

Abstract
Background
Elderly patients with ST-segment elevation myocardial infarction (STEMI) are at high risk for complications and early mortality; still, they are underrepresented in clinical trials and observational studies. We studied the risk profiles at presentation and early mortality in elderly (≥80 years) versus younger (<80 years) STEMI patients.
Design
This was a prospective cohort study.
Methods
The study population comprised 4,092 consecutive STEMI patients admitted to Oslo University Hospital, Ulleval from 2006 to 2010. Baseline characteristics at admission were recorded, as well as in-hospital mortality. Etiologic strategy was used in the analyses.
Results
Patients ≥80 years of age (n=536) were more likely to be women and have prior myocardial infarction, angina, and stroke, but were less likely to be current smokers. The crude in-hospital mortality was 16.2% in patients aged 80 years and older versus 3.5% in those younger than 80 years. The adjusted odds ratio for mortality in patients aged 80 years and older versus those younger than 80 years increased with increasing levels of serum creatinine and total cholesterol. In patients with low levels of serum creatinine and total cholesterol, the odds ratio was 3.01 (95% confidence interval, 1.86–4.93; P=0.0001); increasing to 11.72 (95% confidence interval, 5.26–26.3; P=0.001) in patients with high levels.
Conclusion
High levels of serum cholesterol and creatinine were important risk factors for early mortality in elderly patients. Depending on the levels of cholesterol and creatinine, in-hospital mortality in patients aged 80 years and older varied from a threefold to an almost twelvefold risk compared with younger patients.
Keywords: ST-segment elevation myocardial infarction, mortality, elderly patients, octogenarian, creatinine, total cholesterol
Introduction
Increasing life expectancy makes the elderly the fastest-growing population segment in high-income countries.1 Although an increasing proportion of myocardial infarctions (MIs) occur in the elderly, they are still underrepresented in clinical trials and observational studies.2–5
Older age by itself has been shown to be the core predictor of survival after ST-segment elevation MI (STEMI).6 As a consequence, elderly patients stand a higher risk for mortality and adverse outcomes compared with younger patients. However, variables such as risk profile at presentation also influence survival. The risk profile in elderly STEMI patients and its influence on survival is not truly stated, and neither is an estimate of the adjusted risk for early mortality in relation to their risk factors.
The aim of this study was to describe the risk profile at presentation in STEMI patients aged 80 years and older compared with younger patients. Further, we wanted to study the risk of in-hospital mortality in older versus younger STEMI patients, in relation to their risk factors at admission.
Materials and methods
Patients
The study population was a cohort of all cases of STEMI hospitalized at Oslo University Hospital, Ulleval from January 1, 2006, to December 31, 2010. The cohort comprised 4,092 STEMI cases from a source population of 8,866 cases of acute MI (AMI) (Figure 1).
Figure 1.
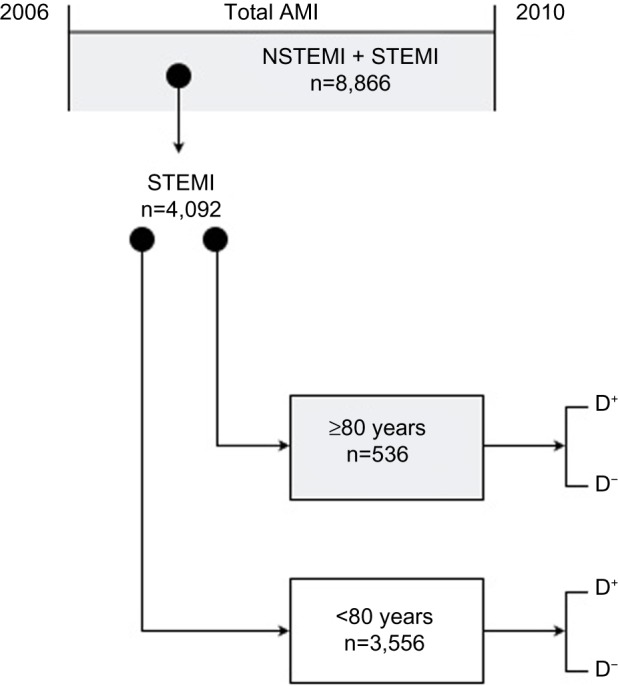
Flow chart of the exposed/nonexposed cohort design.
