

Abstract
Background and Objectives
Cryolipolysis procedures have been shown to safely and effectively reduce the thickness of fat in a treated region. This study was conducted to determine whether the addition of post-treatment manual massage would improve efficacy while maintaining the safety profile of the original cryolipolysis treatment protocol.
Materials and Methods
The study population consisted of an efficacy group (n = 10) and a safety group (n = 7). Study subjects were treated on each side of the lower abdomen with a Cooling Intensity Factor of 42 (−72.9 mW/cm2) for 60 minutes. One side of the abdomen was massaged post-treatment and the other side served as the control. Immediately post-treatment, the massage side was treated for 1 minute using a vigorous kneading motion followed by 1 minute of circular massage using the pads of the fingers. For the efficacy group, photos and ultrasound measurements were taken at baseline, 2 months, and 4 months post-treatment. For the safety group, histological analysis was completed at 0, 3, 8, 14, 30, 60, and 120 days post-treatment to examine the effects of massage on subcutaneous tissue over time.
Results
Post-treatment manual massage resulted in a consistent and discernible increase in efficacy over the non-massaged side. At 2 months post-treatment, mean fat layer reduction was 68% greater in the massage side than in the non-massage side as measured by ultrasound. By 4 months, mean fat layer reduction was 44% greater in the massage side. Histological results showed no evidence of necrosis or fibrosis resulting from the massage.
Conclusion
Post-treatment manual massage is a safe and effective technique to enhance the clinical outcome from a cryolipolysis procedure. Lasers Surg. Med. 46:20–26, 2014. © 2013 The Authors. Lasers in Surgery and Medicine Published by Wiley Periodicals, Inc.
Keywords: body contouring, cryolipolysis, non-surgical fat reduction, post-treatment massage
INTRODUCTION
Cryolipolysis is a novel non-invasive fat reduction technique that applies controlled localized cooling to the skin surface to reduce subcutaneous fat. Cryolipolysis procedures can safely and effectively reduce fat without damaging overlying skin or surrounding structures 1–3. While the mechanisms of fat reduction are not entirely understood, studies have shown that cold exposure induces apoptotic cell death of subcutaneous fat cells 4,5.
Cryolipolysis is approved by the FDA, Health Canada and the European Union as a non-invasive treatment for the reduction of localized subcutaneous fat 6. Recent studies have focused on improving and optimizing cryolipolysis treatment protocols to enhance the reduction of fat. Two studies suggest that a second successive course of treatment may improve the efficacy of this procedure 6. One study demonstrated, however, that a second treatment improved efficacy in the abdomen area but not the love handles 7. Because cryolipolysis is still a relatively new procedure, treatment protocols have yet to be refined and optimized to maximize results.
The purpose of this study is to evaluate whether the addition of a post-treatment manual massage enhances the effectiveness of a single cryolipolysis treatment. Additionally, this study evaluates the safety of incorporating post-treatment manual massage into cryolipolysis treatment.
METHODS
All studies were conducted using a commercially available non-invasive medical device for cryolipolysis (CoolSculpting, ZELTIQ Aesthetics, Pleasanton, CA). Subjects were selected from new patient consultations or referrals from friends and family. Study subjects received treatments free of charge but were not otherwise compensated. Prior to treatment, trained clinicians collected patient data including gender, weight, age, height, BMI, and medical history.
Subjects were screened based upon the following inclusion/exclusion criteria. Subjects included in the study had a visible bulge of adipose tissue on their abdomen below the umbilicus and stated willingness to maintain weight within 10 lbs for the duration of the study. No adjunctive fat reduction therapies were used over the course of the study. Subjects were excluded if they had undergone liposuction, other surgical procedures, or abdomen contouring treatments in the past 6 months. They were excluded for history of cryoglobulinemia, paroxysmal cold hemoglobinuria, cold urticaria, areas of impaired peripheral circulation, Raynaud's disease, pregnancy, scar tissue, or extensive skin conditions, such as eczema or dermatitis at the treatment area, impaired skin sensation, open or infected wounds, and area of recent bleeding or hemorrhage. Also, subjects with skin laxity or enrolled for other clinical studies were excluded.
Efficacy was determined using photographic and ultrasound analysis at 2 and 4 months post-treatment. Safety was evaluated from a separate group of 7 subjects by assessing side effects and analyzing histology. Subjects received cryolipolysis treatments prior to abdominoplasty surgery and the resected tissue underwent histology processing, imaging, and analysis.
Treatment Method
As illustrated in Figure 1, the cryolipolysis vacuum applicator was used to sequentially treat the left and right sides of the abdomen below the umbilicus for 60 minutes each. Immediately following cryolipolysis treatment, one side of the abdomen was manually massaged using a 2-minute protocol, while the remaining side served as a control.
