

About a decade ago, researchers defined the term “population health” to mean the “health outcomes of a group of individuals, including the distribution of such outcomes within the group.”1 Their goal was to broaden the discussion of health policy in the United States beyond the “biomedical paradigm” and to encourage investigation into and policy development of the underlying causes of illness. As originally conceived, the term encompassed the impact of income inequality, educational differences, and unjust disparities. Since then, population health has come to mean many different things to many different people.
Two years ago, I met with a vice president of a local health system who had asked to brief me on his company's “population health strategy.” I was not familiar with the phrase. I kept asking which population he was referring to. He kept giving me a puzzled look in return. Eventually, I figured out that his health system was marketing an insurance product and that its “population health strategy” meant enrolling as many people as possible.
Insurers are now using “population health” to refer to practically any effort to enhance the health status of their members. For example, the trade organization America's Health Insurance Plans (AHIP) offers “population health solutions” to its health plans across the country. These solutions include “health coaching/fitness/wellness, clinical care/care management, accreditation, pharmacy/PBM, pharmaceutical, oncology, hospice, behavioral health, and surgical device management.”2
Surgical device management?
Health care providers also have adopted “population health” as a catchall for efforts to improve health outcomes. For example, the American Hospital Association maintains that population health depends on effective initiatives “to (1) increase the prevalence of evidence-based preventive health services and preventive health behaviors, (2) improve care quality and patient safety, and (3) advance care coordination across the health care continuum.”3
In addition, psychiatric researchers now use “population health” to refer to the prevention of mental disorders4; health IT companies use the term to refer to the analysis of data for a patient group; and many consultants use it for a wide range of services that pop up when searching for “population health” on Google. Checklists, fact sheets, and white papers promise to provide the recipe for population health success. Increasingly, medical schools are now adopting broad population health curricula. One medical school dean recently stated, “Population health will … allow a careful consideration of the special needs of each physician's, and each practice's, patient panel—how to collect and utilize data and institute system changes that benefit all.”5
Recently, I turned to PubMed to assess the use of the term “population health” and found that its appearance in journal titles is on track to double since 2010 (Figure 1). This popularity, however, may be growing in direct proportion to a lack of clarity in meaning.
Figure 1.
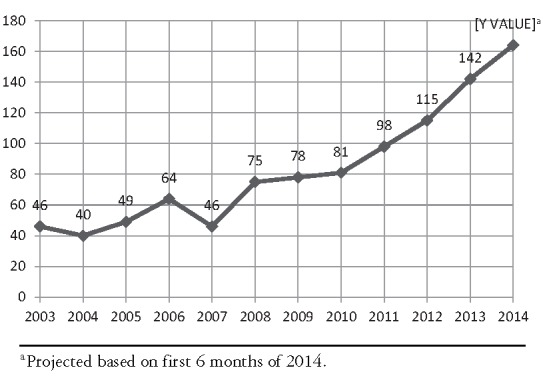
English-Language PubMed Titles With “Population Health”
Under cross-examination, I will admit that when insurers take steps to make their members healthier, it can count as a population health effort—with the “population” defined by those who carry around a particular benefit card. Similarly, when a health care provider undertakes an initiative to improve outcomes among those in its care, it also can qualify as a population health initiative—with “population” meaning those who walk through the clinic or hospital doors.
It obviously is good news that many in the health care system are now using a term to express their interest in improving the health of those they are serving. It is especially promising that medical students are learning about actions that can help improve the health of groups of patients at a time. But something is lost when the term “population health” used predominantly by those whose vision may be limited to the group of people they know, see, and track. Poor health is found—indeed, is more likely to be found—among those without a medical home, those shuffling between periods of no health insurance and periods of temporary coverage, and those facing financial, linguistic, and other barriers to care. Initiatives by insurance carriers and clinicians may miss these groups entirely.
Slowly but surely, “population health” as a term appears to be losing its connection with why it was defined a decade ago. Insurers and health care providers have a number of tools at their disposal that can be better utilized to improve health, but they rarely address the social causes of illness. Instead of serving as a light to illuminate the world outside the boundaries of medical treatment, the term “population health” has become a mirror that reflects back to the leaders of the health care system various ideas for initiatives under their control.
A bold strategy to improve health must go beyond the usual recommended prevention, clinical quality, data integration, and care coordination efforts. It must extend past what a clinic or insurer can do on its own. It must incorporate social and policy initiatives to improve health, and it must define success or failure by not only those served but also those left behind.
There is another term for such a comprehensive approach, and that term is “public health.” Public health agencies can address environmental contributors to asthma, lead successful efforts to reduce tobacco use and other behaviors that undermine health, and partner with zoning, housing, transportation, and other agencies to advance the health of a neighborhood, city, county, or state. Effective leaders in local and state health departments bring a unique set of tools to address poor health, and they can assess trends using a wide range of reliable metrics.
Here's a modest proposal: Medical schools get to keep using the term “population health,” but only if they aim to teach students key public health competencies (as at least 16 in the United States do so far). Insurers and clinicians also can continue using the term “population health,” but with a few conditions. These include collaborating with those agencies responsible for a geographic population; investing in the use of innovative and creative approaches to improve outcomes, including those not under their direct control; and participating in coordinated initiatives to address the underlying causes of illness. Otherwise, we may find ourselves awash in population health efforts, without meaningful progress in the health of our population.
References
- 1.Kindig D, Stoddart G. What is population health? Am J Public Health. 2003;93(3):380–383. doi: 10.2105/ajph.93.3.380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.America's Health Insurance Plans. Population health http://www.ahip.org/Business-Solutions/Population-Health/. Accessed September 1, 2014.
- 3.American Hospital Association. Managing population health: the role of the hospital http://www.hpoe.org/resources/hpoehretaha-guides/805. Published April 2012. Accessed September 1, 2014.
- 4.Jacka FN, Mykletun A, Berk M. Moving towards a population health approach to the primary prevention of common mental disorders. BMC Med. 2012;10:149. doi: 10.1186/1741-7015-10-149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.American Medical Association. AMA med update http://www.ama-assn.org/ams/pub/meded/2014-march/2014-march.shtml. Published March 2014. Accessed September 1, 2014.