

Abstract
The eponym Monteggia fracture-dislocation originally referred to a fracture of the shaft of the ulna accompanied by anterior dislocation of the radial head that was described by Giovanni Battista Monteggia of Italy in 1814. Subsequently, a further classification system based on the direction of the radial head dislocation and associated fractures of the radius and ulna was proposed by Jose Luis Bado of Uruguay in 1958. This article investigates the evolution of treatment, classification, and outcomes of the Monteggia injury and sheds light on the lives and contributions of Monteggia and Bado.
Keywords: Forearm fracture-dislocation, Giovanni Battista Monteggia, Jose Luis Bado, Monteggia fracture, Ulnar fracture
A fracture of the shaft of the ulna associated with an anterior dislocation of the radial head was described by an Italian surgeon, Giovanni Battista Monteggia, in 1814. (1) This injury pattern was eponymously named as the Monteggia fracture-dislocation by Perrin in 1909. (2) In 1958, Jose Luis Bado, a professor of orthopedic surgery from Uruguay, elaborated on the pathomechanics and management of this fracture-dislocation in a monograph that was first published in Spanish then later in English. (3-5) He introduced the concept of a Monteggia lesion and Monteggia equivalent injuries. Bado included a group of injuries having in common a dislocation of the radial head associated with fractures at various levels of the ulna or with injuries at the wrist.
Although the eponym Monteggia fracture-dislocation is well recognized by orthopedic surgeons, little is known about the lives and contributions of Monteggia and Bado and the evolution of treatment of this complex injury. A literature search was conducted that included the archives of the libraries of our home institution, University of the Republic, Montevideo, Uruguay, the University of Milan and the University of Pavia in Italy. Additionally, we collected information from online databases such as the History of Medicine and translated original articles from Italian and Spanish. Finally, we contacted family friends and colleagues of Professor Bado. From these original materials, we present the evolution of treatment of Monteggia fracture-dislocations over 2 centuries and summarize the lives and contributions of Monteggia and Bado.
Evolution of Management
The earliest description of this injury was in Monteggia’s book ‘Istituzioni Chirurgiche’ published in 1814. He wrote “…. At the end of the treatment the arm swelling has resolved, but only the dislocation of the radius that was not easy to reduce…. I applied compression and a new bandage again to contain it, but it did not want to stay in place” (Fig. 1). Monteggia appreciated that the ulna fracture was linked to the radial head dislocation and that both needed to be addressed simultaneously. However, his management of the injury by closed reduction and splintage was suboptimal and resulted in recurrence of the radial head subluxation.
Figure 1.
Cover page of Givoanni Monteggia textbook Istituzioni Chirurgiche second edition published in 1814 including the original description of the Monteggia fracture.
The evolution of management of Monteggia fracture-dislocations can be considered in 3 chronological periods. In the early period (1814–1939), the components of the Monteggia injury were identified, and the importance of reducing the radial head and ulna shaft fracture became apparent. In the intermediate period (1940–1990), the availability of implants made open reduction and internal fixation of the ulna shaft possible. There was also an increased awareness of the mechanism of the injury and variations of the original injury, namely the Monteggia lesion and its equivalents. In the current period (1991 and onwards), better results have been obtained as a result of prompt recognition of the injury and improved plate fixation techniques that have allowed anatomic reduction of the ulna and restoration of normal contour of the trochlear notch.
Early period (1814-1939)
In 1844 Cooper, from London, England, described anterior, posterior, and lateral dislocations of the radial head with fracture of the ulna shaft. (6) Shortly after, the fracture pattern received the attention of other authors such as Malgaigne in France (1854), Doerfler in Germany (1886) and Stimson in the United States (1900). (7-9) Malgaigne reported that a fracture of the shaft of the ulna with dislocation of the head of the radius was not uncommon and warned that with any fracture of the ulna, a dislocation of the radius should be considered and vice versa. Doerfler reported 4 cases including a patient who experienced paralysis of the extensor muscles of the forearm owing to injury of the posterior interosseous nerve that was caused by the dislocated head of the radius. Stimson gave a brief account of his personal experience with Monteggia fracture-dislocation in his book ‘Practical Treatise on Fractures and Dislocations’. His series included 10 patients, and he referred to a case that appeared to be one of the earliest descriptions of a known chronic injury. He treated it by an open reduction technique instead of fracture manipulation and closed reduction that was traditionally used to treat forearm fractures at that time. Perrin in France coined the term Monteggia fracture-dislocation in 1909 in his publication Thesis de Paris. (2)
Wilson (1933) in New York and Cunningham (1934) in Oklahoma both presented large numbers of consecutive patients with elbow injuries and formally discussed the management of Monteggia fracture-dislocations. (10-11) Wilson reported 3 cases of Monteggia fracture-dislocation among 439 patients while Cunningham reported 14 cases in a series of 257 patients after excluding fractures of the olecranon and styloid process. Cunningham advocated an immediate reduction of the radial head with simultaneous closed reduction of the ulna fracture. An open reduction of the ulna fracture and radial head with reconstruction of the annular ligament was reserved for chronic cases. In one case, Cunningham used a bone graft to achieve a bony union in a patient who appeared to have malunion of the ulna fracture resulting from a delayed presentation (Fig. 2). Shortly after, Naylor from Bradford, England, reported 9 cases of Monteggia fracture-dislocation that he treated between 1938-1940. (12) He too recommended closed manipulation of dislocated head of radius and reduction of the ulna and dismissed attempts of early open reduction of uncomplicated cases. Five of the 9 Naylor’s patients had complete recovery, 3 patients had limited elbow extension ranging from 130-160 degrees, and 1 patient was unaccounted for.
Figure 2.
