items on helpfulness of hearing other women's experiences (α = .91).
As a manipulation check, research assistants used chat and discussion board transcripts to code the following three types of support behaviors: emotional support, informational support, and companionate support. The coding scheme was based on Bambina's Support OnLine coding scheme.27 Number of posts of each support type and a summary score of total supportive posts were calculated. Coders were kept blind to condition by removing facilitator comments. Randolph's28 free marginal multirater κ was used to calculate inter-rater reliability in coding support categories (emotional, informational, companionship; κ = .82). Finally, the Linguistic Inquiry and Word Count29 text analysis program was used to count the total number of words expressed, the number of negative and positive emotion words expressed, and the number of times first-person (eg, I, me) and second-person (eg, you, you'll) personal pronouns were expressed in chat or the discussion board.
Measures of potential control variables included baseline self-reported demographic and medical background variables, comorbid health conditions,30 perceived social support (α = .93),31 and received formal (eg, counseling) and informal (eg, other support groups) psychosocial intervention.
Symptoms of depression and anxiety were the primary and secondary outcomes, respectively. Study sample size was determined for the primary outcome. We assumed an effect size of at least d = 0.41 (75% of effect size reported in a previous trial using a waitlist control group and depression symptoms as an outcome19), pre-post correlations of at least 0.5, and intraclass correlation coefficients within group of 0.02 (six groups per condition, approximately 15 participants per group). Thus, a sample size of 180 participants (90 participants per condition) would yield an effective sample size of 140, sufficient to detect an effect size of at least d = 0.41, with power = .8 and α = .05. Minimum detectable effects for other outcomes based on this fixed sample size range between d = 0.34 and d = 0.46 for pre-post correlations of 0.7 and 0.3, respectively.
Data Analysis
Descriptive statistics included estimation of means and standard deviations for continuous variables and frequencies/cross-tabulations for categorical variables. Randomly assigned groups were compared on baseline variables using t tests (continuous variables) and χ2 tests (categorical variables). Associations were examined using Pearson's product moment correlations. Outcome analyses used multiple imputations (MIs) to account for missing data.32 Baseline values of response variables, group membership (ie, group 1 to 12), experimental condition, and variables associated with probability of missing response variables (partnered status, education, and age) were included as covariates in models or used to generate 20 multiple imputations based on the highest fraction of missing information, which was < .20 for all model parameters. Results across imputations were combined using Rubin's33 rules for MI inference. The primary study hypothesis was tested via a mixed-effects regression framework under an intent-to-treat framework. Models were adjusted for baseline symptoms, treatment condition, and perceived social support, with group membership treated as a random effect. Neither baseline × treatment interaction nor group membership effects were significant, and thus, results from two ordinary least squares regression models were reported for depression (primary outcome) and anxiety symptoms (secondary outcome). Analyses were performed using Stata 13.1 (STATA Corp). We set the level of significance at α = .05 and used the Benjamini-Hochberg34 false discovery rate correction for multiple comparisons (corrected probabilities = .028 for both depression and anxiety symptoms).
RESULTS
Sample Characteristics
Of the 669 women assessed for eligibility, 66% were ineligible, 7% refused participation, and 28% were randomly assigned after baseline assessment (Fig 1). Of the 184 women randomly assigned, 87% received the allocated intervention and 87% completed the follow-up assessment.
Fig 1.

CONSORT diagram of participant flow. (*) One person inadvertently accessed the wrong Internet support group because of a password typographical error and was excluded from analysis. P-ISG, prosocial Internet support group; S-ISG, standard Internet support group.
Table 1 lists the baseline sample characteristics. There were no statistically significant (all P > .05) differences between intervention conditions on any variables (Table 1), with the once exception that the P-ISG condition had significantly higher perceived social support than the S-ISG condition. Further, perceived social support was inversely correlated with depression symptoms before (r = −0.49, P < .001) and after intervention (r = −0.43, P < .001) and with anxious symptoms before (r = −0.20, P = .006) and after intervention (r = −0.25, P = .002). Thus, baseline perceived social support was statistically controlled in inferential analyses. Baseline variables in Table 1 did not differ significantly (all P > .05) between participants who were lost to follow-up (n = 23) and participants who completed the postintervention assessment (n = 160).
Table 1.
