

Abstract
Sexual minorities have higher rates of depression and anxiety than their heterosexual counterparts. This elevated risk of psychological distress has generally been hypothesized to be a result of the effects of discrimination including internalized negative beliefs about sexual minorities. However, little research has examined the role of various types of coping in mediating between internalized homophobia and mental health. We tested the direct relationship between internalized homophobia and psychological distress and evaluated general and sexual minority-specific coping strategies as potential mediators using structural equation modeling. Data are from a national sample of 1,099 young adult sexual minority women who were on average 20.86 (SD= 2.12) years old, participating in a study on mental health and substance use. The model demonstrated acceptable fit, χ2 (83) = 402.9, p <.001, CFI=.94, TLI=.92, SRMR= .07, and RMSEA=.06, accounting for 73% of variance in psychological distress. Greater use of maladaptive coping and less use of sexual minority-specific coping were associated with higher psychological distress. Although maladaptive coping mediated the relationship between internalized homophobia and psychological distress, sexual minority-specific coping did not. Our findings support previous studies that have demonstrated the impact of internalized homophobia on psychological distress as well as the role of coping as a protective/risk factor in this relationship.
Keywords: sexual minority women, young adults, depression, anxiety, coping
Introduction
A number of studies conducted over the past decade provide compelling evidence of mental health disparities between sexual minorities and their heterosexual counterparts (Bostwick, Boyd, Hughes, & McCabe, 2010; Hughes, Szalacha, & McNair, 2010; King et al., 2008; Meyer, 2003; Steele, Ross, Dobinson, Veldhuizen, & Tinmouth, 2009). In a seminal meta-analysis on the prevalence of mental disorders, Meyer (2003) concluded that sexual minorities were nearly two times as likely as heterosexuals to meet criteria for lifetime mood and anxiety disorders.
The most widely accepted theory proposed to explain the higher prevalence of mood and anxiety disorders among sexual minorities is the minority stress model (Herek & Garnets, 2007; Meyer, 2003). Based on this theory, sexual minorities are exposed to multiple stressors such as discrimination, microaggressions, stigma, and the need for concealment. These stressors then lead to increased psychological distress. Supporting this model, higher levels of stigma-related stressors have been associated with psychological distress in sexual minorities (King et al., 2008; Hatzenbuehler, Nolen-Hoeksema, & Erickson, 2008; Meyer, 2003).
Internalized homophobia is one stigma-related stressor that refers to the sexual minority individual’s “direction of negative social attitudes towards the self, leading to a devaluation of the self and resultant internal conflicts and poor self-regard” due to one’s sexual orientation (p.161; Meyer & Dean, 1998). It includes internalized negative attitudes toward homosexuality generally, discomfort with disclosure of sexual identity to others, and discomfort with same-sex sexual activity (Newcomb & Mustanski, 2010). Among sexual minority women, higher levels of internalized homophobia have been found to be associated with psychological distress (Meyer, 1995; Nicholson & Long, 1990; Szymanski, Kashubeck-West, & Meyer, 2008a). A small to moderate correlation between internalized homophobia and depression and anxiety have been reported in a meta-analytic review (Newcomb & Mustanski, 2010). Indeed, Meyer (2003) included internalized homophobia as a proximal stressor in his minority stress framework.
Clearly, however, not all sexual minorities who exhibit internalized homophobia develop mood or anxiety disorders. A more recent theory, the psychological mediation framework, builds upon the minority stress model and postulates that stress from stigma then leads to disruptions in psychological processes that mediate between stigma-related stress and psychopathology (Hatzenbuehler, 2009). One such psychological process is coping. Researchers have identified aspects of coping that may be protective and others that act as risk factors for psychopathology (Carver & Scheier, 1994; Folkman & Lazarus, 1985; Glass, Flory, Hankin, Kloos, & Turecki, 2009). One distinction in the literature is between problem-focused and emotion-focused coping. Problem focused coping involves actively planning or engaging in a specific behaviors to overcome the problem causing the distress and can include strategies like evaluating the pros and cons or implementing steps to solve a problem; this type of coping is generally viewed as adaptive and protective (Folkman & Lazarus, 1985). In contrast, emotion focused coping strategies involve regulating emotional distress and can include both active and avoidant aspects of coping, with the former considered adaptive and the latter maladaptive (Holahan & Moos, 1987). For example, emotion focused coping can include actively seeking emotional support and using positive reframing and humor, but also can include mental or behavioral disengagement, which would be avoidant. Research on coping shows that individuals typically use multiple types of strategies in response to stressful situations (Folkman & Lazarus, 1980) and these strategies are not mutually exclusive (Fleishman & Fogel, 1994; Schmitz & Crystal, 2000). One way to approach evaluating these coping strategies is to group them as either adaptive (i.e., problem focused coping, active emotion-focused coping) or maladaptive strategies (i.e., avoidant emotion-focused coping; Lehavot, 2012).
There is consistent support in the literature for the detrimental effect of maladaptive coping on psychological distress among sexual minorities (Szymanski, 2009; Szymanski & Carr, 2008; Talley & Bettencourt, 2011), especially in sexual minority women (Lehavot, 2012; Szymanski & Owens, 2008). In contrast, support for associations between adaptive coping and psychological distress is less robust (Glass, Flory, Hankin, Kloos, & Turecki, 2009; Schindler, Elhai, & Gray, 2007). Among sexual minority women findings are mixed, whereas higher endorsement of adaptive coping was associated with lower psychological distress in one study (Lehavot, 2012) but did not predict psychological distress in another (Szymanski & Owens, 2008).
