

Abstract
Ectopic liver tissue (ELT) is a rare condition, which is usually not diagnosed preoperatively, but coincidentally during abdominal surgery. While the location of ELT can vary, it is usually localized on the gallbladder wall or in close proximity. ELT is associated with various complications, a major complication being extrahepatic hepatocellular carcinoma. A 59-year-old female underwent elective surgery for chronic cholecystitis with stones. During laparoscopic exploration, a 2-cm-diameter ELT was detected in the anterior gallbladder wall and a laparoscopic cholecystectomy was performed. The case is presented due to the rare nature of ELT and as a reminder of ELT-related complications.
Keywords: Ectopic liver tissue, Laparoscopic cholecystectomy, Hepatocellular carcinoma
Core tip: Ectopic hepatic tissue is a rare condition and it has been reported in several sites, such as the gallbladder, gastrohepatic ligament, adrenal glands, and esophagus. It is usually clinically silent and found incidentally. Ectopic hepatic tissue carries an increased risk of malignant degeneration to hepatocellular carcinoma. It should be discovered and removed by the surgeon to prevent a higher risk of complications and malignant transformation.
INTRODUCTION
Congenital localization anomalies of the liver are rare, and can be classified into two major subgroups: those that are connected to the main liver tissue mechanically, and those that are not[1]. Ectopic liver tissue (ELT) is a subtype that is not connected to the main liver tissue, and it can be present in any intra-abdominal or supradiaphragmatic location. The most frequent intra-abdominal location is the gallbladder, and ELT is generally identified by recognizing extra tissue on the gallbladder wall that is of the same color as liver tissue[2].
First defined in 1922, ELT can vary in size, from microscopic scales to 3 cm in diameter. Despite its small size, since it is liver tissue histopathologically, it is prone to parenchymal diseases of the liver, including carcinoma development. Due to its small size, ELT is generally not noticed during routine radiological examinations; however, when noticed, it might be necessary to differentiate it from various conditions, including gallbladder cancer[3].
Here, we present a case of ELT on the gallbladder wall, which was detected during surgery, and review the relevant literature.
CASE REPORT
A 59-year-old female presented to the general surgery clinic with occasional epigastric pain and dyspeptic complaints for 2 mo. She had no history of systemic disease, previous abdominal surgery, or regular medication use, and her physical examination and laboratory tests were normal. Abdominal ultrasonography (USG) revealed a large number of millimeter-size stones in the gallbladder lumen, and she was scheduled to undergo an elective cholecystectomy. Laparoscopic exploration revealed a 2 cm × 1 cm tissue mass located in the fundus of the anterior gallbladder wall, which had the same color as the liver (Figure 1). The patient was diagnosed as having ELT on the gallbladder wall, and underwent a laparoscopic cholecystectomy (Figure 2). She did not have any postoperative problems, and was discharged on the second day. Following histopathological examination, the tissue attached to the gallbladder wall was confirmed to be ELT. The specimen examination showed that it was a truly ectopic liver and was not connected to the mother liver. The patient has been followed without any problems for 5 mo.
Figure 1.
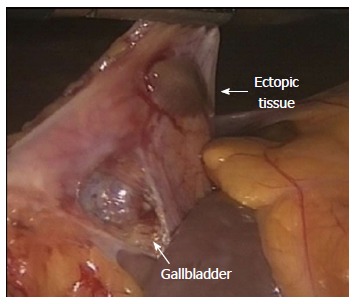
Laparoscopic exploration: A 2 cm × 1 cm cm tissue mass located at the gallbladder wall, which had the same color as the liver.
Figure 2.

Laparoscopic cholecystectomy material with ectopic tissue.
DISCUSSION
Ectopic liver tissue is a rare condition that is usually detected coincidentally during a post-mortem examination or abdominal surgery. According to the literature, the incidence of ELT at laparoscopy or laparotomy is 0.24%-0.47%[4]. In a 5500-case autopsy series, the incidence of ELT was 0.05%[5], while its incidence was 0.47% in a 1060-case laparoscopic surgery series[6]. During the past 5 years, 5000 patients underwent abdominal surgery at our clinic for various reasons and ELT was observed in a single patient (0.02%), the case presented here.
The most frequent localization of ELT is the gallbladder, although other sites have been reported, including the adrenal glands, pancreas, spleen, falciform ligament, pylorus, umbilicus, retroperitoneum, thorax (intrapleural/extrapleural), and pericardium[2]. ELT is generally asymptomatic, but it can present with recurrent abdominal pain due to torsion, hemorrhagic necrosis, or rupture, or with pressure symptoms due to mass formation as a consequence of malignant degeneration[7]. We believe that our patient’s non-specific complaints were due to cholecystopathy, and not associated with the ELT, because there was not pathological appearance of ELT such as torsion, necrosis.
Various theories have been presented to explain the development of ELT at different sites, and ELT can be seen together with biliary atresia, caudate lobe agenesis, omphalocele, and certain congenital cardiac anomalies[8]. We did not observe any comorbid anomalies in our case. It is a truly ectopic liver and is not connected to the mother liver. The ectopic liver tissue presents resulting from liver tissue migration to fundus of gallbladder during embryogenesis.