Baseline Demographics and Clinical Characteristics of Sample

| Demographic or Clinical Characteristic | S-ISG Group (n = 95) |
P-ISG Group (n = 88) |
P | ||
|---|---|---|---|---|---|
| No. of Participants | %* | No. of Participants | %* | ||
| Age in years | .39 | ||||
| Mean | 52.73 | 51.75 | |||
| SD | 6.95 | 8.44 | |||
| White | 91 | 52.3 | 83 | 47.2 | .65 |
| Educational attainment | |||||
| High school graduate | 50 | 27.3 | 43 | 23.5 | .61 |
| College graduate | 45 | 24.6 | 45 | 24.6 | |
| Employed part or full time | 66 | 52.4 | 60 | 47.6 | .85 |
| Married/in marital-like relation | 83 | 53.2 | 73 | 46.8 | .40 |
| Stage of cancer | |||||
| I | 55 | 54.5 | 46 | 45.5 | .45 |
| II | 40 | 48.8 | 42 | 51.2 | |
| Months since diagnosis | .19 | ||||
| Mean | 24.41 | 23.00 | |||
| SD | 6.90 | 7.62 | |||
| Surgical treatment | 91 | 52.3 | 83 | 47.7 | .65 |
| Chemotherapy treatment | 66 | 55.5 | 53 | 44.5 | .19 |
| Radiotherapy treatment | 61 | 48.8 | 64 | 51.2 | .22 |
| Hormonal treatment | 72 | 52.2 | 66 | 47.8 | .90 |
| Comorbid conditions, No. | .67 | ||||
| Mean | 2.01 | 1.95 | |||
| SD | 1.53 | 1.58 | |||
| Perceived social support | .047 | ||||
| Mean | 39.36 | 41.16 | |||
| SD | 6.52 | 5.59 | |||
| Receiving psychosocial care outside of trial | 27 | 47.4 | 30 | 52.6 | .41 |
| Depression symptoms | .33 | ||||
| Mean | 7.20 | 6.64 | |||
| SD | 3.85 | 3.80 | |||
| Anxiety symptoms | .23 | ||||
| Mean | 10.12 | 10.68 | |||
| SD | 3.02 | 3.31 | |||
Abbreviations: P-ISG, prosocial Internet support group; SD, standard deviation; S-ISG, standard Internet support group.
Percentages are rounded to nearest tenth.
Treatment Fidelity and Manipulation Checks
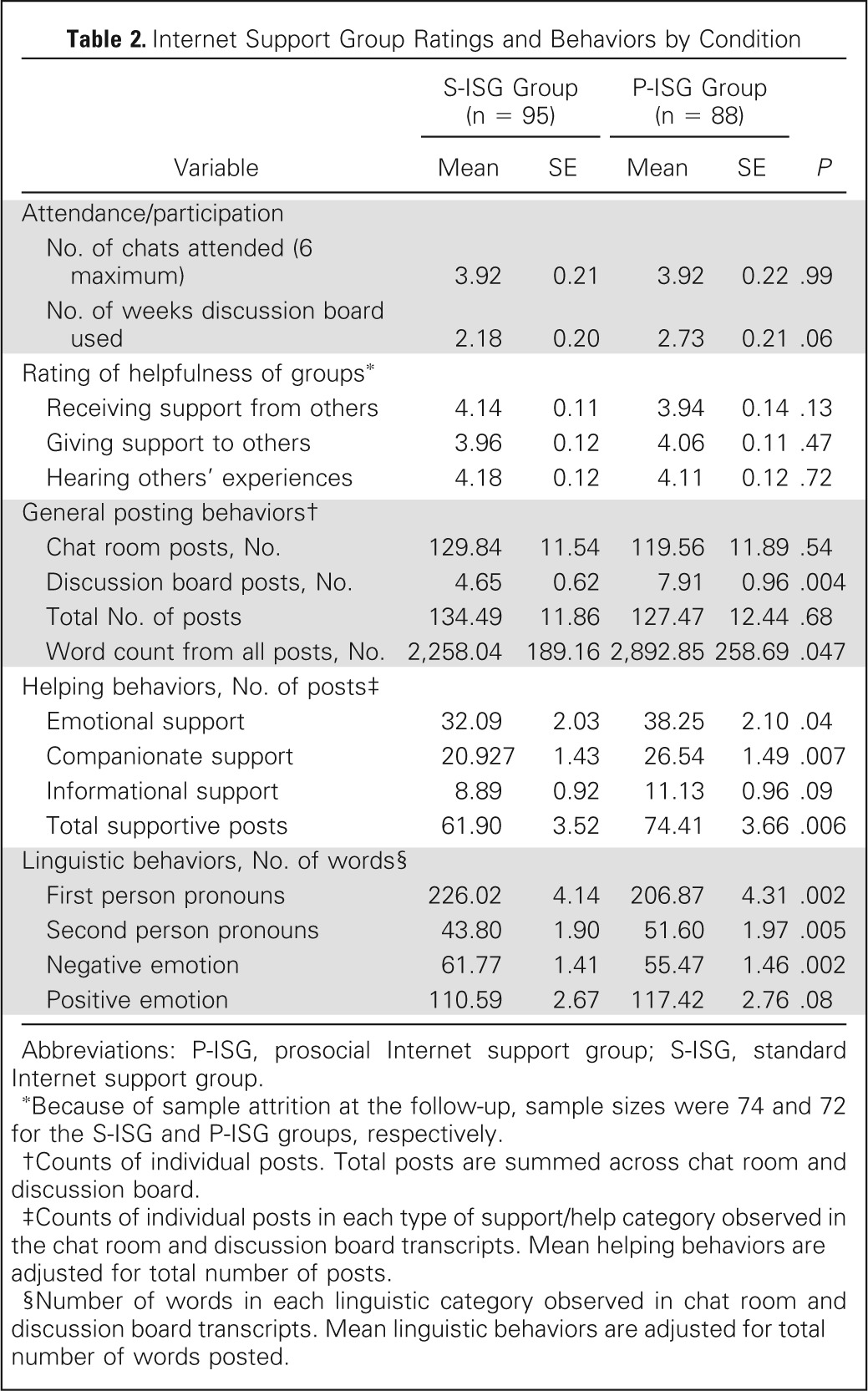
The mean level of facilitators' adherence to protocol was high in the S-ISG (mean, 95% adherent; standard deviation, 3.01) and P-ISG (mean, 97% adherent; standard deviation, 2.07) conditions. As shown in Table 2, chat attendance (P = .99) and discussion board participation (P = .06) did not differ significantly across condition. The number of posts in chat did not differ significantly across conditions (P = .54), whereas the number of discussion board posts was significantly higher in the P-ISG condition (P = .004). The total number of posts did not differ between conditions (P = .68), but the total number of words posted was significantly higher in the P-ISG condition (P = .047).
Table 2.
Internet Support Group Ratings and Behaviors by Condition
| Variable | S-ISG Group (n = 95) |
P-ISG Group (n = 88) |
P | ||
|---|---|---|---|---|---|