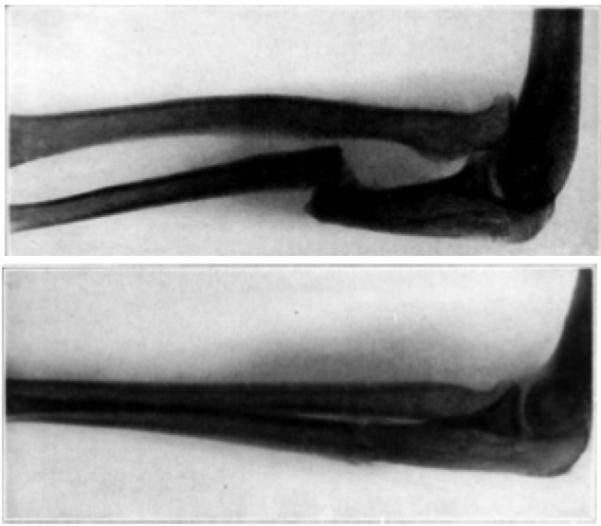
Showing an X-ray of a 32-year-old patient who had a malunion of ulna fracture that was treated with an open reduction and an osteoperiosteal graft.
Intermediate Period (1940-1990)
During this period, a number of publications discussing Monteggia fracture-dislocations appeared in the literature, which reflected an increasing awareness and experience with this injury. The benefits of rigid fixation to promote bone healing became more apparent. (13) Furthermore, improvements in anesthesia and introduction of antibiotics led to a dramatic shift in treatment from closed manipulation and reduction of the radial head and ulna fracture to open reduction and internal fixation. This paradigm shift was initiated by the publication of Speed and Boyd’s article ‘Treatment of fractures of ulna with dislocation of head of radius’ in 1940. (14) The authors presented different patterns of Monteggia injuries in 62 cases that involved acute and chronic fractures of adults and children. They suggested that a closed reduction of Monteggia fracture-dislocation often resulted in poor outcomes and made several recommendations. For adults with acute injury, they advocated the use of an open reduction and fixation of the ulna fracture using vitallium plates and reduction of dislocated radial head through a single lateral incision (Fig. 3). They also advocated reconstruction of the annular ligament using a fascial sling wrapped around the head of the radius to prevent recurrence of dislocation. They discussed pediatric injuries separately from those of adults. They stated that closed reduction of the fracture usually resulted in satisfactory outcomes; however, they performed an open reduction and plate fixation, in similar fashion to the treatment of adults, if the radial head proved difficult to reduce. For cases of nonunion/malunion, they recommended using an onlay bone graft secured by vitallium screws to restore the length of the ulna. Resection of the head and neck of the radius was reserved for a severely fractured radial head to avoid complications such as degenerative arthritis of the radiohumeral joint or recurrence of dislocation. In 1950, Thompson and Hamilton from North Carolina introduced an alternative method of internal fixation of ulna fractures using intramedullary Steinman pins. (15) The authors successfully treated 3 patients with Monteggia fracture using this technique (Fig. 4). They argued that intramedullary nailing was quick, easy, less invasive, provided stronger stabilization, and associated with fewer complications than plate fixation. Furthermore they suggested that this technique allowed faster rehabilitation and recovery of the forearm and elbow joint. However their study involved a limited number of patients, and their technique did not apparently become as popular as plate and screw fixation.
Figure 3.
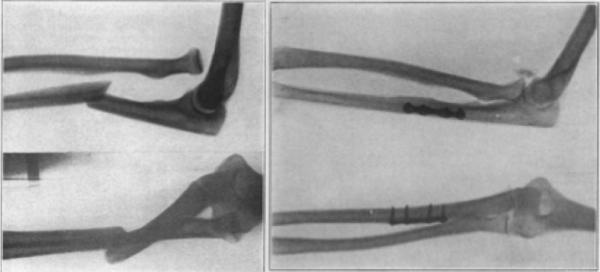
X-rays showing a Monteggia fracture of a young man (left) and his 1 year-postoperative radiograph following open reduction and fixation of the ulna shaft fracture by a vitallium plate and a fascial sling to maintain the reduction of the head of the radius.
Figure 4.
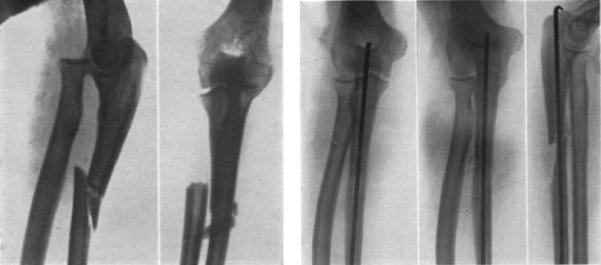
Demonstrating another method of fixation of Monteggia fracture using intramedullary pins as described by Thomas and Hamilton.
Despite the advancements achieved in fracture fixation techniques during that period, the exact mechanism of injury, fracture configuration, and biomechanics of Monteggia fracture-dislocations were still not fully determined. In 1949, Evans from Birmingham, England, carried out experimental work on cadaveric specimens that elaborated on the mechanism of injury. (16) Evans showed that when a patient falls forward onto an outstretched hand, the hand becomes fixed to the ground, whereas the forearm and the rest of the body rotate around its longitudinal axis. As the upper body and the arm continue to rotate outward (supinate), the forearm rotates inwards (pronate). In the forearm, the radius is relatively mobile and rotates around the ulna that is fixed proximally by its articulation with the humerus and distally by the triangular fibrocartilage. The ulna resists rotation and fractures as a result of combination of rotation force and longitudinal compression. The fractured ulna fragment acts as a fulcrum that either pushes the radial head outward of the proximal radioulnar joint or the radius is fractured in its proximal third. Tompkins in Wisconsin later challenged the mechanism of injury described by Evans and suggested that a soft-tissue component might be responsible for the pattern of injury observed. He stated that as a person falls on the outstretched hand, a strong contraction of the biceps muscle causes anterior dislocation of the radial head. The fracture of the ulna is caused by the pull of the intact interosseous membrane and the pull of the brachialis muscle. (17-18) Both Evans and Tompkins explained the mechanism of only 1 variant of Monteggia fracture-dislocation (fracture of the ulna shaft with anterior dislocation of the head of radius). They did not explain the mechanism involved with other patterns of Monteggia fracture-dislocations such as fracture of the ulna shaft with posterior or posterolateral dislocation of the radial head. The latter is less common and was not described by Monteggia.