Ectopic liver tissue is not noticed during radiological examinations, as it is generally asymptomatic, rare, small in size, or the examiner is not aware of this entity. The diagnosis of ELT should be considered when a soft-tissue mass is detected on the gallbladder wall using USG or computed tomography. Color Doppler USG and angiography can show the blood vessel feeding the liver. However, the incidence of radiological detection is low, and the number of reported cases for which a preoperative diagnosis has been made is very limited[2,3]. When noted radiologically, the exact diagnosis is made by showing the presence of hepatic tissue in a percutaneous biopsy; however, this is not a suggested method for diagnosis, due to the bleeding risk and malignant degeneration[4].
The normal progression of ELT is not known. Since it is liver tissue, it is affected by the same risk factors affecting the liver, and lipid infiltration, cirrhotic changes, chronic active hepatitis, hemosiderosis, metastatic tumors, and hepatocellular carcinoma (HCC) have been reported to develop in ELT[8]. The development of HCC is the most important condition, and involves a higher risk of neoplastic transformation that is independent of the main liver tissue. The lack of complete functional structure for neoplastic transformation in small ELT, absence of vascular and ductal systems, and possible metabolic insufficiency are believed to contribute to the carcinogenetic process[4,9].
In conclusion, ELT is a rare condition, and it is difficult to make a radiological diagnosis. When seen during a surgical intervention, it should be excised because of the possibility of developing a malignancy.
COMMENTS
Case characteristics
Patient presented to the general surgery clinic with occasional epigastric pain and dyspeptic complaints for 2 mo.
Clinical diagnosis
Patient had no history of systemic disease, previous abdominal surgery, or regular medication use, and her physical examination was normal.
Laboratory diagnosis
Laboratory tests were normal.
Imaging diagnosis
Abdominal ultrasonography revealed a large number of millimeter-size stones in the gallbladder lumen.
Pathological diagnosis
Following histopathological examination, the tissue attached to the gallbladder wall was confirmed to be liver tissue.
Treatment
The patient was underwent a laparoscopic cholecystectomy.
Related reports
Laparoscopic exploration revealed a 2 cm × 1 cm tissue mass located in the fundus of the anterior gallbladder wall.
Experiences and lessons
Ectopic liver tissue is a rare condition, and it is difficult to make a radiological diagnosis. When seen during a surgical intervention, it should be excised because of the possibility of developing a malignancy.
Peer review
This paper was concise and well-written.
Footnotes
P- Reviewer: Lau WY, Murata A, Tagaya N S- Editor: Ji FF L- Editor: A E- Editor: Wu HL
References
- 1.Collan Y, Hakkiluoto A, Hästbacka J. Ectopic liver. Ann Chir Gynaecol. 1978;67:27–29. [PubMed] [Google Scholar]
- 2.Lundy J, Johnson E, Edwards K, Rivera D. Laparoscopic management of gallbladder-associated ectopic liver. JSLS. 2005;9:485–487. [PMC free article] [PubMed] [Google Scholar]
- 3.Hamdani SD, Baron RL. Ectopic liver simulating a mass in the gallbladder wall: imaging findings. AJR Am J Roentgenol. 1994;162:647–648. doi: 10.2214/ajr.162.3.8109514. [DOI] [PubMed] [Google Scholar]
- 4.Martinez CA, de Resende HC, Rodrigues MR, Sato DT, Brunialti CV, Palma RT. Gallbladder-associated ectopic liver: A rare finding during a laparoscopic cholecystectomy. Int J Surg Case Rep. 2013;4:312–315. doi: 10.1016/j.ijscr.2013.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eiserth P. Beitrage zur Kenntnis der Nebenlebern. Virchows Arch A Pathol Anat Histopathol. 1940;307:307–313. [Google Scholar]
- 6.Watanabe M, Matsura T, Takatori Y, Ueki K, Kobatake T, Hidaka M, Hirakawa H, Fukukmoto S, Shimada Y. Five cases of ectopic liver and a case of accessory lobe of the liver. Endoscopy. 1989;21:39–42. doi: 10.1055/s-2007-1012892. [DOI] [PubMed] [Google Scholar]
- 7.Nagar S, Koffron A, Raofi V. A Case of Hemorrhagic Necrosis of Ectopic Liver Tissue within the Gallbladder Wall. HPB Surg. 2011;2011:389381. doi: 10.1155/2011/389381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Griniatsos J, Riaz AA, Isla AM. Two cases of ectopic liver attached to the gallbladder wall. HPB (Oxford) 2002;4:191–194. doi: 10.1080/13651820260503873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Beltran MA, Barria C, Pujado B, Barrera R, Mendez P, Pozo C. Hepatic heterototopic tissue on the gallbladder wall: an incidental finding with pathological potential. J Gastrointestin Liver Dis. 2007;16:347–349. [PubMed] [Google Scholar]