

Abstract
The prevalence of kidney stone disease is increasing, and newer research is finding that stones are associated with several serious morbidities. These facts suggest that emphasis needs to be placed not only on stone treatment but also stone prevention. However, there is a relative dearth of information on dietary and medical therapies to treat and avoid nephrolithiasis. In addition, studies have shown that there are many misconceptions among both the general community and physicians about how stones should be managed. This article is meant to serve as a review of the current literature on dietary and drug therapies for stone prevention.
Keywords: Diet therapy, Drug therapy, Kidney calculi, Nephrolithiasis
INTRODUCTION
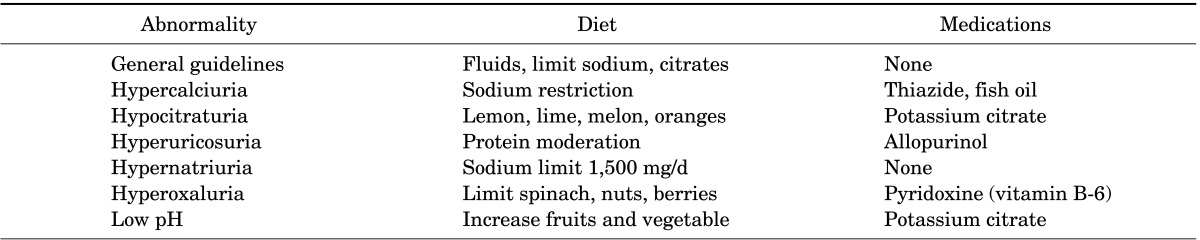
The prevalence of urinary tract stone disease is increasing. According to the U.S. National Health and Nutrition Examination Survey (NHANES), as of 2012, 10.6% of men and 7.1% of women in the United States are affected by kidney stones, a 70% increase from the previous NHANES in 1994 that reported just 6.3% of men and 4.1% of women were affected. Furthermore, the 5-year recurrence rates of stone disease are as high as 30% to 50% [1]. The high rate of recurrence suggests that there are many misconceptions about how to prevent stone formation. Indeed, a recent study demonstrated that only 7% of patients with symptomatic nephrolithiasis and 17% of patients with recurrent episodes underwent a 24-hour urine metabolic evaluation to direct stone prevention measures. The purpose of this article was to explore the existing literature for recommendations on the dietary and medical management of nephrolithiasis, focusing primarily on calcium oxalate and uric acid stones (Table 1).
TABLE 1.
Summary of dietary and medical therapies for kidney stone prevention
DIETARY MANAGEMENT OF CALCIUM OXALATE STONES
1. Hydration
Several studies have shown that increasing fluid intake reduces the risk of stone formation [2,3]. With low fluid intake, urine output is decreased and urine flow is slower, both of which increase the risk of stone formation. Current guidelines recommend drinking enough fluids to produce at least 2.5 L of urine daily [4]. Almost all beverages, including coffee, tea, wine, beer, and fruit juices, are acceptable. The only fluids that should be avoided are tomato, grapefruit, and cranberry juice, because tomato juice is high in sodium whereas grapefruit and cranberry juices are rich in oxalate.
Soda consumption may play a role in stone formation. One study found that among patients who initially drank at least 160 mL/d of soft drinks, those who quit had a higher 3-year freedom from recurrence than did those who continued to drink soda. However, this only held true for patients who drank phosphoric acid-containing sodas, which consist primary of the colas, and not in patients who drank citric acid-containing sodas, which include most clear soft drinks [5].
2. Citric acid
Consuming fruit juice prevents stone formation not only because it increases urine volume but also because it is high in potassium and citric acid. Citrate prevents stone formation by two mechanisms. First, it binds with urinary calcium, thereby reducing the supersaturation of urine. In addition, it binds calcium oxalate crystals and prevents crystal growth [6]. Hypocitraturia is one of the most common metabolic disturbances in patients with calcium stones and affects about 60% of these patients. Patients with low urinary citrate should be encouraged to increase their consumption of foods high in citric acid, such as lemon and lime juice. Consuming just 4 oz of lemon juice per day has been shown to significantly increase urine citrate levels without increasing oxalate levels [7]. Alternatives include melon juice and orange juice, both of which are rich sources of citrate [8].