| Mean | SE | Mean | SE | ||
| Attendance/participation | |||||
| No. of chats attended (6 maximum) | 3.92 | 0.21 | 3.92 | 0.22 | .99 |
| No. of weeks discussion board used | 2.18 | 0.20 | 2.73 | 0.21 | .06 |
| Rating of helpfulness of groups* | |||||
| Receiving support from others | 4.14 | 0.11 | 3.94 | 0.14 | .13 |
| Giving support to others | 3.96 | 0.12 | 4.06 | 0.11 | .47 |
| Hearing others' experiences | 4.18 | 0.12 | 4.11 | 0.12 | .72 |
| General posting behaviors† | |||||
| Chat room posts, No. | 129.84 | 11.54 | 119.56 | 11.89 | .54 |
| Discussion board posts, No. | 4.65 | 0.62 | 7.91 | 0.96 | .004 |
| Total No. of posts | 134.49 | 11.86 | 127.47 | 12.44 | .68 |
| Word count from all posts, No. | 2,258.04 | 189.16 | 2,892.85 | 258.69 | .047 |
| Helping behaviors, No. of posts‡ | |||||
| Emotional support | 32.09 | 2.03 | 38.25 | 2.10 | .04 |
| Companionate support | 20.927 | 1.43 | 26.54 | 1.49 | .007 |
| Informational support | 8.89 | 0.92 | 11.13 | 0.96 | .09 |
| Total supportive posts | 61.90 | 3.52 | 74.41 | 3.66 | .006 |
| Linguistic behaviors, No. of words§ | |||||
| First person pronouns | 226.02 | 4.14 | 206.87 | 4.31 | .002 |
| Second person pronouns | 43.80 | 1.90 | 51.60 | 1.97 | .005 |
| Negative emotion | 61.77 | 1.41 | 55.47 | 1.46 | .002 |
| Positive emotion | 110.59 | 2.67 | 117.42 | 2.76 | .08 |
Abbreviations: P-ISG, prosocial Internet support group; S-ISG, standard Internet support group.
Because of sample attrition at the follow-up, sample sizes were 74 and 72 for the S-ISG and P-ISG groups, respectively.
Counts of individual posts. Total posts are summed across chat room and discussion board.
Counts of individual posts in each type of support/help category observed in the chat room and discussion board transcripts. Mean helping behaviors are adjusted for total number of posts.
Number of words in each linguistic category observed in chat room and discussion board transcripts. Mean linguistic behaviors are adjusted for total number of words posted.
Because P-ISG members tended to post more than S-ISG members, total number of posts was covaried in analyses of helping behaviors. As shown in Table 2, women in the P-ISG condition posted more messages that provided emotional support (P = .036) and companionate support (P = .007). The number of posts providing informational support was also higher in the P-ISG condition than in the S-ISG condition, but the difference was not significant (P = .09). The number of supportive posts of all kinds was significantly higher in the P-ISG condition than in the S-ISG condition (P = .006).