Fig 1.
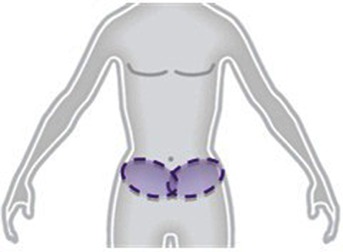
Cryolipolysis treatments were delivered using a vacuum applicator to the left and right sides of the lower abdomen. One side was manually massaged immediately post-treatment, while the other side was the non-massage control.
Cryolipolysis was administered to abdominal tissue drawn between cooled plates in the applicator. To ensure consistent thermal coupling between the skin and the applicator, a pad saturated with a coupling gel (ZELTIQ Aesthetics) was placed on the skin surface prior to placing the applicator on the abdomen. A medium applicator (CoolCore applicator) was applied with moderate vacuum pressure to gently draw a bulge of fat into the applicator cup. Treatment was delivered at a Cooling Intensity Factor 42, corresponding to an average energy extraction rate of 72.9 mW/cm2.
Immediately following treatment, one side of the abdomen was manually massaged for 2 minutes (Fig. 2). The side of the abdomen that received the massage was randomly assigned. The first minute of massage consisted of a vigorous kneading motion, during which the tissue was pulled together between the thumb and fingers and then pulled away from the body. The second minute of massage consisted of circular massage, during which tissue was pushed down into the body and then moved in a circular motion.
Fig 2.

Immediately following cryolipolysis treatment, the tissue was vigorously kneaded and pulled away from the body for 1 minute then pushed into the body in a circular massage motion for 1 minute.
Method of Evaluating Efficacy
The efficacy of adding a 2-minute manual massage following cryolipolysis was evaluated using pre- and post-treatment photographs and ultrasound measurement of fat layer reduction in the massaged and non-massaged sides. Both photographic and ultrasound images were taken at baseline, 2 months, and 4 months post-treatment.
Fat layer reduction, as demonstrated by fat layer thickness changes measured by ultrasound, was confirmed by comparing pre-treatment and post-treatment images, in which each ultrasound image pair corresponded to the same anatomic area. An ultrasound system (SonoSite TITAN, Bothell, WA) with a 7.5-MHz high-resolution linear transducer was used to acquire images of the fat layer. A series of evenly spaced pre-treatment images were acquired, as shown in Figure 3, with five images captured through the untreated control area in the upper abdomen and 10 through the treatment area in the lower abdomen. Overall fat layer thickness changes were normalized by subtracting the control site difference from the treated site difference. For each subject, multiple fat layer reduction measurements were obtained and averaged to determine a mean fat layer thickness change.
Fig 3.
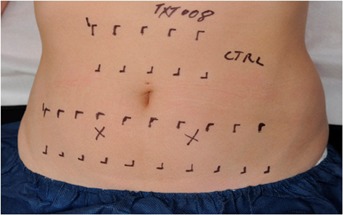
Ultrasound images were acquired of the cryolipolysis treated lower abdomen and the untreated control upper abdomen. Ten images were taken of the lower abdomen (five from the massaged side, five from the non-massaged side) and five images were taken from the control area.
Method of Evaluating Safety
The safety of adding a 2-minute manual massage immediately following cryolipolysis was assessed on a group of seven patients by monitoring procedural side effects and evaluation of tissue histology. Patients were assessed immediately following treatment (0 day) and 3, 8, 14, 30, 60, and 120 days post-treatment to evaluate damage to the dermis or epidermis in the areas treated. Histology has been used to assess cold-induced panniculitis at the dermal-fat interface following cryolipolysis treatment and to evaluate the time course of inflammatory activity 2,3. In this study, the histology was also evaluated for additional tissue injury induced by the post-treatment manual massage.
RESULTS
A total of 10 subjects were assessed for efficacy by baseline ultrasound and photography and seven subjects were evaluated for safety by histology. The analyzed patient population was entirely female with age range 30–50 years, weight range 129–147 lbs, BMI range 21–25, and height 5′2″ to 5′8″. All patients maintained body weight within the specified 10 lbs over the course of the study, ranging from a 6 lb loss to an 8 lb gain. Of the original 10 subjects treated for efficacy assessment, one was lost at 2 months follow-up and an additional subject was lost at 4 months follow-up; both subjects were lost due to inconvenience of follow-up rather than procedure-related adverse event or treatment failure.
Efficacy Results
For all subjects treated, the cryolipolysis procedure visibly reduced the size of the lower abdomen, as demonstrated by ultrasound measurements and photography. Figures 7 show photos taken at baseline, 2 months, and 4 months post-treatment.