Urinary citrate excretion is determined by acid-base status. Higher acid loads facilitate renal citrate reabsorption, thereby reducing its excretion [9]. Foods that have a high acid load include meats, fish, poultry, cheese, and eggs. A high animal protein diet not only increases urinary calcium and uric acid concentration, but also decreases citrate levels and urinary pH. However, we do not a recommend a low-protein diet. Instead, we favor an adequate protein diet, consisting of 0.8 to 1 g of protein/kg. Plant protein is less likely to make the urine acidic than is animal protein and so is the preferred protein source.
3. Calcium
There is a common misconception that decreasing calcium intake will reduce the risk of calcium stone formation. In fact, studies have shown that low dietary calcium actually increases the risk of developing symptomatic kidney stones [3,10,11]. With low calcium intake, there is not enough calcium in the digestive tract to bind with oxalate, leading to increased oxalate absorption and urinary oxalate excretion. Dietary sources of calcium include dairy products; calcium-fortified foods such as orange juice, soy milk, tofu, and selected cereals; sardines with bones; and almonds.
Target calcium intake is 1,200 mg, which is the equivalent of four 8-oz glasses of milk. Dietary calcium is preferred to calcium supplementation because supplements may be associated with an increased risk of stone formation [10]. The reason has not been fully elucidated but is thought to be secondary to timing of supplement intake or excessive total calcium [12]. If patients require calcium supplements, calcium citrate should be utilized instead of calcium carbonate.
Patients should combine their calcium intake with a low-salt diet because sodium chloride leads to urinary calcium excretion [13]. For every 2,300 mg, or 1 teaspoon, of salt intake there is a 23-mg increase in urinary calcium [14]. A good rule of thumb is the "5" rule, which dictates that if the word salt or sodium is listed in the first five ingredients of a food label, that food should be avoided. Other salt-rich foods that should be avoided include pizza and canned soups.
4. Oxalate
Higher oxalate intake has been shown to increase urinary oxalate levels [15]. Although the data are conflicting, the general consensus is that higher urinary oxalate levels increase the risk of nephrolithiasis [4,16]. However, we recommend limiting dietary oxalate only if the patient has hyperoxaluria, because many of the oxalate-rich foods are considered "heart-healthy." Together, spinach, potatoes, and nuts account for 44% of oxalate intake for the average American. The simplest way to minimize oxalate intake is to monitor consumption of these foods. In younger women, chocolate is a significant source of dietary oxalate intake and should be consumed sparingly [17].
5. Vitamins
Vitamin C, at the super-dosages found in supplements, increases urine oxalate concentration because ascorbic acid is metabolized to oxalate. Vitamin B-6 (pyridoxine), on the other hand, may reduce urinary oxalate. Pyridoxine is a cofactor for alanine glyoxylate aminotransferase (AGT), which is the enzyme that catalyzes the conversion of glyoxylate to glycine. When there is a deficiency of AGT or low levels of pyridoxine, glyoxylate may be converted to oxalate. Studies have demonstrated an inverse association between vitamin B-6 intake and the risk of stone formation [18] and have provided evidence that combining dietary therapy with pyridoxine supplementation is effective in hyperoxaluric stone-forming patients [19]. The optimal dosage of supplemental vitamin B-6 has not been determined, but foods high in vitamin B-6 include bananas, avocados, soybeans, halibut, mangos, oatmeal, and fortified ready-to-eat cereal. When using supplemental pyridoxine, we recommend starting with 50 mg daily and titrating up to 200 mg or until a therapeutic response in urinary oxalate is observed.
6. Fish oil
The main source of polyunsaturated fats in Western diets is arachidonic acid (AA), an n-6 fatty acid present in vegetable oil and animal fats. n-6 Fatty acids have been implicated in stone formation. AA breakdown results in the formation of prostaglandins including prostaglandin E2 (PGE2). PGE2 causes hypercalciuria because it increases calcium absorption in the gut, decreases reabsorption in the renal tubules, and increases bone resorption [20]. Dietary eicosapentaenoic acid (EPA) is an n-3 fatty acid and the active ingredient of fish oil. EPA undergoes the same metabolic pathway as the n-6 fatty acids. Therefore, increasing EPA decreases n-6 fatty acid metabolites, in particular PGE2. Lower levels of PGE2 not only decrease urinary calcium excretion but also lead to the activation of the nephron Na/K/2Ca transporter, resulting in increased renal calcium reabsorption. Consuming 1,200 mg/d of fish oil has been associated with significant decreases in urinary calcium and oxalate concentrations and increases in urinary citrate concentration [21,22]. Cold-water fish, including salmon, tuna, mackerel, and sardines; walnuts; flax seeds; and canola oil are rich sources of EPA.
