

Description
A 50-year-old woman presented with a 3-month history of intermittent right-sided chest pain and haemoptysis. She did not have a cough, wheeze or dyspnoea and there was no history of fever, anorexia or weight loss. Skiagram chest posteroanterior view showed triangular opacity in the right upper zone along with elongated opacity along the right paratracheal area (figure 1).
Figure 1.
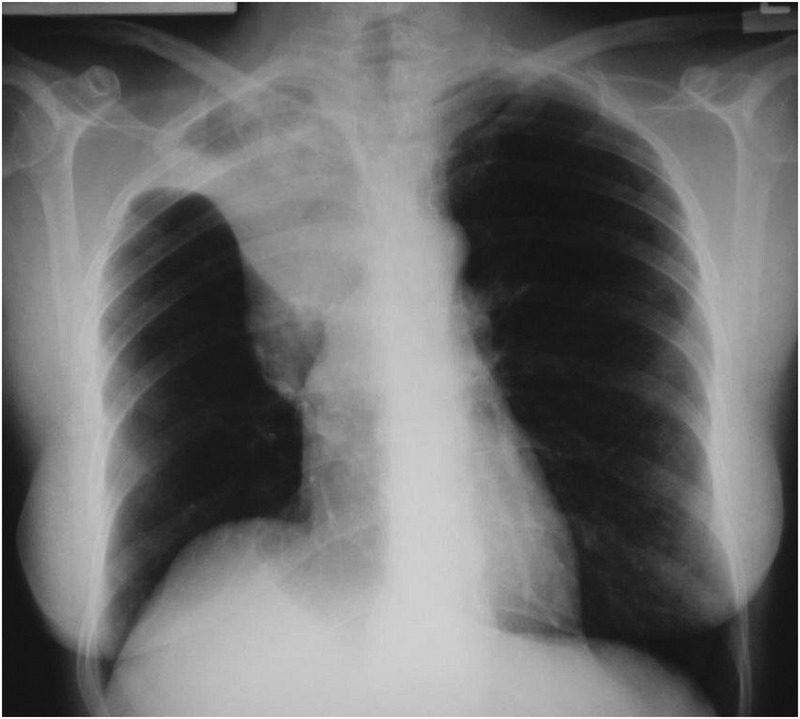
Chest X-ray posteroanterior view shows two different opacities, one is triangular shaped and in the right upper zone, while the other is elongated and along the right paratracheal area.
Contrast-enhanced CT (CECT) of the thorax showed right upper lobe collapse along with the abrupt cutting of right upper lobe bronchus and mediastinal lymphadenopathy (figure 2). Flexible fibre optic bronchoscopy revealed a growth in the right upper lobe bronchus, which proved to be small cell anaplastic carcinoma on histopathological examination.
Figure 2.
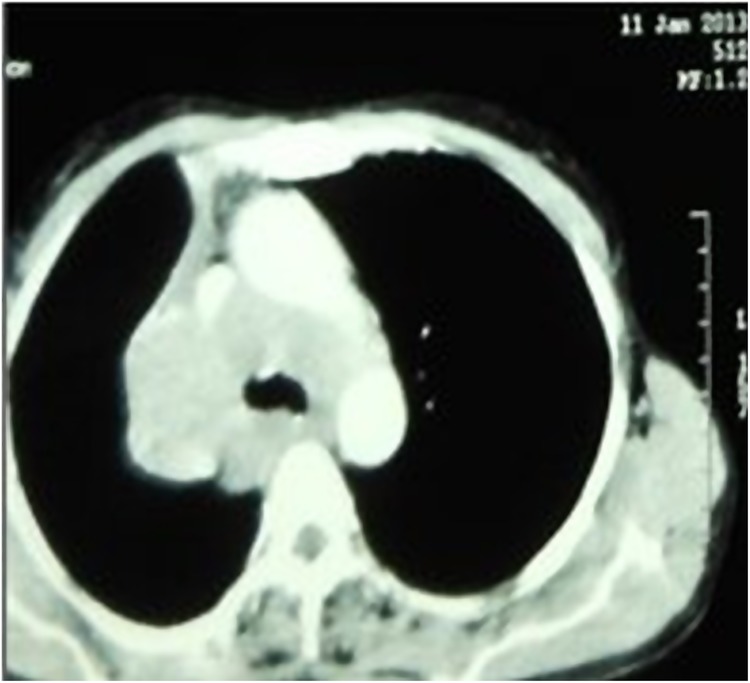
Contrast-enhanced CT of the thorax showing right upper lobe collapse with abrupt cutting of the right upper lobar bronchus and mediastinal lymphadenopathy.
Lobar collapse of the lung may present with a varied combination of direct and indirect signs. The Golden ‘S’ sign is one of them. This sign, also known as ‘Reverse S sign of Golden’, refers to the X-ray appearance of right upper lobe collapse with right hilar enlargement.1 The latter may be seen more clearly on CECT of the thorax.1 2 This sign was first recognised and described by Ross Golden in 1925 in conjunction with bronchogenic carcinoma of the lung, which still remains the most common cause for this radiological sign;1 3 however, other conditions such as lymph node metastasis from other carcinomas, lymphadenopathy due to other aetiologies or primary mediastinal tumours may also lead to this radiological curiosity.1
Distortion of the minor fissure is caused by collapse of the right upper lobe (the lateral part of the curve, which is concave inferiorly) and the underlying endobronchial pathology (the medial part of the curve, which is convex inferiorly). Right upper lobe collapse causes the minor and major fissures to move superiorly and medially toward the mediastinum. This results in the downward concavity of the minor fissure and the triangular opacity represents the collapsed lobe located at the hilum.1
Learning points.
Lobar collapse of a lung is a significant pathology by itself, but the presence of the Golden S sign on the plain radiograph should raise the suspicion of an underlying endobronchial pathology, that is, bronchogenic carcinoma and a bronchoscopy is warranted.
Although this sign is not specific and bronchogenic carcinoma cannot be diagnosed definitively on the basis of this sign alone, it should serve to alert the clinician to the possibility of a centrally obstructing mass as a cause of collapse, as was the case in our patient.
Acknowledgments
The authors would like to acknowledge Dr PR Gupta for his help in editing and proofreading of the manuscript.
Footnotes
Contributors: MLB and RT contributed to the conception of the image quiz, and the acquisition and analysis of material. SA and RB were involved in analysis and interpretation of material for the work. All the authors were involved in drafting the report and revising it critically before final submission for publication.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Gupta P. The Golden S sign. Radiology 2004;233:790–1. [DOI] [PubMed] [Google Scholar]
- 2.Reinig JW, Ross P. Computed tomography appearance of Golden's “S” sign. J Comput Tomogr 1984;8:219–23. [DOI] [PubMed] [Google Scholar]
- 3.Golden R. The effect of bronchostenosis upon the roentgen ray shadow in carcinoma of the bronchus. Am J Roentgenol 1925;13:21. [Google Scholar]