Because P-ISG members wrote more words than S-ISG members, overall number of words was covaried in analyses of linguistic behaviors. As shown in Table 2, women in the P-ISG condition used fewer self-referencing, first-person pronouns (P = .002) and more other-referencing, second-person pronouns (P = .005). The number of negative emotion words was lower in the P-ISG condition (P = 002). The number of positive emotion words was higher in the P-ISG condition, but the between-group difference was not significant (P = .08).
Table 2 also shows that the perceived helpfulness of intervention elements did not vary significantly by condition. The average helpfulness score of the different components was approximately 4 (quite a bit).
Outcome Analyses
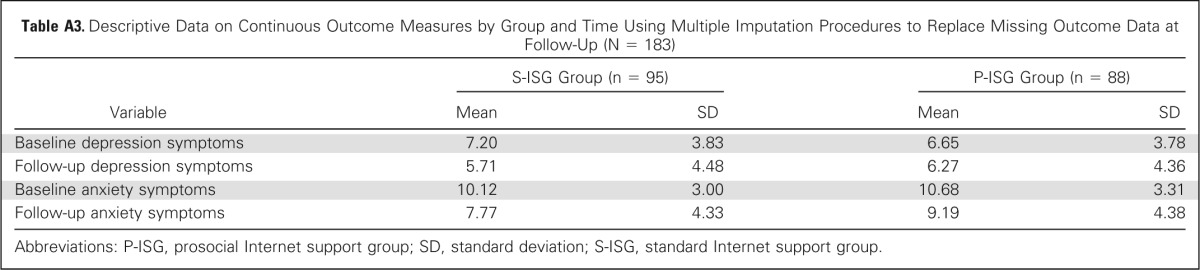
Intent-to-treat results for depression and anxiety symptoms are listed in Table 3. All covariates were significantly related to postintervention symptoms. Baseline symptoms were positively related to postintervention symptoms, whereas baseline level of social support was inversely related to level of postintervention symptoms (all P < .05). There was a significant effect of condition on postintervention symptoms, controlling for baseline symptoms and perceived social support (all P < .05). However, the effects were opposite of prediction; the S-ISG condition was associated with lower symptoms of depression and anxiety (a little more than 1 unit less) than the P-ISG condition. Sensitivity analyses showed that regression analyses using listwise deletion and last observation carried forward produced results similar to those using MI to address missing data (Appendix, online only).35
Table 3.
Results of Intent-To-Treat Analyses of Intervention Effects on Continuous Depression and Anxiety Symptoms Using Linear Regression (N = 183)

| Variable | Depression Symptoms at Follow-Up |
Anxiety Symptoms at Follow-Up |
||||
|---|---|---|---|---|---|---|
| B* | 95% CI | P | B* | 95% CI | P | |
| Baseline symptoms† | 0.65 | 0.48 to 0.83 | .001 | 0.62 | 0.45 to 0.80 | .001 |
| Perceived support | −0.10 | −0.19 to −0.02 | .022 | −0.12 | −0.22 to −0.03 | .012 |
| Condition‡ | 1.11 | 0.12 to 2.11 | .028 | 1.28 | 0.16 to 2.41 | .025 |
| Constant | 5.08 | 0.85 to 9.30 | .019 | 6.26 | 1.95 to 10.57 | .005 |
Unstandardized coefficients.
Level of baseline anxiety symptoms was covaried in analyses when anxiety symptoms were the outcome, whereas level of baseline depressive symptoms was covaried in analyses when depressive symptoms were the outcome.
Condition: standard Internet support group = 0, prosocial Internet support group = 1.
DISCUSSION
The goal of this trial was to evaluate the relative efficacy of an S-ISG compared with a novel P-ISG for improving the mental health of distressed women treated for breast cancer. Both interventions were acceptable based on participation levels and subjective helpfulness ratings. Relative to the standard intervention, the prosocial intervention increased helping behaviors and communication that was more other-focused and had less negative emotional content. Despite successfully increasing helping, the prosocial intervention resulted in poorer psychological outcomes than the standard intervention.