In another cadaveric experiment, Penrose (1951) from Coventry, England, evaluated the mechanism of Monteggia fracture-dislocations associated with posterior displacement of the head of the radius. (19) He demonstrated that the ligamentous attachments of the elbow are stronger than the shaft of the ulna. A direct blow to the ulna produces a predictable pattern of injury that consists of a proximal ulna fracture with anterior triangular or quadrangular segment at or near the level of coronoid process together with a posterior or posterolateral dislocation of the radiocapitellar head (Fig. 5). The ligamentous support of the radial head, namely annular ligament, has also received a considerable attention in the literature. Smith (1947) from New York illustrated the fate of the annular ligament associated with Monteggia injuries. (20) He described 3 types of annular ligament pathology. First, the ligament may be torn across and remain open; or it may become torn and fold behind the radial head, thus preventing its reduction and permitting further dislocation. Third, instead of the radial head tearing through the ligament, it may be pulled out from beneath it and come to lie anterior to an intact ligament.
Figure 5.

Typical fracture pattern of posterior variant of Monteggia lesion as described by Penrose.
Bado was able to compile the available evidence into a more precise classification that has formed the basis of the modern management of this complex injury. (3-5) In his seminal article published in 1967, Bado classified Monteggia injuries under the term Monteggia lesion, which included types I-IV according to the level and angulation of ulna shaft fracture and the direction of dislocation of the radial head (Table 1). In addition to these 4 types, Bado described a Monteggia equivalent injury that differed in radiological appearance but possessed similar characteristics especially in the mechanism of injury and in its treatment. Bado reported the treatment outcomes of 22 adults and 18 children, the majority of whom experienced from acute injuries. In all except Monteggia type IV injuries, Bado advocated a nonoperative approach except for resistant cases and reported satisfactory results. This contrasted with Speed and Boyd, (14) who were in favor of open reduction and internal fixation for acute injuries except for children in whom nonoperative treatment was employed. In 1969, Boyd and Boals (21) reported the outcomes of another 97 patients. This was in addition to their previous publication in 1940 (Speed and Boyd) and raised their total experience with the treatment of Monteggia fracture-dislocations to 159 cases. Over almost 3 decades their management approach did not change substantially, although their preferred fixation technique involved the use of compression plates that were introduced in the late 1950s. In 1974, Bruce et al. from Los Angeles reported 35 cases of Monteggia fracture-dislocations that were treated with a variety of methods including closed reduction, compression plates, intramedullary rods, and finally a combination for