MEDICAL MANAGEMENT OF CALCIUM STONES
1. Thiazide diuretics
Thiazide diuretics decrease sodium reabsorption by inhibiting the NaCl cotransporter in the distal convoluted tubule and increase calcium reabsorption by an unknown mechanism [23]. Several randomized controlled trials have investigated whether this hypocalciuric effect of thiazide diuretics reduces stone formation. An Agency for Healthcare Research and Quality (AHRQ) review analyzed 7 randomized controlled trails, which had a mean follow-up of 3 years, and found that taking thiazide diuretics led to a 29% absolute risk reduction in stone recurrence [24]. Therefore, thiazide diuretics are recommended in patients with hypercalciuria or recurrent calcium stones [4]. Hydrochlorothiazide (25 mg twice a day), chlorthalidone (24 mg/d), and indapamide (1.25 to 2.5 mg/d) have all been associated with reduced stone formation. The hypocalciuric effect of thiazide diuretics can be maximized by limiting dietary sodium. Sodium restriction also minimizes potassium losses that result from the use of thiazides. A risk of taking a thiazide diuretic is its effects on vertebral bone density. The incidence of vertebral fractures was found to be significantly increased in a group of patients from Rochester, Minnesota, who were treated with thiazides for an initial episode of symptomatic urolithiasis. Luckily, thiazide diuretics significantly increased the z-score for bone mineral density of L2-L4 vertebrae, the femoral neck, and the radial shaft [25].
2. Potassium citrate
Prospective randomized controlled trials have shown that potassium citrate reduces the risk of stone formation in patients with recurrent calcium stones or with low urinary citrate. Potassium citrate therapy causes a significant increase in urinary citrate, pH, and potassium, leading to significantly less stone formation [26]. The effects on urinary pH and citrate have been shown to start in less than 12 months and to last for more than 3 years [27]. The AHRQ reviewed six randomized controlled trials and found that the composite risk reduction of taking calcium was 41% [24].
3. Allopurinol
Allopurinol prevents the production of uric acid by acting as a competitive inhibitor of xanthine oxidase, the enzyme that converts xanthine into uric acid. A prospective randomized controlled trial found that allopurinol reduced the risk of recurrent calcium oxalate stones in patients with hyperuricosuria and normal urinary calcium. In patients with elevated uric acid blood or urine levels, the absolute risk reduction was 22% according to the AHRQ review [24]. Although the effectiveness of allopurinol treatment in patients without hyperuricosuria has not been established, hyperuricosuria is not a necessary prerequisite for allopurinol therapy.
MANAGEMENT OF URIC ACID STONES
Uric acid stones account for 15% of all kidney stones. Urinary uric acid is derived from endogenous sources, including de novo synthesis and catabolism of nucleic acids, and exogenous sources, which are dependent on the dietary intake of proteins. Animal protein increases urinary calcium and uric acid, decreases urinary citrate and pH, and increases bone resorption [9,28]. Fish are particularly high in purines, secondary to their high protein levels, and should be avoided in patients with uric acid stones [29]. Other high-purine foods include organ meats, glandular tissue, gravies, and meat extracts. Because uric acid stones form in acidic environments, patients should increase their alkaline load by increasing their intake of fruits and vegetables. Plant proteins do not seem to acidify the urine as much as animal proteins and are therefore preferable. However, mushrooms, asparagus, green peas, and spinach should be avoided [4]. Patients with uric acid stones should also avoid high-fructose corn syrup, which has been associated with hyperuricemia and hyperuricosuria [30].
The most common risk factor for uric acid stones is a decreased urinary pH. Therefore, first-line medical therapy for patients with uric acid stones is potassium citrate to increase urinary pH values, with a goal pH of 6 [4]. Allopurinol is an option for patients with high urinary acid levels (>900 mg/d) who have failed dietary treatment. These patients should be started on 100 mg/d and can be titrated up to 300 mg/d if needed. Allopurinol does not help dissolve current stones, but does help prevent the formation of new stones.
MANAGEMENT OF CYSTINE STONES
Cystine stones result from cystinuria, an autosomal recessive disorder that causes a defect in renal tubular reabsorption of dibasic amino acids. This defect, combined with the relative insolubility of cysteine at physiologic urine pH levels, leads to the formation of cystine stones [31]. The single most important intervention in patients with cystine stones is to increase cystine solubility by increasing fluid intake. Adults with stones should have a target urine output of at least 3 L daily and less than 200 mg of cystine/L of urine [32]. Sodium restriction is also crucial because sodium excretion promotes cystine excretion [33,34]. In addition, limiting animal protein intake is usually recommended because meats are high in cysteine and methionine, which is metabolized into cysteine [35].