Consistent with prior research,19,20 the findings from this study suggest that professionally facilitated ISGs may be beneficial to women's mental health. However, the findings fail to support the theory that helping others is effective at promoting mental health. There is only one published study,36 to our knowledge, that has experimentally tested the benefits of helping in a cancer population. In that study, patients who underwent hematopoietic stem-cell transplantation were randomly assigned to one of the following four writing conditions: peer helping (sharing experiences in writing to help others prepare for transplantation), expressive writing (expressing thoughts and feelings about transplantation in writing), expressive helping (combination of peer helping and expressive writing), or neutral writing (writing a factual account of transplantation). There were no main effects of condition on distress. Subgroup analyses showed that among participants with elevated survivorship problems, expressive helping reduced distress relative to peer helping and neutral writing. The expressive helping condition is similar to our prosocial condition, which includes both opportunities for expressing feelings and helping others. However, in the expressive helping condition, the expression of emotions was private, whereas in the prosocial condition, the expression of emotions was in a group forum. Thus, unlike participants in the prosocial condition, those in the expressive helping condition did not need to worry that expressing their negative emotions might adversely affect others.
For women in this trial, the opportunity to participate in a support group may have been a unique chance to talk freely with empathic others without having to worry about rejection or burdening others.37 However, adding a prosocial emphasis to the ISG may have inadvertently raised participants' concerns about burdening others with their problems. Patients with cancer can sometimes feel constrained in talking about their cancer-related concerns and fears because they do not want to upset others.2,38 Similar social constraints may arise in a breast cancer support group. In trying to be supportive toward others in the prosocial intervention, women may have felt a need to suppress their own negative feelings and increase their expression of positive feelings. The linguistic analyses of negative and positive emotion are consistent with this interpretation.
The present results do not confirm the widely held assumption6,7,39 that helping others is a key mechanism through which support groups improve psychological outcomes. More generally, the results fail to support the helper therapy principle. Many past studies of the helper therapy principle have used cross-sectional correlational data and rarely have included clinical populations.5 It is possible that some reported associations between helping behaviors and health reflect a reverse or spurious causal relation. It is also possible that helping others is only beneficial when it is not a burden40 or does not interfere with other therapeutic processes.
Several study limitations are noteworthy. First, the lack of a usual-care control group prevents us from estimating the amount of symptom improvement that is attributable to natural recovery. Second, the reliance on self-report data for the primary outcomes is a limitation, but keeping assessors blind to condition and assigning interventionists to one intervention condition minimized self-report bias as a result of experimental artifacts. To further control for bias, interventionists and participants were not told the study hypotheses. Finally, the focus on distressed patients treated for nonmetastatic breast cancer limits the generalizability of the findings.
In conclusion, the results of this trial do not support the hypothesis that boosting prosocial elements of a facilitated S-ISG will improve psychological outcomes in distressed survivors of breast cancer. Indeed, adding a prosocial emphasis may impede emotional recovery and constrain women's expression of their feelings, particularly negative emotions. The data suggest that the S-ISG conveyed some psychological benefits to participants, but the extent of benefit is difficult to determine without a usual-care control group.
Acknowledgment
We thank the women who took part in this trial and Anne Gessert, Michael States, Erika Maslan, Sue Meyn, Melissa Godfrey, Rachel Myers, Julianne Ani, Levi James, and Andrea Echeverri, who aided in the performance of the research.
Appendix
Appendix Tables A1 to A3 list descriptive data on outcome variables using various approaches to addressing missing data at follow-up, including listwise deletion of any patients missing at follow-up (Appendix Table A1), replacement of missing data at follow-up with values of variables at baseline (Appendix Table A2), and multiple imputation procedures (Appendix Table A3). Appendix Tables A4 and A5 list the results of linear regression analyses performed on outcomes using either listwise deletion of patients with missing data at follow-up or replacement of missing data at follow-up with values of variables at baseline, respectively. The results in Appendix Tables A4 and A5 are highly consistent with the results reported in the article (Table 3) using multiple imputation procedures to replace missing data on outcomes at follow-up.
Table A1.
Descriptive Data on Continuous Outcome Measures by Group and Time With No Replacement of Missing Data at Follow-Up (listwise deletion)

| Variable | S-ISG Group |
P-ISG Group |
||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Baseline depression symptoms* | 7.20 | 3.85 | 6.64 | 3.80 |
| Follow-up depression symptoms† | 5.77 | 4.34 | 6.13 | 4.21 |
| Baseline anxiety symptoms* | 10.12 | 3.02 | 10.68 | 3.31 |
| Follow-up anxiety symptoms† | 7.74 | 4.14 | 9.18 | 4.26 |
Abbreviations: P-ISG, prosocial Internet support group; SD, standard deviation; S-ISG, standard Internet support group.
N = 183 at pretest (S-ISG, n = 95; P-ISG, n = 88).
n = 160 at posttest (S-ISG, n = 82; P-ISG, n = 78).
Table A2.