Abbreviations: AMI, acute myocardial infarction; STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; D, in-hospital mortality yes (+) or no (−).
Oslo University Hospital, Ulleval has 24-hour/7-days-a-week service for primary percutaneous coronary intervention (PCI). It is the primary medical center for a population of 190,000, and it also serves as a secondary cardiac center, performing coronary angiography and PCI for a population of about 1,400,000 in southeastern Norway.
The registration of patient data started at the time of diagnosis. Predefined data on baseline characteristics at admittance, initial electrocardiographic pattern, invasive procedures, and in-hospital mortality were recorded by the responsible physician. Furthermore, the results of routine blood tests taken on admittance were registered. Later, data quality was checked by a specially trained study nurse and the primary study investigator to ensure the validity of the database. The data were entered into a specially designed database developed by the Mid-Norway Regional Health Authority (MRS Norsk Hjerteinfarktregister). To ensure that all patients with AMI were included, a cross-check against the Hospital Discharge Register was performed, and missing patients were included if the diagnosis was regarded as valid.
The diagnosis of AMI was based on current international criteria.7 Troponin T was used as the primary biochemical marker. AMI cases were differentiated as STEMI or non-STEMI (NSTEMI) on the basis of the initial electrocardiographic pattern. Cases were categorized as STEMI when new ST-elevation or a new left bundle branch block were present on the index electrocardiogram and as NSTEMI if the electrocardiogram was normal or showed ST-depression or T-inversion. A few cases were unclassifiable, mainly because of a missing admission electrocardiogram.
The variables considered in this study were defined in the protocol of the register. Hypertension was defined as patients treated for hypertension before the admission, and diabetes mellitus was defined as patients with prediagnosed diabetes mellitus. Smokers were considered those who currently smoked at the date of AMI. Further, hyperlipidemia was defined as patients diagnosed and treated with medical and lifestyle intervention for increased levels of cholesterol or triglycerides. Family history included parents, siblings, or/and children with coronary heart disease (CHD) or other arteriosclerotic vascular disease in early life (males younger than 55 years and women younger than 65 years of age). Peripheral vascular disease was defined as known intermittent claudication or carotid artery stenosis.
The local registry establishment was approved by the Privacy Protection Officer at Oslo University Hospital, Oslo. The Norwegian Regional Ethics Committee classified the study as a quality-of-care project without need for approval from the committee. All data were anonymized before analysis.
Epidemiological design and statistical methods
From the total AMI population, a prospective cohort study was generated (Figure 1). Our strategy was etiologic,8 with a hypothesis consisting of being 80 years old or older (yes/no) as the exposition variable and in-hospital mortality as the primary outcome. All other variables were of interest only as confounders or effect modifiers of the association. A stratification analysis was performed, using the Mantel-Haenszel method, to identify effect modifiers and quantify confounders, followed by controlling for multiconfounders using the logistic regression model in a manual backward elimination procedure.9,10
The association between high age (≥80 years) and in-hospital mortality was quantified using odds ratios (ORs) and their 95% confidence intervals. Differences in categorical variables were compared with Chi-square test, and quantitative variables with skewed distribution with Mann–Whitney test.
A priori power analysis for in-hospital mortality
A beforehand power analysis of the primary hypothesis, the risk for early mortality in patients aged 80 years or older versus younger than 80 years, was performed by the published literature. A challenge of the estimate was a result of the great age variation in previous studies.4,5,11–14 Furthermore, only very few studies have focused on patients aged 80 years and older, all of which were hampered by small patient numbers.2–5
When considering the mean of the relative risks from previous studies,4,5,11–14 we found a mean relative risk of 5.3, indicating a fivefold risk for early mortality for elderly patients compared with younger patients. The mean incidence of in-hospital mortality in younger or nonelderly patients in the same studies was around 2.8%. This low incidence was probably a result of the highly selected group of patients being included in these studies.