Since the solubility of cystine in urine increases with increasing pH, the first-line medication for patients with cystinuria is potassium citrate, and the goal is a pH of 7.0 [4,36]. If the urinary cystine concentration is greater than 500 mg/L, treatment with cystine-binding thiol drugs should be initiated [32]. Thiol drugs reduce the disulfide bond that connects the two cysteine molecules of cystine, and forms a cysteine-thiol compound, which is much more soluble than cystine. Three commonly used thiols are D-penicillamine, alpha-mercaptopropionylglycine, and tiopronin. Tiopronin is started at 200 mg twice a day and the dose is increased until there is less than 200 mg of cystine/L of urine. Tiopronin is usually the preferred thiol, because penicillamine has significant side effects, which include fever, arthralgia, leukopenia, and neuropathy. Tiopronin is more effective when urinary pH is greater than 7, so aggressive hydration is still crucial.
MANAGEMENT OF STRUVITE STONES
Struvite stones are caused by an infection of the urinary tract with urease-producing organisms, such as Pseudomonas, Klebsiella, Proteus, Staphylococcus, and Escherichia coli species. There is no role for dietary therapy in the management of struvite stones. Treatment is primarily surgical. If surgical options have been exhausted, patients can be medically managed with acetohydroxamic acid (AHA), 250 mg three times a day. In randomized controlled trials, AHA inhibited the growth of struvite stones [37,38]. However, patients undergoing AHA therapy have to be monitored carefully for the serious side effects of treatment, including phlebitis and hypercoagulable phenomena [39].
CONCLUSIONS
By combining dietary and medical therapy for stone prevention, one can significantly decrease the risk of stone recurrence and improve quality of life. Patient-centered therapy based on 24-hour urine evaluations of stone risk profiles is recommended.
Footnotes
The authors have nothing to disclose.
References
- 1.Scales CD, Jr, Smith AC, Hanley JM, Saigal CS Urologic diseases in America project. Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160–165. doi: 10.1016/j.eururo.2012.03.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. J Urol. 1996;155:839–843. [PubMed] [Google Scholar]
- 3.Curhan GC, Willett WC, Rimm EB, Stampfer MJ. A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. N Engl J Med. 1993;328:833–838. doi: 10.1056/NEJM199303253281203. [DOI] [PubMed] [Google Scholar]
- 4.Pearle MS, Goldfarb DS, Assimos DG, Curhan G, Denu-Ciocca CJ, Matlaga BR, et al. Medical management of kidney stones: AUA guideline. J Urol. 2014;192:316–324. doi: 10.1016/j.juro.2014.05.006. [DOI] [PubMed] [Google Scholar]
- 5.Shuster J, Jenkins A, Logan C, Barnett T, Riehle R, Zackson D, et al. Soft drink consumption and urinary stone recurrence: a randomized prevention trial. J Clin Epidemiol. 1992;45:911–916. doi: 10.1016/0895-4356(92)90074-w. [DOI] [PubMed] [Google Scholar]
- 6.Penniston KL, Nakada SY, Holmes RP, Assimos DG. Quantitative assessment of citric acid in lemon juice, lime juice, and commercially-available fruit juice products. J Endourol. 2008;22:567–570. doi: 10.1089/end.2007.0304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Seltzer MA, Low RK, McDonald M, Shami GS, Stoller ML. Dietary manipulation with lemonade to treat hypocitraturic calcium nephrolithiasis. J Urol. 1996;156:907–909. [PubMed] [Google Scholar]
- 8.Baia Lda C, Baxmann AC, Moreira SR, Holmes RP, Heilberg IP. Noncitrus alkaline fruit: a dietary alternative for the treatment of hypocitraturic stone formers. J Endourol. 2012;26:1221–1226. doi: 10.1089/end.2012.0092. [DOI] [PubMed] [Google Scholar]