Descriptive Data on Continuous Outcome Measures by Group and Time Using Baseline Values of Outcomes to Replace Missing Data Values at Follow-Up (last observation carried forward; N = 183)

| Variable | S-ISG Group (n = 95) |
P-ISG Group (n = 88) |
||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Baseline depression symptoms | 7.20 | 3.85 | 6.64 | 3.80 |
| Follow-up depression symptoms | 5.85 | 4.08 | 6.38 | 4.26 |
| Baseline anxiety symptoms | 10.12 | 3.02 | 10.68 | 3.31 |
| Follow-up anxiety symptoms | 8.11 | 4.01 | 9.50 | 4.28 |
Abbreviations: P-ISG, prosocial Internet support group; SD, standard deviation; S-ISG, standard Internet support group.
Table A3.
Descriptive Data on Continuous Outcome Measures by Group and Time Using Multiple Imputation Procedures to Replace Missing Outcome Data at Follow-Up (N = 183)
| Variable | S-ISG Group (n = 95) |
P-ISG Group (n = 88) |
||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Baseline depression symptoms | 7.20 | 3.83 | 6.65 | 3.78 |
| Follow-up depression symptoms | 5.71 | 4.48 | 6.27 | 4.36 |
| Baseline anxiety symptoms | 10.12 | 3.00 | 10.68 | 3.31 |
| Follow-up anxiety symptoms | 7.77 | 4.33 | 9.19 | 4.38 |
Abbreviations: P-ISG, prosocial Internet support group; SD, standard deviation; S-ISG, standard Internet support group.
Table A4.
Results of Analyses of Intervention Effects on Continuous Depression and Anxiety Symptoms Using Linear Regression and Listwise Deletion of Data From Participants Missing at Follow-Up (n = 160)

| Variable | Depression Symptoms at Follow-Up |
Anxiety Symptoms at Follow-Up |
||||
|---|---|---|---|---|---|---|
| B* | 95% CI | P | B* | 95% CI | P | |
| Baseline symptom† | 0.65 | 0.48 to 0.83 | .001 | 0.63 | 0.45 to 0.81 | .001 |
| Perceived support | −0.10 | −0.19 to −0.02 | .022 | −0.12 | −0.21 to −0.04 | .006 |
| Condition‡ | 1.16 | 0.17 to 2.15 | .022 | 1.42 | 0.29 to 2.55 | .014 |
| Constant | 5.01 | 0.76 to 9.27 | .021 | 6.28 | 2.15 to 10.42 | .003 |
Unstandardized coefficients.
Level of baseline anxiety symptoms was covaried in analyses when anxiety symptoms were the outcome, whereas level of baseline depressive symptoms was covaried in analyses when depressive symptoms were the outcome.
Condition: standard Internet support group = 0, prosocial Internet support group = 1.
Table A5.
Results of Analyses of Intervention Effects on Continuous Depression and Anxiety Symptoms Using Linear Regression and Replacing Missing Outcome Data at Follow-Up With Baseline Values of Variable (N = 183)

| Variable | Depression Symptoms at Follow-Up |
Anxiety Symptoms at Follow-Up |
||||
|---|---|---|---|---|---|---|
| B* | 95% CI | P | B* | 95% CI | P | |
| Baseline symptoms† | 0.69 | 0.53 to 0.84 | .001 | 0.68 | 0.52 to 0.85 | .001 |
| Perceived support | −0.09 | −0.17 to −0.01 | .031 | −0.11 | −0.19 to −0.02 | .012 |
| Condition‡ | 1.06 | 0.19 to 1.93 | .017 | 1.20 | 0.18 to 2.22 | .022 |
| Constant | 4.40 | 0.54 to 8.25 | .026 | 5.39 | 1.49 to 9.28 | .007 |
Unstandardized coefficients.
Level of baseline anxiety symptoms was covaried in analyses when anxiety symptoms were the outcome, whereas level of baseline depressive symptoms was covaried in analyses when depressive symptoms were the outcome.
Condition: standard Internet support group = 0, prosocial Internet support group = 1.
Footnotes
Supported by National Institutes of Health Grant No. R21CA15877.
Presented in part at the 2013 Annual Meeting of the International Society for Research on Internet Interventions, Chicago, IL, May 16-18, 2013 and the International Psycho-Oncology Society 14th World Congress of Psycho-Oncology, Brisbane, Queensland, Australia, November 13-15, 2012.
Clinical trial information: NCT01396174.
Authors' disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Disclosures provided by the authors are available with this article at www.jco.org.
AUTHOR CONTRIBUTIONS
Conception and design: All authors
Collection and assembly of data: Stephen J. Lepore, Joanne S. Buzaglo, Judith R. Greener
Data analysis and interpretation: Stephen J. Lepore, Morton A. Lieberman, Judith R. Greener, Adam Davey
Manuscript writing: All authors
Final approval of manuscript: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Comparing Standard Versus Prosocial Internet Support Groups for Patients With Breast Cancer: A Randomized Controlled Trial of the Helper Therapy Principle
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. For a detailed description of the disclosure categories, or for more information about ASCO's conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors.