Reviewing the results from the literature and considering a ratio (<80 years: ≥80 years) of 7, for a type 1 error of 5% and a power of 80%, we would need 82 patients aged 80 years or older and 574 patients younger than 80 years, for a total of 656 patients.
Results
Clinical profile
From a total number of 4,092 STEMI cases, 3,556 patients (86.9%) were younger than 80 years and 536 patients (13.1%) were aged 80 years or older. Only 72 patients (1.8%) were aged 90 years or older. Table 1 summarizes the differences in baseline risk factors between the two groups. Elderly patients were more likely to be women, have treated hypertension, and have a history of previous stroke, AMI, angina, or peripheral vascular disease, whereas patients younger than 80 years were more likely to be current smokers and have a family history of CHD. Creatinine levels were higher and total cholesterol levels slightly lower in patients aged 80 years or older.
Table 1.
Patient characteristics at admittance
| Characteristics | <80 years (n=3,556) |
≥80 years (n=536) |
P-value* |
|---|---|---|---|
| Male, n (%) | 2,822 (79.4) | 266 (49.6) | <0.001 |
| Current smokers, n (%) | 1,727 (48.6) | 70 (13.1) | <0.001 |
| Treated hypertension, n (%) | 1,154 (32.5) | 263 (49.1) | <0.001 |
| Diabetes mellitus, n (%) | 435 (12.3) | 75 (14.0) | 0.257 |
| Prior hyperlipidemia, n (%) | 420 (11.8) | 40 (7.5) | 0.003 |
| Family history, n (%) | 617 (17.5) | 11 (2.1) | <0.001 |
| Prior myocardial infarction, n (%) | 478 (13.5) | 123 (22.9) | <0.001 |
| Prior percutaneous coronary intervention, n (%) | 387 (10.9) | 46 (8.6) | 0.104 |
| Prior stroke, n (%) | 154 (4.3) | 72 (13.5) | <0.001 |
| Prior peripheral vascular disease, n (%) | 121 (3.4) | 44 (8.2) | <0.001 |
| Prior angina, n (%) laboratory values† | 266 (7.5) | 97 (18.1) | <0.001 |
| Creatinine, μmol/L | 73 (62–105) | 88 (72–110) | <0.001 |
| Total cholesterol, mmol/L | 4.8 (4.1–5.6) | 4.7 (3.8–5.7) | 0.024 |
Notes:
Chi-square test for categorical variables. Mann–Whitney test for continuous variables;
median with 25th and 75th percentile.
Invasive procedures
The rates of coronary angiography and PCI (primary and rescue) were significantly lower in patients aged 80 years or older compared with in patients younger than 80 years (80.6% versus 97.2% and 67.5% versus 86.4%, respectively; P<0.001 for both).
In-hospital mortality
The incidence of in-hospital mortality was 16.2% in patients aged 80 years or older versus 3.5% in patients younger than 80 years (P<0.001). Table 2 summarizes the stratification analysis for in-hospital mortality. The crude OR of in-hospital mortality was 5.41 (95% confidence interval, 4.0–7.3) for patients aged 80 years or older compared with patients younger than 80 years. Current smoker status had a confounding effect of 24%, with an OR for in-hospital mortality in elderly versus younger smokers of 7.82 compared with an OR of 3.84 in elderly nonsmokers. Another confounder was the presence of previous angina, with a confounding effect of 5.04%.
Table 2.