- 9.Reddy ST, Wang CY, Sakhaee K, Brinkley L, Pak CY. Effect of low-carbohydrate high-protein diets on acid-base balance, stone-forming propensity, and calcium metabolism. Am J Kidney Dis. 2002;40:265–274. doi: 10.1053/ajkd.2002.34504. [DOI] [PubMed] [Google Scholar]
- 10.Curhan GC, Willett WC, Speizer FE, Spiegelman D, Stampfer MJ. Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in women. Ann Intern Med. 1997;126:497–504. doi: 10.7326/0003-4819-126-7-199704010-00001. [DOI] [PubMed] [Google Scholar]
- 11.Borghi L, Schianchi T, Meschi T, Guerra A, Allegri F, Maggiore U, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. N Engl J Med. 2002;346:77–84. doi: 10.1056/NEJMoa010369. [DOI] [PubMed] [Google Scholar]
- 12.Jackson RD, LaCroix AZ, Gass M, Wallace RB, Robbins J, Lewis CE, et al. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006;354:669–683. doi: 10.1056/NEJMoa055218. [DOI] [PubMed] [Google Scholar]
- 13.Nouvenne A, Meschi T, Prati B, Guerra A, Allegri F, Vezzoli G, et al. Effects of a low-salt diet on idiopathic hypercalciuria in calcium-oxalate stone formers: a 3-mo randomized controlled trial. Am J Clin Nutr. 2010;91:565–570. doi: 10.3945/ajcn.2009.28614. [DOI] [PubMed] [Google Scholar]
- 14.Sakhaee K, Harvey JA, Padalino PK, Whitson P, Pak CY. The potential role of salt abuse on the risk for kidney stone formation. J Urol. 1993;150(2 Pt 1):310–312. doi: 10.1016/s0022-5347(17)35468-x. [DOI] [PubMed] [Google Scholar]
- 15.Holmes RP, Goodman HO, Assimos DG. Contribution of dietary oxalate to urinary oxalate excretion. Kidney Int. 2001;59:270–276. doi: 10.1046/j.1523-1755.2001.00488.x. [DOI] [PubMed] [Google Scholar]
- 16.Curhan GC, Taylor EN. 24-h uric acid excretion and the risk of kidney stones. Kidney Int. 2008;73:489–496. doi: 10.1038/sj.ki.5002708. [DOI] [PubMed] [Google Scholar]
- 17.Taylor EN, Curhan GC. Oxalate intake and the risk for nephrolithiasis. J Am Soc Nephrol. 2007;18:2198–2204. doi: 10.1681/ASN.2007020219. [DOI] [PubMed] [Google Scholar]
- 18.Curhan GC, Willett WC, Speizer FE, Stampfer MJ. Intake of vitamins B6 and C and the risk of kidney stones in women. J Am Soc Nephrol. 1999;10:840–845. doi: 10.1681/ASN.V104840. [DOI] [PubMed] [Google Scholar]
- 19.Ortiz-Alvarado O, Miyaoka R, Kriedberg C, Moeding A, Stessman M, Monga M. Pyridoxine and dietary counseling for the management of idiopathic hyperoxaluria in stone-forming patients. Urology. 2011;77:1054–1058. doi: 10.1016/j.urology.2010.08.002. [DOI] [PubMed] [Google Scholar]
- 20.Taylor EN, Stampfer MJ, Curhan GC. Fatty acid intake and incident nephrolithiasis. Am J Kidney Dis. 2005;45:267–274. doi: 10.1053/j.ajkd.2004.09.026. [DOI] [PubMed] [Google Scholar]
- 21.Ito H, Kotake T, Nomura K. Effect of ethyl icosapentate on urinary calcium excretion in calcium oxalate stone formers. Urol Int. 1995;54:208–213. doi: 10.1159/000282725. [DOI] [PubMed] [Google Scholar]
- 22.Yasui T, Tanaka H, Fujita K, Iguchi M, Kohri K. Effects of eicosapentaenoic acid on urinary calcium excretion in calcium stone formers. Eur Urol. 2001;39:580–585. doi: 10.1159/000052507. [DOI] [PubMed] [Google Scholar]
- 23.Nijenhuis T, Hoenderop JG, Loffing J, van der Kemp AW, van Os CH, Bindels RJ. Thiazide-induced hypocalciuria is accompanied by a decreased expression of Ca2+ transport proteins in kidney. Kidney Int. 2003;64:555–564. doi: 10.1046/j.1523-1755.2003.00128.x. [DOI] [PubMed] [Google Scholar]
- 24.Guirguis-Blake J. Preventing recurrent nephrolithiasis in adults. Am Fam Physician. 2014;89:461–463. [PubMed] [Google Scholar]