type IV Monteggia fracture-dislocation. (22) Acceptable results were achieved in 64% of children, most of whom were treated nonoperatively. In adults, 24% were deemed to have acceptable results; all were treated operatively, indicating that nonoperative treatment in the adult usually yielded an unsatisfactory result compared to that achieved in children. The authors also concluded that no form of internal fixation in adults was found to be superior to the other. Several other reports showed conflicting evidence regarding the best method of treatment and long-term outcomes. (23-26)
Table 1.
Bado Classification of Monteggia lesions including equivalent lesions
| Bado classification | Direction of radial head dislocation |
Ulnar fracture |
Radial fracture |
Incidence | Equivalents |
|---|---|---|---|---|---|
|
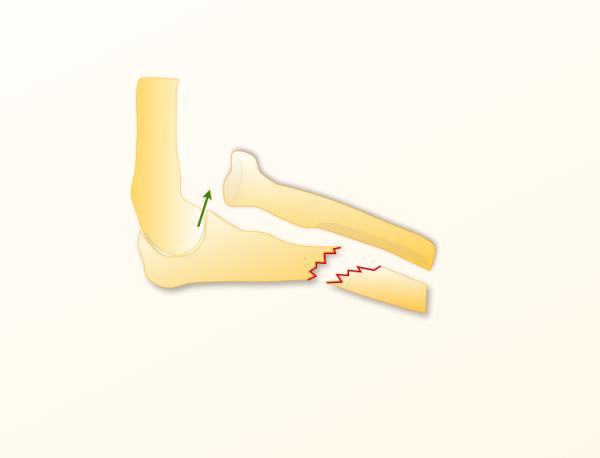
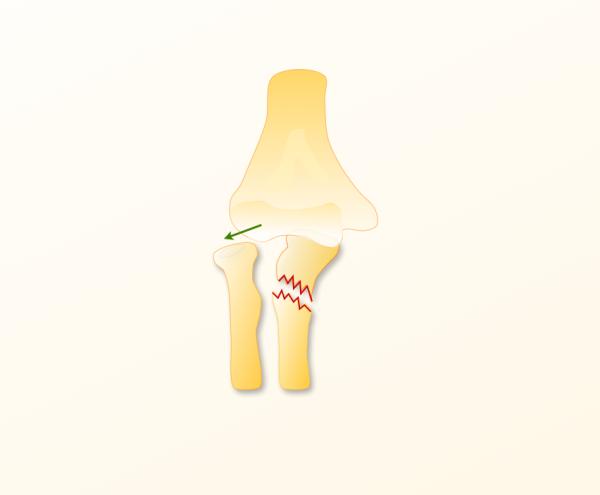
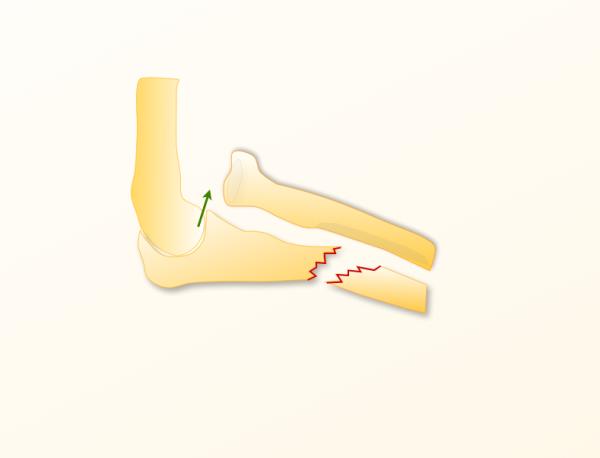
I
(Figure 6A) |
Anterior | Diaphyseal, anterior angulation |
– | 60-70% |
|
|
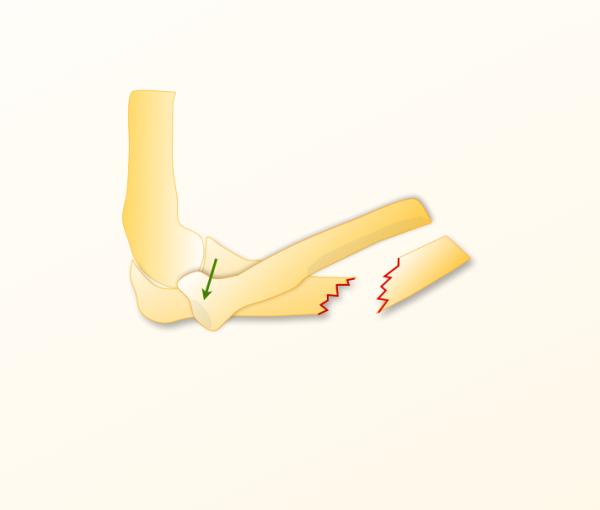
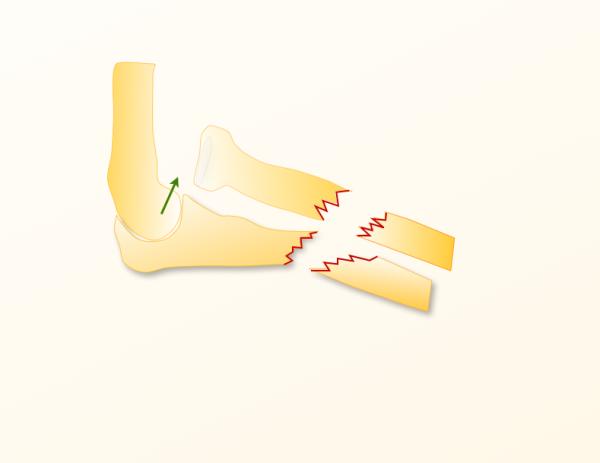
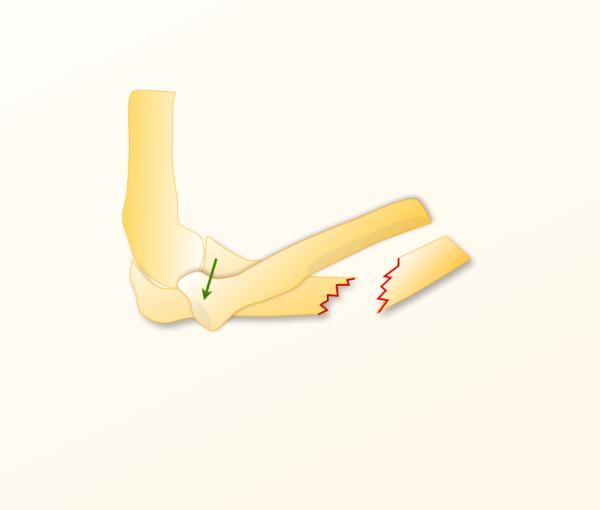
II
(Figure 6B) |
Posterior or posterolateral |
Diaphyseal, Posterior angulation |
– | 15% |
|
|
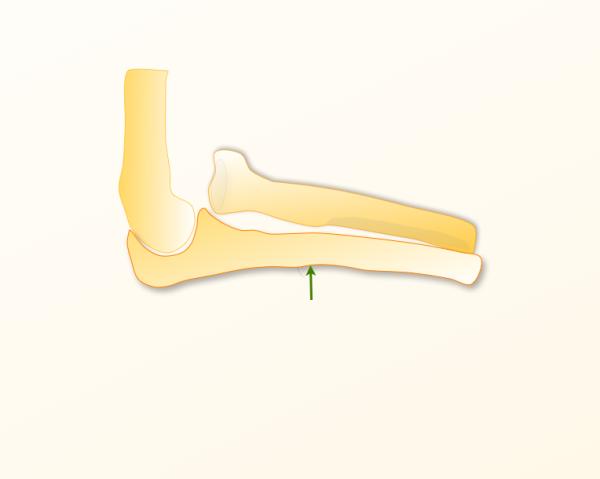
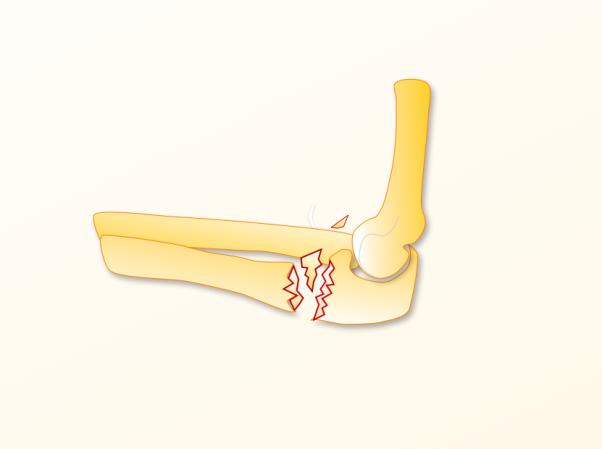
III
(Figure 6C) |
Lateral or Anterolateral |
Metaphysis | – | 20% | – |
|
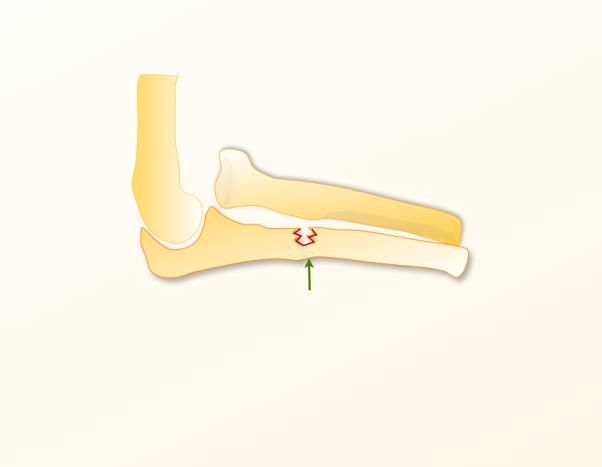
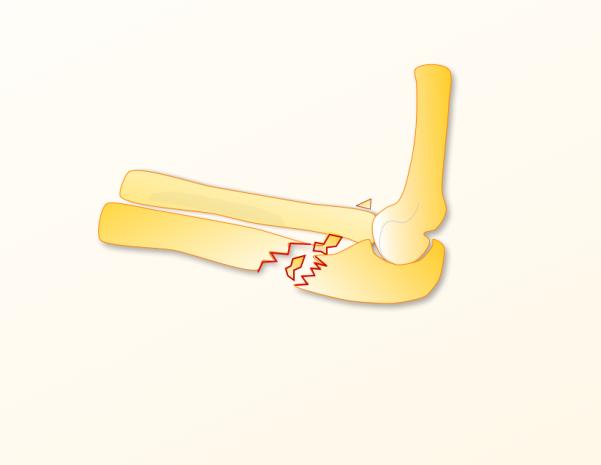
IV
(Figure 6D) |
Anterior | Diaphyseal | Diaphyseal | 1% | – |
The management of children with Monteggia fracture-dislocation has also been a subject of debate. Fahmy (1980) from Salford, England, and then Letts and colleagues (1985) from Manitoba, Canada, suggested a Monteggia equivalent that Bado did not refer to in his classification and that is only found in children. (27-28) This equivalent lesion has no fracture but rather a bend of the ulna (plastic deformation of immature bone) that is sufficient to permit the radial head to dislocate anteriorly. Letts acknowledged that lack of appreciation of this variant could have contributed to cases of missed Monteggia fracture-dislocations in children, and he proposed a new classification that takes equivalent lesions into consideration (Table 2). Wiley and Galey from Ottawa, Canada presented the results of 46 children with Monteggia fracture-dislocations and suggested closed reduction and splinting in supination and elbow flexion for 3 weeks. (29) Nineteen out of the 46 patients had associated olecranon fractures. This association seen more often in Bado type III injuries (12/18 cases), and the authors felt that patients with olecranon fractures should also be included as a Monteggia injury. This contrasted with the opinion of other surgeons to whom the involvement of the olecranon meant that the injury was not a true Monetggia fracture-dislocation. (22)
Table 2.
Letts classification of pediatric Monteggia fracture dislocation
| Letts classification | Description |
|---|---|
|
A
(Figure 7A) |
Anterior bend of the ulnar shaft with anterior dislocation of the radial head(Plastic deformation) |