Fig 7.
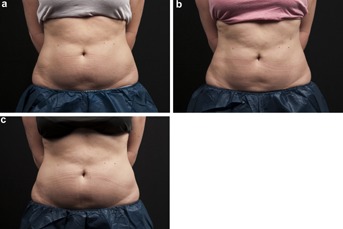
Subject #2 had post-treatment massage on left and non-massage control on right. Photographic analysis of post-treatment manual massage at baseline (a), 2-months (b), and 4-months (c) post-treatment.
Fig 4.
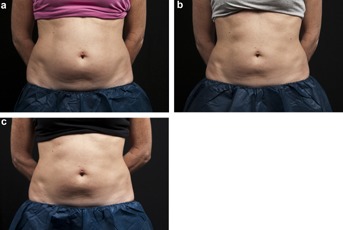
Subject #8 had post-treatment massage on left and non-massage control on right. Photographic analysis of post-treatment manual massage at baseline (a), 2-months (b), and 4-months (c) post-treatment.
Fig 5.
Subject #10 had post-treatment massage on left and non-massage control on right. Photographic analysis of post-treatment manual massage at baseline (a), 2-months (b), and 4-months (c) post-treatment.
Fig 6.

Subject #6 had post-treatment massage on left and non-massage control on right. Photographic analysis of post-treatment manual massage at baseline (a), 2-months (b), and 4-months (c) post-treatment.
Ultrasound measurements of fat reduction between massaged and non-massaged sites 2 months post-treatment are shown in Figure 8. In all patients at 2 months, there was a significant decrease in fat layer thickness on the side that was massaged post-treatment. The normalized mean fat layer reduction was 12.6% with standard deviation 7.2% and range −2.4 to 20.0% (mean 2.6 mm, standard deviation 1.9 mm, range −1.1 to 5.0 mm) for the non-massaged side and 21.0% with standard deviation 8.5% and range 10.0 to 34.9% (mean 4.2 mm, standard deviation 2.2 mm, range 0.8 to 7.2 mm) for the massaged side. Thus, mean fat reduction was 68% greater on the massaged side at 2 months. At 4 months post-treatment, the normalized mean fat layer reduction was 10.3% with standard deviation 8.6% and range −2.6 to 25.8% (mean 1.9 mm, standard deviation 1.1 mm, range 0.5 to 3.9 mm) for the non-massaged side and 14.9% with standard deviation 6.1% and range 5.3 to 22.1% (mean 2.7 mm, standard deviation 1.5 mm, range 0.4 to 4.9 mm) for the massaged side. At 4 months, the mean fat layer reduction was 44% greater in the massaged side, Figure 9.
Fig 8.
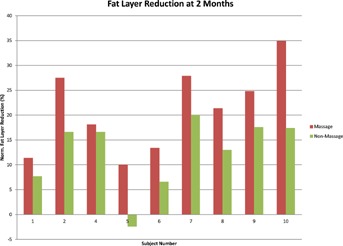
Fat layer reduction for nine subjects at 2 months. Mean fat layer reduction was 68% greater for the massaged compared to the non-massaged side following cryolipolysis.
Fig 9.
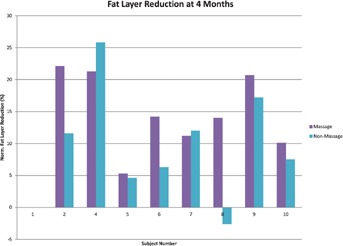
Fat layer reduction for eight subjects at 4 months. Mean fat layer reduction was 44% greater for the massaged compared to the non-massaged side following cryolipolysis.
Safety Results
Treatment sites were evaluated immediately following post-treatment manual massage for any epidermal, dermal, or subcutaneous findings. Non-massage sites were assessed immediately following cryolipolysis. In all cases, typical side effects, such as erythema, bruising, minor pain, and transient loss of sensation, were observed. Aside from one subject that reported slight numbness in the massaged side for 8 weeks, typical side effects resolved spontaneously within 14–30 days and no adverse events were reported.
Safety was evaluated by histological analysis at 0, 3, 8, 14, 30, 60, and 120-day time points post-treatment. As shown in Figure 10, the post-treatment massage tissue showed no evidence of necrosis or fibrosis at any of the time points. The non-massage tissue also did not show abnormality following cryolipolysis treatment at 0, 3, 8, 14, 30, 60, and 120 days post-treatment. The histological timeline shows increasing inflammatory response, peaking at 30 days with dense inflammatory cell infiltrate and reduction in adipocyte size, then decreasing to a similar response at 60 and 120 days, with reduced adipocyte size and decreased infiltrates.