Stephen J. Lepore
No relationship to disclose
Joanne S. Buzaglo
Consulting or Advisory Role: Genentech (Inst), Pfizer (Inst), Onyx (Inst), Celgene (Inst), Bristol-Myers Squibb (Inst)
Morton A. Lieberman
No relationship to disclose
Mitch Golant
No relationship to disclose
Judith R. Greener
No relationship to disclose
Adam Davey
No relationship to disclose
REFERENCES
- 1.Helgeson VS, Cohen S. Social support and adjustment to cancer: Reconciling descriptive, correlational, and intervention research. Health Psychol. 1996;15:135–148. doi: 10.1037//0278-6133.15.2.135. [DOI] [PubMed] [Google Scholar]
- 2.Lepore SJ, Revenson TA. Social constraints on disclosure and adjustment to cancer. Soc Personal Psychol Compass. 2007;1:1–20. [Google Scholar]
- 3.Hong Y, Peña-Purcell NC, Ory MG. Outcomes of online support and resources for cancer survivors: A systematic literature review. Patient Educ Couns. 2012;86:288–296. doi: 10.1016/j.pec.2011.06.014. [DOI] [PubMed] [Google Scholar]
- 4.Reissman F. The helper-therapy principle. Soc Work. 1965;10:27–32. [Google Scholar]
- 5.Post SG. Altruism and Health: Perspectives From Empirical Research. New York, NY: Oxford University Press; 2007. [Google Scholar]
- 6.Gottlieb BH, Wachala ED. Cancer support groups: A critical review of empirical studies. Psychooncology. 2007;16:379–400. doi: 10.1002/pon.1078. [DOI] [PubMed] [Google Scholar]
- 7.Campbell HS, Phaneuf MR, Deane K. Cancer peer support programs: Do they work? Patient Educ Couns. 2004;55:3–15. doi: 10.1016/j.pec.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 8.Reich M, Lesur A, Perdrizet-Chevallier C. Depression, quality of life and breast cancer: A review of the literature. Breast Cancer Res Treat. 2008;110:9–17. doi: 10.1007/s10549-007-9706-5. [DOI] [PubMed] [Google Scholar]
- 9.Fann JR, Thomas-Rich AM, Katon WJ, et al. Major depression after breast cancer: A review of epidemiology and treatment. Gen Hosp Psychiatry. 2008;30:112–126. doi: 10.1016/j.genhosppsych.2007.10.008. [DOI] [PubMed] [Google Scholar]
- 10.Burgess C, Cornelius V, Love S, et al. Depression and anxiety in women with early breast cancer: Five year observational cohort study. BMJ. 2005;330:702. doi: 10.1136/bmj.38343.670868.D3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment:Meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160:2101–2107. doi: 10.1001/archinte.160.14.2101. [DOI] [PubMed] [Google Scholar]
- 12.Shelby RA, Scipio CD, Somers TJ, et al. Prospective study of factors predicting adherence to surveillance mammography in women treated for breast cancer. J Clin Oncol. 2012;30:813–819. doi: 10.1200/JCO.2010.34.4333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Faller H, Schuler M, Richard M, et al. Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: Systematic review and meta-analysis. J Clin Oncol. 2013;31:782–793. doi: 10.1200/JCO.2011.40.8922. [DOI] [PubMed] [Google Scholar]
- 14.Jacobsen PB, Jim HS. Psychosocial interventions for anxiety and depression in adult cancer patients: Achievements and challenges. CA Cancer J Clin. 2008;58:214–230. doi: 10.3322/CA.2008.0003. [DOI] [PubMed] [Google Scholar]
- 15.Lepore SJ, Coyne JC. Psychological interventions for distress in cancer patients: A review of reviews. Ann Behav Med. 2006;32:85–92. doi: 10.1207/s15324796abm3202_2. [DOI] [PubMed] [Google Scholar]
- 16.Stephen J, Rojubally A, Macgregor K, et al. Evaluation of CancerChatCanada: A program of online support for Canadians affected by cancer. Curr Oncol. 2013;20:39–47. doi: 10.3747/co.20.1210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Davison KP, Pennebaker JW, Dickerson SS. Who talks? The social psychology of illness support groups. Am Psychol. 2000;55:205–217. [PubMed] [Google Scholar]
- 18.Owen JE, Goldstein MS, Lee JH, et al. Use of health-related and cancer-specific support groups among adult cancer survivors. Cancer. 2007;109:2580–2589. doi: 10.1002/cncr.22719. [DOI] [PubMed] [Google Scholar]
- 19.Winzelberg AJ, Classen C, Alpers GW, et al. Evaluation of an Internet support group for women with primary breast cancer. Cancer. 2003;97:1164–1173. doi: 10.1002/cncr.11174. [DOI] [PubMed] [Google Scholar]