|
B
(Figure 7B) |
Greenstick fracture of the ulnar shafyt with anterior dislocation of the radial head |
|
C
(Figure 7C) |
Anterior complete fracture of the ulnar shaft with anterior dislocation of the radial head |
|
D
(Figure 7D) |
Fracture of the ulnar shaft with posterior dislocation of the radial head |
|
E
(Figure 7E) |
Fracture of the ulnar shaft with lateral dislocation of the radial head |
Current Period (1991 till date)
In 1991, Jupiter and colleagues from Boston expanded on Bado’s type II description of posterior Monteggia fracture-dislocation to further highlight the location and type of ulna fracture as well as the pattern of radial head injury. They introduced an additional 4 subtypes IIA-IID (Table 3). (30) Jupiter and colleagues showed that fractures involving the olecranon are associated with poorer outcomes. Similar poor results of Monteggia fracture-dislocations associated with olecranon fracture were also reported on a series of 67 adult patients by Reynders etl al. from Leuven, Belgium in 1996. (31)
Table 3.
Jupiter Classification of Posterior Monteggia Fractures
| Jupiter Classification | Description | Jupiter Classification | Description |
|---|---|---|---|
|
II A
(Figure 8A) |
Fracture of the ulna involves the distal olecranon and coronoid process |
IIB
(Figure 8B) |
Fracture of the ulna is diaphyseal. |
|
IIC
(Figure 8C) |
Fracture of the ulna is distal to the coronoid process, involving the metaphyseal and diaphyseal junction |
IID
(Figure 8D) |
Fracture of the ulna which extends from the diaphysis to the olecranon |
This is a classification system built off of Bados type II lesion. It is based upon type and location of the ulnar fracture. In addition to the ulnar shaft fracture, radial head fractures have been further classified into R0: no fracture, R2: two part fracture, R3: three part fracture and C: comminuted fracture.
Open reduction with internal fixation of the ulna fracture and closed reduction of the radial head is currently the accepted treatment of choice of acute Monteggia fracture-dislocations in adults. (18, 32-33) A compression plate placed on the dorsal surface of the ulna, contoured around the olecranon especially with proximal and comminuted fractures, provides structural stability, resists ulnar angulation, and restores ulna length. In comminuted injuries a bone graft may be required to maintain ulnar length. Reduction of the radial head often ensues following an anatomic reduction and internal fixation of the ulna. Poor reduction of the ulna may result in persistent dislocation of the radial head. If the radial head is not stable following reduction of the ulna, interposition of ligamentous tissue or the posterior interosseous nerve should be considered, and a lateral approach is indicated. (33) Concomitant fractures of the radial head may be ignored if they are small and not disrupting forearm rotation. Excision of the radial head and replacement with prosthesis should be considered in displaced and severely comminuted fractures (Fig 9). (34)
Figure 9.