Risk for in-hospital mortality in patients 80 years old and older versus those younger than 80 years, showing variables with significant confounding effect and effect modifiers in the stratification analysis
| Variable level | OR (95% CI) | ORM-H (95% CI) | C% | P-value* |
|---|---|---|---|---|
| Prior angina | ||||
| Yes | 3.06 (1.43–6.53) | 5.16 (3.84–6.95) | 5.4 | 0.1233 |
| No | 5.84 (4.25–8.03) | |||
| Current smoker | ||||
| Yes | 7.82 (3.57–17.09) | 4.10 (3.03–5.55) | 24.2 | 0.0996 |
| No | 3.84 (2.78–5.30) | |||
| Creatinine, μmol/L | ||||
| >84 | 3.04 (2.06–4.47) | † | Effect modifier | 0.0025 |
| <84 | 7.60 (4.86–11.89) | |||
| Cholesterol, mmol/L | ||||
| >4.8 | 10.67 (5.86–19.40) | † | Effect modifier | 0.0054 |
| <4.8 | 4.01 (2.85–5.65) | |||
Notes: Variables included that did not show any confounding effect on in-hospital mortality: sex, diabetes mellitus, treated hypertension; prior hyperlipidemia, family history, prior MI, prior percutaneous coronary intervention, prior stroke, and prior peripheral vascular disease. Crude OR was 5.41 (95% confidence interval, 4.04–7.24); confounder effect % = [[ORM-H – ORc]/ORc] ×100.
Heterogeneity test across strata, Breslow-Day test; P<0.05= effect modifier;
we cannot estimate an adjusted ORM-H in the presence of effect modification.
Abbreviations: C%, confounder effect percentage; CI, confidence interval; MI, myocardial infarction; OR, odds ratio; ORM-H, Mantel-Haenszel adjusted OR.
Two potential effect modifiers were found: creatinine level and total cholesterol level (Table 2). The OR for in-hospital mortality in patients aged 80 years or older compared with younger patients was 7.60 in patients with creatinine levels lower than 84 μmol/L (median cutoff value) and 3.04 in patients with creatinine levels of 84 μmol/L or higher (P=0.0025). Furthermore, the OR for in-hospital mortality in patients aged 80 years or older compared with younger patients was 10.67 in patients with high levels of total cholesterol (median cut-off value, ≥4.8 mmol/L) and 4.01 in patients with low levels of total cholesterol (median cut-off value, <4.8 mmol/L) (P=0.0054).
Adjusted effect on in-hospital mortality
In the logistic regression model (Table 3), smoking was the confounder, and the creatinine and total cholesterol levels were the two effect modifiers. In the adjusted model, the OR of early mortality increased with increasing levels of creatinine, as well as serum cholesterol.
Table 3.
Adjusted risk for in-hospital mortality in patients 80 years old and older versus those younger than 80 years, controlling for the confounding effect of smoking and for the two effect modifiers, serum cholesterol and creatinine
| Creatinine, μmol/L* | Cholesterol, mmol/L† | Odds ratio‡ | 95% confidence interval | P-value |
|---|---|---|---|---|
| 63 | 4.1 | 3.01 | 1.86–4.93 | 0.0001 |
| 110 | 4.1 | 4.15 | 2.69–6.40 | 0.0001 |
| 63 | 6.4 | 8.50 | 3.80–19.20 | 0.0001 |
| 110 | 6.4 | 11.72 | 5.26–26.13 | 0.001 |
Notes: Variables included that did not show any confounding effect on in-hospital mortality: sex, diabetes mellitus, treated hypertension; prior hyperlipidemia, family history, prior myocardial infarction, prior percutaneous coronary intervention, prior stroke, and prior peripheral vascular disease. Crude odds ratio was 5.41 (95% confidence interval, 4.04–7.24).
63 μmol/L and 110 μmol/L =25th and 90th percentiles of creatinine, respectively;
4.1 mmol/L and 6.4 mmol/L =25th and 90th percentiles of cholesterol, respectively;
logistic regression analysis.
With a serum creatinine level of 63 μmol/L (25th percentile) and a serum cholesterol level of 4.1 mmol/L (25th percentile), the OR of in-hospital mortality was 3.01, indicating three times higher risk for in-hospital mortality for patients aged 80 years or older versus patients younger than 80 years. With a creatinine level of 110 μmol/L (90th percentile) and cholesterol level of 4.1 mmol/L, the OR of in-hospital mortality increased to 4.15. Finally, the OR was 11.7 with a creatinine level of 110 μmol/L and a total cholesterol level of 6.4 mmol/L (90th percentile).