- 20.Lieberman MA, Golant M, Giese-Davis J, et al. Electronic support groups for breast carcinoma: A clinical trial of effectiveness. Cancer. 2003;97:920–925. doi: 10.1002/cncr.11145. [DOI] [PubMed] [Google Scholar]
- 21.Salzer MS, Palmer SC, Kaplan K, et al. A randomized, controlled study of Internet peer-to-peer interactions among women newly diagnosed with breast cancer. Psychooncology. 2010;19:441–446. doi: 10.1002/pon.1586. [DOI] [PubMed] [Google Scholar]
- 22.Wortman CB, Dunkel-Schetter C. Interpersonal relationships and cancer: A theoretical analysis. J Soc Issues. 1979;35:120–155. [Google Scholar]
- 23.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 24.Zickuhr K. Who's not online and why. Pew Research Center's Internet and American Life Project, 2013. http://www.pewinternet.org/2013/09/25/whos-not-online-and-why/
- 25.Roberts KJ, Lepore SJ, Hanlon AL, et al. Genitourinary functioning and depressive symptoms over time in younger versus older men treated for prostate cancer. Ann Behav Med. 2010;40:275–283. doi: 10.1007/s12160-010-9214-4. [DOI] [PubMed] [Google Scholar]
- 26.Jacobsen PB, Donovan KA, Trask PC, et al. Screening for psychologic distress in ambulatory cancer patients. Cancer. 2005;103:1494–1502. doi: 10.1002/cncr.20940. [DOI] [PubMed] [Google Scholar]
- 27.Bambina A. Online Social Support: The Interplay of Social Networks and Computer-Mediated Communication. London, United Kingdom: Cambria Press; 2007. [Google Scholar]
- 28.Randolph JJ. Free-marginal multirater kappa (multirater K[free]): An alternative to Fleiss' fixed-marginal multirater kappa. Presented Joensuu Learning and Instruction Symposium; October 14-15, 2005; Joensuu, Finland. [Google Scholar]
- 29.Pennebaker JW, Booth RJ, Francis ME. Linguistic Inquiry and Word Count: LIWC 2007. http://liwc.net/
- 30.Sangha O, Stucki G, Liang MH, et al. The Self-Administered Comorbidity Questionnaire: A new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003;49:156–163. doi: 10.1002/art.10993. [DOI] [PubMed] [Google Scholar]
- 31.Cutrona CE, Russell D. The provisions of social relationships and adaptation to stress. In: Jones WH, Perlman D, editors. Advances in Personal Relationships. Greenwich, CT: JAI Press; 1987. pp. 37–67. [Google Scholar]
- 32.Davey A, Savla J. Statistical Power Analysis With Missing Data: A Structural Equation Modeling Approach. New York, NY: Routledge; 2009. [Google Scholar]
- 33.Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York, NY: John Wiley & Sons; 2004. [Google Scholar]
- 34.Benjamini Y, Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J R Stat Soc B. 1995;57:289–300. [Google Scholar]
- 35.National Research Council. The Prevention and Treatment of Missing Data in Clinical Trials. Washington, DC: The National Academies Press; 2010. [PubMed] [Google Scholar]
- 36.Rini C, Austin J, Wu LM, et al. Harnessing benefits of helping others: A randomized controlled trial testing expressive helping to address survivorship problems after hematopoietic stem cell transplant. Health Psychol. doi: 10.1037/hea0000024. [epub ahead of print on November 25, 2013] [DOI] [PubMed] [Google Scholar]
- 37.Ussher J, Kirsten L, Butow P, et al. What do cancer support groups provide which other supportive relationships do not? The experience of peer support groups for people with cancer. Soc Sci Med. 2006;62:2565–2576. doi: 10.1016/j.socscimed.2005.10.034. [DOI] [PubMed] [Google Scholar]
- 38.Lepore SJ. A social–cognitive processing model of emotional adjustment to cancer. In: Baum A, Andersen BL, editors. Psychosocial Interventions for Cancer. Washington, DC: American Psychological Association; 2001. pp. 99–116. [Google Scholar]
- 39.Proudfoot JG, Jayawant A, Whitton AE, et al. Mechanisms underpinning effective peer support: A qualitative analysis of interactions between expert peers and patients newly-diagnosed with bipolar disorder. BMC Psychiatry. 2012;12:196. doi: 10.1186/1471-244X-12-196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Post SG. Altruism, happiness, and health: It's good to be good. Int J Behav Med. 2005;12:66–77. doi: 10.1207/s15327558ijbm1202_4. [DOI] [PubMed] [Google Scholar]