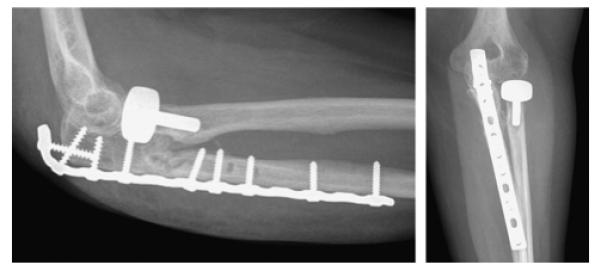
A long dorsal contoured plate achieved healing with good alignment of a posterior Monteggia lesion. Note replacement of radial head with radial head prothesis that achieved adequate articulation at the radiocapitellar joint.
In children most of injuries (e.g. plastic deformation, metaphyseal buckle fracture of the ulna) can be treated by closed reduction of the ulna with a combination of longitudinal traction, forearm rotation, and direct pressure applied to the apex of the fracture. Complete transverse and short oblique fractures can be treated by an open reduction and intramedullary nailing, however plates and screws are often required for long oblique and comminuted fractures. (32-33,35-36) Chronic or neglected lesions are more commonly seen in children and are frequently associated with chronic radiocapitellar instability and nonunion/malunion of the ulna fracture that leads to ulna shortening, pain, and limited forearm prono-supination. In chronic symptomatic radial head dislocations in children, reconstructive procedures include an open reduction of the radiocapitellar joint, annular ligament reconstruction, and corrective osteotomy of ulna malunion/nonunion. (32, 37) In adults an excision of the radial head can be considered. (38)
Future directions
Strauss and colleagues from New York investigated a rare subtype of Bado type II Monteggia fracture-dislocation. (39) In addition to the proximal ulna fracture-dislocation and posterior radial head fracture-dislocation, this subset includes posterior ulnohumeral dislocation, which accompany the injury. Dislocation of the ulnohumeral joint usually results from high-energy injuries such as a fall on the outstretched hand with the arm abducted that causes failure of the posterior capsule and lateral collateral ligaments. Their series included 23 patients with Bado type II Monteggia fracture-dislocation, of whom 6 patients had an accompanying posterior ulnohumeral dislocation. Comparison between patients with ulnohumeral dislocation (n=6) and patients without (n=17) showed poorer outcomes of the former in terms of elbow motion (flexion, extension, pronation, and supination). Greater disability was also noted in patients who experienced ulnohumeral dislocation when evaluated by outcome scores including the Disabilities of the Arm, Shoulder or Hand questionnaire and the functional rating index of Broberg and Morrey. However there was no recurrence of ulnohumeral instability following lateral collateral ligament reconstruction. The authors finally highlighted the need of recognition and repair of elbow soft-tissue stabilizers such as the lateral collateral ligament complex and warned against poor outcomes associated with this type of injury. Further studies with larger number of patients might be required to further study the impact of soft-tissue stabilizers and their repair on the functional outcome of the elbow joint following posterior (type II) Monteggia fracture-dislocations.
LIVES OF THE SURGEONS
Giovanni Battista Monteggia (1762-1815)
Giovanni Battista Monteggia (Fig.10) was born on August 8, 1762 in Laveno, Italy. (40) At age 17, Monteggia went to study surgery at Ospedale Maggiore in Milan, and later he completed his examination for the free practice of surgery at the University of Pavia. (40-41) Becoming engrossed in anatomy as a surgical student, Monteggia requested to have his office at Maggiore Hospital in order to be close to the dissection rooms so that he could nurture this passion. This nurturing influenced Monteggia’s first published work Fasciculi Pathologici in 1789 in Milan, which detailed his dissections and examination of varying lesions of the human body. (42)
Figure 10.

Giovanni Battista Monteggia (1762-1815).
In 1795 Monteggia treated his most prominent patient, Duke Francesco Melzi d’Eril. After several physicians had declared him near death, Monteggia was called upon for a final examination. Under Monteggia’s care, Francesco Melzi d’Eril made a full recovery. To show his gratitude, the Duke presented Monteggia with an annuity and appointed him as his personal physician. Monteggia used this annuity for access to a multitude of publications to support his future research. (43) Between 1795 and 1800, Monteggia was a professor of surgery at Maggiore Hospital, a delegate for the inoculation of the smallpox vaccine, a member of the Standing Committee on Health, and chair of surgery at Maggiore Hospital. Monteggia also continued to work tirelessly as a practicing physician and researcher, leading him to write his masterpiece publication ‘Istituzioni Chirurgiche’, which was published several times in Milan, Naples, and Pavia. The first edition of this work came in 5 volumes and was published in Milan between 1802 and 1805. The second edition, in which he described the forearm fracture-dislocation, was 8 volumes and appeared in print between 1813 and 1816. These publications discussed a variety of surgical problems such as gangrene, rheumatism, tumors, wounds, fractures, and many other diseases he encountered in his practice. Monteggia described the pathogenesis of poliomyelitis from a clinical perspective. At age 52, Monteggia died on January 17, 1815 after experiencing fever and a skin infection that started around his ear and quickly spread over his face. (41, 43)
Jose Luis Bado (1903 – 1977)
Jose Luis Bado (Fig. 11) was born in Montevideo, Uruguay on July 8, 1903. Bado studied medicine at the Universidad de la República, Montevideo and graduated at the top of his class in 1928. He then travelled to the Instituto Rizzoli in Bologna, which a the center of orthopedic surgery at the time. (44) Unlike Monteggia, Bado focused all his efforts on orthopedic surgery. Along with his clinical practice Bado immersed himself into research. He was constantly seen recording pertinent scientific observations related to his field and meditating on his notes, a practice that he preached to his colleagues and students. (45)
Figure 11.