Figures 2 and 3 show the variation in the adjusted risk for in-hospital mortality for patients aged 80 years or older versus patients younger than 80 years for different levels of creatinine (Figure 2) and cholesterol (Figure 3). The adjusted risk for in-hospital mortality in patients aged 80 years or older versus those younger than 80 years increased moderately with increasing levels of creatinine, but more markedly with increasing levels of total cholesterol.
Figure 2.
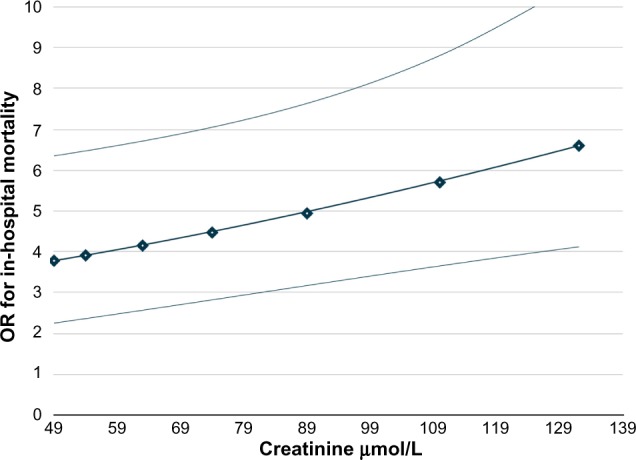
Adjusted odds ratio (OR) of in-hospital mortality for patients 80 years old and older vs those younger than 80 years in relation to creatinine levels, controlling for smoking habits and for the median level of serum cholesterol (4.8 mmol/L).
Notes: OR curve with 95% confidence interval lower and upper bound. Points represent, from left to right, 5th, 10th, 25th, 50th, 75th, 90th, and 95th percentiles.
Figure 3.
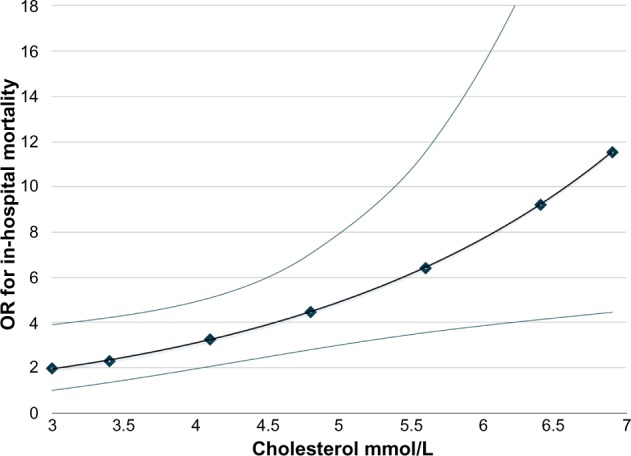
Adjusted odds ratio (OR) of in-hospital mortality for patients 80 years old and older vs those younger than 80 years in relation to total cholesterol levels, controlling for smoking habits and for the median level of serum creatinine (84 μmol/L).
Notes: OR curve with 95% confidence interval lower and upper bound. Points represent, from left to right, 5th, 10th, 25th, 50th, 75th, 90th, and 95th percentiles.
Discussion
The main findings of this study are that the risk profile of STEMI patients aged 80 years or older differs significantly from that of patients younger than 80 years. Second, the risk for early mortality in patients aged 80 years or older compared with younger patients was associated with the levels of serum creatinine and cholesterol; the risk for early mortality increased moderately with increasing levels of creatinine and drastically with increasing levels of cholesterol.
Clinical profiles
Compared with younger patients, elderly patients had more comorbidities. Variables that predominated in the elderly were being female, prior AMI, hypertension, stroke, peripheral vascular disease, and angina. Conversely, there was a reduced rate of smoking, prior family history of CHD, and hyperlipidemia. Elderly patients also had a higher level of serum creatinine and a lower level of serum cholesterol at admittance.