Fig 10.
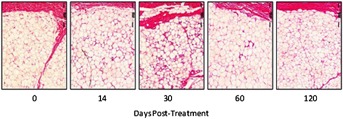
Histology images of abdominal tissue manually massaged post-treatment showed no evidence of necrosis or fibrosis. The massaged and non-massaged tissue looked similar. H&E stain, 40× magnification.
DISCUSSION
Incorporating manual massage immediately following cryolipolysis treatment appears to significantly increase treatment efficacy. While the 2-month follow-up data showed 68% increase in fat layer reduction in the massaged compared to the non-massaged treatment area, the 4-month measurements showed a 44% increase in fat layer reduction. Although it is still an improvement in fat layer reduction, it is unknown why the effect was more pronounced at the 2-month timepoint. A paired t-test found significant effect from post-treatment massage with P = 0.0007 at 2 months, but P = 0.1 at 4 months. It may be indicative that manual massage caused an additional mechanism of damage immediately following treatment, perhaps from tissue reperfusion injury. With additional time, however, the cold-induced apoptosis is likely to cause gradual, ongoing fat cell destruction in both the massaged and non-massaged treatment areas. The mechanism of action by which cryolipolysis induces damage to adipocytes is not well understood and remains an ongoing subject of research. The ultrasound fat layer measurements in this study yielded results that were lower than the typical published results of approximately 20%. This is likely due to the small sample size since there is a significant range in patient response to non-surgical fat reduction procedures, such as cryolipolysis.
The manual massage sensation was reported to be uncomfortable but not painful, and it is likely that the level of discomfort is acceptable to the patient given the resultant increased treatment efficacy. No long-term side effects or adverse events were reported. Therefore, cryolipolysis is shown to be a well-tolerated, efficacious treatment method for decreasing fat layer thickness in the lower abdomen. As cryolipolysis treatment protocols continue to be refined and optimized, post-treatment manual massage is one technique that can be incorporated to safely improve treatment efficacy.
CONCLUSION
This study found that post-treatment manual massage improved cryolipolysis treatment efficacy. At 2 months follow-up, the massaged sites had mean fat layer reduction 68% greater than the non-massaged sites. By 4 months post-treatment, the massaged sites had 44% greater fat layer reduction compared to the non-massaged treatment sites. Histological analysis of massage tissue at 0, 3, 8, 14, 30, 60, and 120 post-treatment found no evidence of fibrosis or necrosis. The massaged and non-massaged tissues looked similar. Thus, post-treatment manual massage is shown to be a safe and effective method to further reduce the fat layer following a cryolipolysis procedure.
Acknowledgments
The authors acknowledge Kevin Springer and Bill Blaker for assistance with ultrasound imaging and clinical photography.
REFERENCES
- 1.Coleman SR, Sachdeva K, Egbert BM, Preciado J, Allison J. Clinical efficacy of noninvasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plast Surg. 2009;33(4):482–488. doi: 10.1007/s00266-008-9286-8. [DOI] [PubMed] [Google Scholar]
- 2.Manstein D, Laubach H, Watanabe K, Farinelli W, Zurakowski D, Anderson RR. Selective cryolysis: A novel method of non-invasive fat removal. Lasers Surg Med. 2008;40(9):595–604. doi: 10.1002/lsm.20719. [DOI] [PubMed] [Google Scholar]
- 3.Zelickson B, Egbert BM, Preciado J, Allison J, Springer K, Rhoades RW, Manstein D. Cryolipolysis for noninvasive fat cell destruction: Initial results from a pig model. Dermatol Surg. 2009;35(10):1462–1470. doi: 10.1111/j.1524-4725.2009.01259.x. [DOI] [PubMed] [Google Scholar]
- 4.Preciado J, Allison J. The effect of cold exposure on adipocytes: Examining a novel method for the noninvasive removal of fat. Cryobiology. 2008;57(3):327. [Google Scholar]
- 5.Nelson AA, Wasserman D, Avram MM. Cryolipolysis for reduction of excess adipose tissue. Semin Cutan Med Surg. 2009;28(4):244–249. doi: 10.1016/j.sder.2009.11.004. [DOI] [PubMed] [Google Scholar]
- 6.Brightman L, Geronemus R. Can second treatment enhance clinical results in cryolipolysis. Cosmetic Derm. 2011;24(2):85–88. [Google Scholar]
- 7.Shek SY, Chan NP, Chan HH. Non-invasive cryolipolysis for body contouring in Chinese—A first commerial experience. Laser Surg Med. 2011;44(2):125–130. doi: 10.1002/lsm.21145. [DOI] [PubMed] [Google Scholar]