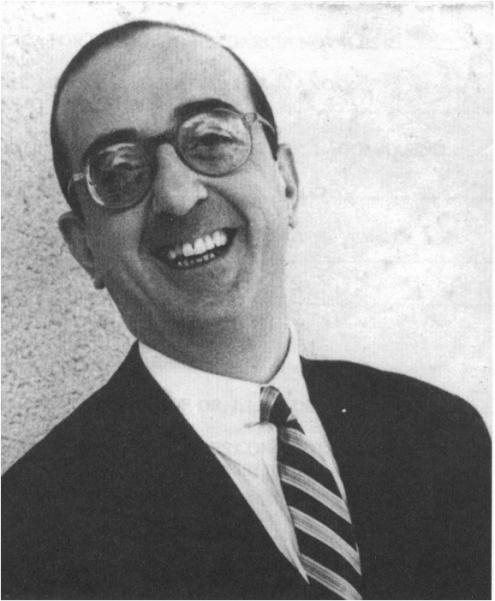
Jose Luis Bado (1903-1977).
Upon his return from Italy, Bado established the Instituto Traumatologico de Montevideo, later referred to as Instituto de Ortopedia y Traumatologia. Bado single handedly brought the practice of orthopedic surgery to Uruguay and across South America. Throughout his career, he was seen as a resource of information and constant inspiration to those around him. Bado’s immense dedication to his specialty is apparent in his 130 published articles and 12 published books throughout his lifetime. (44) Bado passed away in his hometown Montevideo on December 19, 1977 at age 74.
Although controversies have long surrounded the diagnosis and treatment of Monteggia injury, the legacy of Monteggia and Bado have inspired many generations of orthopedic surgeons around the world and substantially influenced the modern management of this complex fracture. One can hope that their contributions will be long remembered and celebrated.
Figure 6A-D.
Incorporate in Table 1. No separate figure legends required.
Figure 7A-E.
Incorporate in Table 2. No separate figure legends required.
Figure 8A-D.

Incorporate in Table 3. No separate figure legends required.
Acknowledgements
We would like to acknowledge Dr. Antonio L. Turnes from Montevideo, Uruguay for sharing biographical information and photographs of Prof. Jose Luis Bado. His assistance is greatly appreciated.
Supported in part by grants from Seed funding provided through the MCubed program at the University of Michigan and the National Institute of Arthritis and Musculoskeletal and Skin Diseases and National Institute on Aging (R01 AR062066) and from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (2R01 AR047328-06) and a Midcareer Investigator Award in Patient-Oriented Research (K24 AR053120) (to Dr. Kevin C. Chung).
Footnotes
Disclosure: None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
References
- 1.Monteggia GB. Lussazioni delle ossa delle estremita superiori. In: Monteggia GB, editor. Instituzioni Chirurgiches. 2nd Vol. 5. Maspero; Milan, Italy: 1814. pp. 131–133. [Google Scholar]
- 2.Perrin J. Les fractures du cubitus accompagnees de luxation de l'extremite superieur du radius. In: Perrin J, editor. These de Paris. G Steinheil; Paris, France: 1909. [Google Scholar]
- 3.Bado JL. La lesion de Monteggia. Inter-Medica Sarandi; 1958. p. 328. [Google Scholar]
- 4.Bado JL. The Monteggia lesion. Charles C. Thomas; Springfield, IL: 1959. [Google Scholar]
- 5.Bado JL. The Monteggia lesion. Clin Orthop. 1967;50:71–86. [PubMed] [Google Scholar]
- 6.Cooper AS. Dislocations and Fractures of the Joints. TR Marvin; Boston, MA: 1844. pp. 391–400. [Google Scholar]
- 7.Doerfler H. Fractur der Ulna in ihrem oberen Drittel combinirt mit Luxatimt des Radius. Deutsche Zeitschrift für Chirurgie. 1886;23(3-4):338–361. [Google Scholar]
- 8.Malgaigne M. Revue medico-chirurgicale de Paris. XIII. Tome Quinzieme; Paris, France: 1854. pp. 213–215. 80. [Google Scholar]
- 9.Stimson LA. Dislocation of the head of the radius with fracture of the ulna. In: Stimson LA, editor. A practical treatise on fractures and dislocations. 3rd Lea Brothers & Co; New York, NY and Philadelphia, PA: 1900. pp. 662–663. [Google Scholar]
- 10.Wilson PD. Fractures and Dislocations in the Region of the Elbow. Surg Gynec Obstet. 1933;LVI:335. [Google Scholar]
- 11.Cunningham SR. Fractures of the Ulna with dislocations of the head of the radius. J Bone Joint Surg Am. 1934;16(2):351–354. [Google Scholar]
- 12.Naylor A. Monteggia fractures. British Journal of Surgery. 1942;115(29):323–326. [Google Scholar]
- 13.Harness NG, Meals RA. The history of fracture fixation of the hand and wrist. Clin Orthop Relat Res. 2006;445:19–29. doi: 10.1097/01.blo.0000205882.73705.50. [DOI] [PubMed] [Google Scholar]
- 14.Speed JS, Boyd HB. Treatment of fractures of Ulna with dislocation of head of radius (Monteggia fracture) JAMA. 1940;115(20):1699–1705. [Google Scholar]
- 15.Thompson HA, Hamilton AT. Monteggia fracture: Internal fixation of the fractured ulna with intramedullary steinmann pin. AM J Surg. 1950;79(4):579–584. [Google Scholar]
- 16.Evans EM. Pronation injuries of the forearm, with special reference to the anterior Monteggia fracture. J Bone Joint Surg Br. 1949;31B(4):578–588. [PubMed] [Google Scholar]
- 17.Tompkins DG. The anterior Monteggia fracture: observations on etiology and treatment. J Bone Joint Surg Am. 1971 Sep;53(6):1109–1114. [PubMed] [Google Scholar]
- 18.Eathiraju S, Mudgal CS, Jupiter JB. Monteggia fracture-dislocations. Hand Clin. 2007;23(2):165–177. doi: 10.1016/j.hcl.2007.01.008. [DOI] [PubMed] [Google Scholar]