The prevalence of risk factors in our study cohort seems to agree with the prevalence of risk factors in previous studies. However, the BLITZ-3 Registry5 from Italy showed less diabetes mellitus in the elderly, whereas studies2,12 from the Netherlands and the United States indicated an increased rate of diabetes mellitus in the elderly. Similar to us, Hafiz et al4 did not find any differences in the incidence of diabetes between the age groups.
The prevalence of prior AMI and hypertension was significantly higher in the elderly in all reviewed studies, with the exception of the BLITZ-3 Registry,5 in which no significant differences were found.
International geographic variability in baseline characteristics of elderly AMI patients does exist. A recently published comparison between the United States and Sweden concerning treatment and long-term outcomes for AMI in the elderly found that male patients in the United States had a higher risk for prior hypertension, diabetes, and heart failure compared with Swedish men, whereas American female patients had a higher risk for prior hypertension and heart failure.15
In-hospital mortality
The crude OR of in-hospital mortality (OR, 5.41; 95% confidence interval, 4.0–7.3) in patients aged 80 years or older versus younger patients was similar to the fivefold risk for early mortality shown in previous studies.4,5,11–14 However, most previous studies have included very select patient populations. In our study, all consecutive STEMI cases admitted to our hospital during a 5-year period were included, and our estimates are probably a better reflection of the mortality rates in a real-life population than most previous studies on selected patient populations. In spite of this broad inclusion of patients, the rate of in-hospital mortality in the elderly was relatively low (16.2%). This might be because of the high rate of invasive treatment offered to the elderly patients admitted to our hospital (81% of STEMI patients aged 80 years or older underwent coronary angiography).
The are several reasons for the increased in-hospital mortality rate in octogenarians with STEMI: atypical presentation and high incidence of comorbidities such as diabetes, peripheral vascular disease, stroke, congestive heart failure (CHF), prior AMI, and renal insufficiency make elderly patients more vulnerable to complications.3,11 Furthermore, as a result of advancing age, the elderly have a prolonged exposition of risk factors and a more distinct development of multivessel disease, and the aging process and its pathophysiologic alterations on coronary arteries contribute to higher mortality and lower invasive success.3,16
High levels of serum cholesterol and creatinine are risk factors for early mortality after AMI
We found that the adjusted in-hospital mortality rate in patients aged 80 years or older versus those younger than 80 years depended on the level of serum cholesterol and creatinine at admittance; varying from a threefold to an almost twelvefold risk for early mortality.
Our results suggest there is also a relationship between high cholesterol levels and mortality in the elderly.
Although the predictive value of cholesterol levels in older individuals has been shown to be less robust than in younger individuals,17 high cholesterol is an established risk factor for CHD in middle-aged and young elderly patients, and lifetime risk for CHD increases sharply with higher total cholesterol levels at all ages, even in octogenarians.18–20 However, some observational studies have linked low total cholesterol levels in elderly patients with an increased risk for CHD and higher all-cause mortality.18,21 Declining cholesterol levels resulting from comorbid illnesses may partly explain this association.17,18 To our knowledge, this is the first study showing an increased risk for in-hospital mortality in elderly STEMI patients with high levels of cholesterol at admittance.
Renal dysfunction or chronic renal insufficiency has been associated with worse outcomes and increased short-term mortality in octogenarians after AMI.16,22,23 These previous findings seem to agree with the findings in our study: increased level of creatinine, as an indicator of renal dysfunction, was a risk factor of early mortality.
Limitations
As this study focused only on the risk profile at presentation, in-hospital complications and treatment were not evaluated. Previous heart failure was unfortunately not registered at baseline but is prevalent in the elderly and is a strong predictor of mortality.
Because of the anonymization of patient data, we were not able to separate first admissions from second or third admissions. All hospital admissions for STEMI in the selected period were therefore included in this analysis. However, we know from the Myocardial Infarction Registry in our hospital that the rate of new admissions resulting from reinfarction was very low in STEMI patients during the period from 2006 to 2011 (reinfarction rate, 6.4%/6 years in patients <80 years and 5.2%/6 years in patients ≥80 years). This very low rate of reinfarction reduces the risk for bias in our study.