- 25.Pak CY, Heller HJ, Pearle MS, Odvina CV, Poindexter JR, Peterson RD. Prevention of stone formation and bone loss in absorptive hypercalciuria by combined dietary and pharmacological interventions. J Urol. 2003;169:465–469. doi: 10.1097/01.ju.0000047341.55340.19. [DOI] [PubMed] [Google Scholar]
- 26.Barcelo P, Wuhl O, Servitge E, Rousaud A, Pak CY. Randomized double-blind study of potassium citrate in idiopathic hypocitraturic calcium nephrolithiasis. J Urol. 1993;150:1761–1764. doi: 10.1016/s0022-5347(17)35888-3. [DOI] [PubMed] [Google Scholar]
- 27.Robinson MR, Leitao VA, Haleblian GE, Scales CD, Jr, Chandrashekar A, Pierre SA, et al. Impact of long-term potassium citrate therapy on urinary profiles and recurrent stone formation. J Urol. 2009;181:1145–1150. doi: 10.1016/j.juro.2008.11.014. [DOI] [PubMed] [Google Scholar]
- 28.Fellstrom B, Danielson BG, Karlstrom B, Lithell H, Ljunghall S, Vessby B, et al. Effects of high intake of dietary animal protein on mineral metabolism and urinary supersaturation of calcium oxalate in renal stone formers. Br J Urol. 1984;56:263–269. doi: 10.1111/j.1464-410x.1984.tb05384.x. [DOI] [PubMed] [Google Scholar]
- 29.Best S, Tracy C, Bagrodia A, Poindexter J, Adams-Huet B, Sakhaee K, et al. Effect of various animal protein sources on urinary stone risk factors [Internet] Linthicum, MD: American Urological Association; c2014. [cited 2014 Nov 24]. Available from: https://www.auanet.org/university/abstract_detail.cfm?id=2147&meetingID=11WAS. [Google Scholar]
- 30.Reiser S, Powell AS, Scholfield DJ, Panda P, Ellwood KC, Canary JJ. Blood lipids, lipoproteins, apoproteins, and uric acid in men fed diets containing fructose or high-amylose cornstarch. Am J Clin Nutr. 1989;49:832–839. doi: 10.1093/ajcn/49.5.832. [DOI] [PubMed] [Google Scholar]
- 31.Sakhaee K, Maalouf NM, Sinnott B. Clinical review. Kidney stones 2012: pathogenesis, diagnosis, and management. J Clin Endocrinol Metab. 2012;97:1847–1860. doi: 10.1210/jc.2011-3492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Barbey F, Joly D, Rieu P, Mejean A, Daudon M, Jungers P. Medical treatment of cystinuria: critical reappraisal of long-term results. J Urol. 2000;163:1419–1423. doi: 10.1016/s0022-5347(05)67633-1. [DOI] [PubMed] [Google Scholar]
- 33.Jaeger P, Portmann L, Saunders A, Rosenberg LE, Thier SO. Anticystinuric effects of glutamine and of dietary sodium restriction. N Engl J Med. 1986;315:1120–1123. doi: 10.1056/NEJM198610303151803. [DOI] [PubMed] [Google Scholar]
- 34.Rodríguez LM, Santos F, Malaga S, Martinez V. Effect of a low sodium diet on urinary elimination of cystine in cystinuric children. Nephron. 1995;71:416–418. doi: 10.1159/000188761. [DOI] [PubMed] [Google Scholar]
- 35.Rodman JS, Blackburn P, Williams JJ, Brown A, Pospischil MA, Peterson CM. The effect of dietary protein on cystine excretion in patients with cystinuria. Clin Nephrol. 1984;22:273–278. [PubMed] [Google Scholar]
- 36.Saravakos P, Kokkinou V, Giannatos E. Cystinuria: current diagnosis and management. Urology. 2014;83:693–699. doi: 10.1016/j.urology.2013.10.013. [DOI] [PubMed] [Google Scholar]
- 37.Williams JJ, Rodman JS, Peterson CM. A randomized double-blind study of acetohydroxamic acid in struvite nephrolithiasis. N Engl J Med. 1984;311:760–764. doi: 10.1056/NEJM198409203111203. [DOI] [PubMed] [Google Scholar]
- 38.Griffith DP, Gleeson MJ, Lee H, Longuet R, Deman E, Earle N. Randomized, double-blind trial of Lithostat (acetohydroxamic acid) in the palliative treatment of infection-induced urinary calculi. Eur Urol. 1991;20:243–247. doi: 10.1159/000471707. [DOI] [PubMed] [Google Scholar]
- 39.Rodman JS, Williams JJ, Jones RL. Hypercoagulability produced by treatment with acetohydroxamic acid. Clin Pharmacol Ther. 1987;42:346–350. doi: 10.1038/clpt.1987.159. [DOI] [PubMed] [Google Scholar]