- 19.Penrose JH. The Monteggia fracture with posterior dislocation of the radial head. J Bone Joint Surg Br. 1951;33B(1):65–73. doi: 10.1302/0301-620X.33B1.65. [DOI] [PubMed] [Google Scholar]
- 20.Smith FM. Monteggia fractures; an analysis of 25 consecutive fresh injuries. Surg Gynecol Obstet. 1947;85(5):630–640. [PubMed] [Google Scholar]
- 21.Boyd HB, Boals JC. The Monteggia lesion. A review of 159 cases. Clin Orthop Relat Res. 1969;66:94–100. [PubMed] [Google Scholar]
- 22.Bruce HE, Harvey JP, Wilson JC., Jr Monteggia fractures. J Bone Joint Surg Am. 1974;56(8):1563–1576. [PubMed] [Google Scholar]
- 23.May VR, Jr, Mauck W. Dislocation of the radial head with associated fracture of the ulna. (Monteggia fracture) South Med J. 1961;54:1255–1261. doi: 10.1097/00007611-196111000-00008. [DOI] [PubMed] [Google Scholar]
- 24.Barquet A, Caresani J. Fracture of the shaft of ulna and radius with associated dislocation of the radial head. Injury. 1981;12(6):471–476. doi: 10.1016/0020-1383(81)90166-2. [DOI] [PubMed] [Google Scholar]
- 25.Bell Tawse AJ. The treatment of malunited anterior Monteggia fractures in children. J Bone Joint Surg Br. 1965;47(4):718–723. [PubMed] [Google Scholar]
- 26.Pavel A, Pitman JM, Lance EM, Wade PA. The posterior Monteggia fracture: A clinical study. J Trauma. 1965;5:185–199. doi: 10.1097/00005373-196503000-00006. [DOI] [PubMed] [Google Scholar]
- 27.Fahmy NR. Unusual Monteggia lesions in children. Injury. 1981;12(5):399–404. doi: 10.1016/0020-1383(81)90011-5. [DOI] [PubMed] [Google Scholar]
- 28.Letts M, Locht R, Wiens J. Monteggia fracture-dislocations in children. J Bone Joint Surg Br. 1985;67(5):724–727. doi: 10.1302/0301-620X.67B5.4055869. [DOI] [PubMed] [Google Scholar]
- 29.Wiley JJ, Galey JP. Monteggia injuries in children. J Bone Joint Surg Br. 1985;67(5):728–731. doi: 10.1302/0301-620X.67B5.4055870. [DOI] [PubMed] [Google Scholar]
- 30.Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM. The posterior Monteggia lesion. J Orthop Trauma. 1991;5(4):395–402. doi: 10.1097/00005131-199112000-00003. [DOI] [PubMed] [Google Scholar]
- 31.Reynders P, De Groote W, Rondia J, Govaerts K, Stoffelen D, Broos PL. Monteggia lesions in adults. A multicenter Bota study. Acta Orthop Belg. 1996;62(Suppl 1):78–83. [PubMed] [Google Scholar]
- 32.Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg. 1998;6(4):215–224. doi: 10.5435/00124635-199807000-00003. [DOI] [PubMed] [Google Scholar]
- 33.Ring D. Monteggia fractures. Orthop Clin North Am. 2013;44(1):59–66. doi: 10.1016/j.ocl.2012.08.007. [DOI] [PubMed] [Google Scholar]
- 34.McGlinn EP, Sebastin SJ, Chung KC. A historical perspective on the Essex-Lopresti injury. J Hand Surg Am. 2013;38(8):1599–1606. doi: 10.1016/j.jhsa.2013.04.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bae DS, Waters PM. Surgical Treatment of Acute and Chronic Monteggia Fracture-Dislocations. Operative Techniques in Orthopaedics. 2005;15(4):308–314. [Google Scholar]
- 36.Alexander MG, Graham HK. Chapter 13 Dislocations of the Elbow in Children. In: Stanley David, Trail Ian., editors. Operative Elbow surgery. Churchill Livingstone; New York, NY: 2011. pp. 214–221. [Google Scholar]
- 37.Wilkins KE. Changes in the management of monteggia fractures. J Pediatr Orthop. 2002;22(4):548–554. [PubMed] [Google Scholar]
- 38.Fayaz HC, Jupiter JB. Monteggia fractures in adults. Acta Chir Orthop Traumatol Cech. 2010;77(6):457–462. [PubMed] [Google Scholar]
- 39.Strauss EJ, Tejwani NC, Preston CF, Egol KA. The posterior Monteggia lesion with associated ulnohumeral instability. J Bone Joint Surg Br. 2006 Jan;88(1):84–89. doi: 10.1302/0301-620X.88B1.16704. [DOI] [PubMed] [Google Scholar]
- 40.Acerbi FE. Della Vita Di Giambatista Monteggia. Dalla Stamperia Dova; Milano, Italy: 1816. [Google Scholar]
- 41.Fiamberti AM. The life and works of Giovanni Battista Monteggia (8TH August, 1762-17TH January, 1815). A commerative Talk on the bicentary of his birth. Panminerva Med. 1963;104:427–430. [PubMed] [Google Scholar]
- 42.Conforti Maria, Monteggia Giovanni Battista. Biographical Dictionary of Italian L'enciclopedia Italiana. 2012 Treccani.it. Web. 23 Jul. 2013. http://www.treccani.it/enciclopedia/giovanni-battista-monteggia_(Dizionario-Biografico, Last accessed 12/04/2013)
- 43.Peltier LF. Eponymic fractures: Giovanni Battista Monteggia and Monteggia's fracture. Surgery. 1957;42(3):585–591. [PubMed] [Google Scholar]
- 44.Bado Jose Luis. The Journal of Bone & Joint Surgery. 1979;61(1):153–154. 1903--1977. [PubMed] [Google Scholar]
- 45.Mostofi SB. Who's Who in Orthopedics. Springer; London: 2005. pp. 17–18. [Google Scholar]