It is likely that the management of AMI patients has improved during the 5 years of observation. However, we did not make any adjustments to these possible trend variations. As we are in an observational study situation, there are always possibilities of unmeasured and hidden confounders.
Conclusion
High levels of serum cholesterol and creatinine were important risk factors for early mortality in elderly patients with STEMI. Depending on the levels of total cholesterol and creatinine at admittance, in-hospital mortality in patients aged 80 years or older varied from a threefold to an almost twelvefold risk compared with younger patients.
Acknowledgments
We thank study personnel Charlotte Holst Hansen and Monica Ziener, as well as the cardiologists at the Department of Cardiology, Ulleval, Oslo University Hospital, for the acquisition of data. We also want to thank the personnel at the Section of Invasive Cardiology, Oslo University Hospital, for performing coronary angiography and PCI in all of these patients.
Footnotes
Author contributions
All authors have made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; have been involved in drafting the manuscript or revising it critically for important intellectual content; and have given final approval of the version to be published.
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: the challenges ahead. Lancet. 2009;374(9696):1196–1208. doi: 10.1016/S0140-6736(09)61460-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Claessen BEPM, Kikkert WJ, Engstrom AE, et al. Primary percutaneous coronary intervention for ST elevation myocardial infarction in octogenarians: trends and outcomes. Heart. 2010;96(11):843–847. doi: 10.1136/hrt.2009.185678. [DOI] [PubMed] [Google Scholar]
- 3.Klein LW. Percutaneous coronary intervention in the elderly patient (Part I of II) J Invasive Cardiol. 2006;18(6):286–295. [PubMed] [Google Scholar]
- 4.Hafiz AM, Jan MF, Mori N, Gupta A, Bajwa T, Allaqaband S. Contemporary clinical outcomes of primary percutaneous coronary intervention in elderly versus younger patients presenting with acute ST-segment elevation myocardial infarction. J Interv Cardiol. 2011;24(4):357–365. doi: 10.1111/j.1540-8183.2011.00634.x. [DOI] [PubMed] [Google Scholar]
- 5.Casella G, Scorcu G, Cassin M, et al. Blitz-3 Investigators Elderly patients with acute coronary syndromes admitted to Italian intensive cardiac care units: a Blitz-3 Registry sub-analysis. J Cardiovasc Med (Hagerstown) 2012;13(3):165–174. doi: 10.2459/JCM.0b013e3283515be3. [DOI] [PubMed] [Google Scholar]
- 6.Gharacholou SM, Lopes RD, Alexander KP, et al. Age and outcomes in ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: findings from the APEX-AMI trial. Arch Intern Med. 2011;171(6):559–567. doi: 10.1001/archinternmed.2011.36. [DOI] [PubMed] [Google Scholar]
- 7.Thygesen K, Alpert JS, White HD, Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50(22):2173–2195. doi: 10.1016/j.jacc.2007.09.011. [DOI] [PubMed] [Google Scholar]
- 8.Hennekens CH, Buring JE, Mayrent SL. Epidemiology in Medicine. Boston. Boston: Little, Brown; 1987. [Google Scholar]
- 9.Kleinbaum DG, Klein M. Logistic Regression: a Self-Learning Text. 3rd ed. New York, NY: Springer-Verlag; 2010. [Google Scholar]
- 10.Kleinbaum DG, Kupper LL. H M. Epidemiologic Research: Principles and Quantitative Methods. New York, NY: Van Nostrand Reinhold; 1982. [Google Scholar]
- 11.Bauer T, Möllmann H, Weidinger F, et al. Predictors of hospital mortality in the elderly undergoing percutaneous coronary intervention for acute coronary syndromes and stable angina. Int J Cardiol. 2011;151(2):164–169. doi: 10.1016/j.ijcard.2010.05.006. [DOI] [PubMed] [Google Scholar]
- 12.Forman DE, Chen AY, Wiviott SD, Wang TY, Magid DJ, Alexander KP. Comparison of outcomes in patients aged <75, 75 to 84, and ≥85 years with ST-elevation myocardial infarction (from the ACTION Registry-GWTG) Am J Cardiol. 2010;106(10):1382–1388. doi: 10.1016/j.amjcard.2010.07.008. [DOI] [PubMed] [Google Scholar]
- 13.Oqueli E, Dick R, In-hospital Mortality and Clinical Outcome Percutaneous coronary intervention in very elderly patients. In-hospital mortality and clinical outcome. Heart Lung Circ. 2011;20(10):622–628. doi: 10.1016/j.hlc.2010.08.012. [DOI] [PubMed] [Google Scholar]
- 14.Sakai K, Nagayama S, Ihara K, et al. Primary percutaneous coronary intervention for acute myocardial infarction in the elderly aged ≥75 years. Catheter Cardiovasc Interv. 2012;79(1):50–56. doi: 10.1002/ccd.22810. [DOI] [PubMed] [Google Scholar]
- 15.Smith LG, Herlitz J, Karlsson T, Berger AK, Luepker RV. International comparison of treatment and long-term outcomes for acute myocardial infarction in the elderly: Minneapolis/St Paul, MN, USA and Goteborg, Sweden. Eur Heart J. 2013;34(41):3191–3197. doi: 10.1093/eurheartj/eht196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Batchelor WB, Anstrom KJ, Muhlbaier LH, et al. National Cardiovascular Network Collaboration Contemporary outcome trends in the elderly undergoing percutaneous coronary interventions: results in 7,472 octogenarians. J Am Coll Cardiol. 2000;36(3):723–730. doi: 10.1016/s0735-1097(00)00777-4. [DOI] [PubMed] [Google Scholar]
- 17.Roberts CGP, Guallar E, Rodriguez A. Efficacy and safety of statin monotherapy in older adults: a meta-analysis. J Gerontol A Biol Sci Med Sci. 2007;62(8):879–887. doi: 10.1093/gerona/62.8.879. [DOI] [PubMed] [Google Scholar]
- 18.Petersen LK, Christensen K, Kragstrup J. Lipid-lowering treatment to the end? A review of observational studies and RCTs on cholesterol and mortality in 80+-year olds. Age Ageing. 2010;39(6):674–680. doi: 10.1093/ageing/afq129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lloyd-Jones DM, Wilson PWF, Larson MG, et al. Lifetime risk of coronary heart disease by cholesterol levels at selected ages. Arch Intern Med. 2003;163(16):1966–1972. doi: 10.1001/archinte.163.16.1966. [DOI] [PubMed] [Google Scholar]
- 20.Thompson PL. Clinical relevance of statins: instituting treatment early in acute coronary syndrome patients. Atheroscler Suppl. 2001;2(1):15–19. doi: 10.1016/s1567-5688(00)00005-2. [DOI] [PubMed] [Google Scholar]
- 21.Strandberg TE, Pitkala KH, Tilvis RS. Statin treatment is associated with clearly reduced mortality risk of cardiovascular patients aged 75 years and older. J Gerontol A Biol Sci Med Sci. 2008;63(2):213–214. doi: 10.1093/gerona/63.2.213. [DOI] [PubMed] [Google Scholar]
- 22.Eckart RE, Shry EA, Simpson DE, Stajduhar KC. Percutaneous coronary intervention in the elderly: procedural success and 1-year outcomes. Am J Geriatr Cardiol. 2003;12(6):366–368. doi: 10.1111/j.1076-7460.2003.02505.x. [DOI] [PubMed] [Google Scholar]
- 23.Fox CS, Muntner P, Chen AY, et al. Acute Coronary Treatment and Intervention Outcomes Network registry Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease: a report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation. 2010;121(3):357–365. doi: 10.1161/CIRCULATIONAHA.109.865352. [DOI] [PMC free article] [PubMed] [Google Scholar]