Although coping has been thought of as a potential moderator between internalized homophobia and psychological distress in minority stress models, it also has been conceptualized as a mediator as well (Szymanski and Owens, 2008). As such, individuals with high internalized homophobia are thought to be more likely to engage in maladaptive coping, such as by avoiding same-sex behaviors and information and engaging in concealment (Cass, 1979; Sophie, 1987; Szymanski et al., 2008). Internalized homophobia may also inhibit the development of more adaptive coping strategies such as coming out to others or obtaining social support. Thus, coping strategies act as mediators because internalized homophobia is seen as leading to reductions in adaptive and increases in maladaptive coping strategies, which in turn leads to increased psychological distress. Given this model, it may be particularly important to evaluate the impact of internalized homophobia on both coping and psychological distress.
While internalized homophobia is theoretically linked with avoidant coping, little empirical research has examined this (Lehavot, 2012). To date, only two studies have specifically examined the effect of internalized homophobia on coping strategies among sexual minority women. One of these (Talley & Bettencourt, 2011) found perceived homophobia was significantly and positively associated with maladaptive coping (Talley & Bettencourt, 2011) in a combined sample of sexual minority males and females. Szymanski and Owens (2008), in testing the mediation model discussed above, found partial support for coping as a mediator between internalized homophobia and psychological distress among sexual minority women. Maladaptive or avoidant coping partially mediated the relationship between internalized heterosexism and psychological distress, however problem-solving coping did not mediate the link between internalized homophobia and distress. Given the lack of research on coping and internalized homophobia in general, and research including sexual minority women in particular, more research is warranted to understand relationships between internalized homophobia and both adaptive and maladaptive coping among sexual minority women.
In addition to examining coping more broadly, it is important to consider specific coping strategies used by sexual minority women. Sexual minority women may employ unique coping strategies to deal with a stigmatized identity and related stressors, which may not be represented in more general coping inventories. For instance, sexual minority-specific forms of coping may involve confronting discrimination, accessing support from the sexual minority community, or challenging one’s own internalized negative beliefs about sexual minorities (Bowleg, Craig, & Burkholder, 2004; Chung, Williams, & Dispenza, 2009; Czech & Waidzunas, 2011). Although theories of stress and coping in relation to sexual minorities discuss specific forms of coping utilized by sexual minorities, the studies conducted to date have not explicitly examined the extent to which sexual minority-specific coping is affected by internalized homophobia, and whether it, in turn, affects psychological distress. Nor have they examined whether sexual-minority specific coping plays a role in understanding psychological distress over and above general adaptive or maladaptive coping strategies.
Summary and Aims
Sexual minorities are at higher risk of psychological distress, including anxiety and depression, compared to heterosexual individuals (Bostwick et al., 2010; Hughes et al., 2010; King et al., 2008; Meyer, 2003). In accordance with the minority stress model, internalized homophobia has been identified as a proximal stressor that contributes to this elevated risk (Hatzenbuehler, 2009; Szymanski et al., 2008a). Coping may mediate the relationship between internalized homophobia and psychological distress (Szymanski & Owens, 2008). However, given the relatively scarce and mixed findings, there is a need for research to examine the role of coping broadly, as well as sexual minority-specific coping in the relationship between internalized homophobia and psychological distress.
Our objective was to evaluate the extent to which internalized homophobia may impact both general and sexual-minority specific coping, as one way to understand means by which internalized homophobia may lead to elevated psychological distress among sexual minority women. For the current study, psychological distress included both symptoms of anxiety and depression (Kessler et al., 1994). We hypothesized that higher internalized homophobia would be associated with higher psychological distress, and that this relationship would be mediated by coping (Szymanski & Owens, 2008). Specifically, we predicted that higher internalized homophobia would be associated with higher use of maladaptive coping, lower adaptive coping, and lower sexual minority-specific coping. In turn, higher maladaptive coping, lower adaptive coping, and lower sexual minority-specific coping would be associated with higher psychological distress. We build on the extant literature by: (1) examining these relationships in a large, national sample of young adult sexual minority women; (2) assessing both adaptive and maladaptive coping; (3) investigating the unique role of sexual minority-specific coping as a mediator.
Materials and Methods
Participants
The present sample consisted of 1,099 women ages 18–25, who completed the baseline assessment for a national study on mental health and substance use among lesbian and bisexual women. The mean age of participants was 20.86 years old (SD= 2.12), and 41% of the sample self-identified as lesbian and 59% as bisexual. We assessed participants’ sexual identity via the following question: “Understanding that sexual identity can be complex, which one category best describes your sexual identity now?” Participants were first asked this as a multiple choice question with an open-ended option. However, participants who did not indicate identifying as either lesbian or bisexual were then asked a follow-up forced choice question. The majority of the sample was Caucasian (69.3%); 12.1% African American, 3.4% Asian American, 1.4% American Indian/Alaskan Native, 0.3% Native Hawaiian/Pacific Islander, and 7.5% multiracial. Six percent of the sample identified as “other” race/ethnicity or did not respond to the question.
Procedures
Participants were recruited via online advertisements placed on the social networking site Facebook and on Craigslist in ethnically diverse cities (i.e., Chicago, New York). Interested participants then clicked on a link to be routed to the screening survey. Eligibility criteria included women who: 1) lived in the U.S., 2) had a valid e-mail address, 3) were between the ages of 18–25, and 4) self-identified as lesbian or bisexual at the time of the assessment. A total of 4,119 women completed the screening survey and 1,877 were eligible for the longitudinal study. Eligible participants received two automatic e-mails inviting them to take an additional 45-minute baseline survey. Once a participant logged into the baseline survey, they were shown a full consent form for the larger longitudinal study. Those that agreed to participate were then routed to the baseline survey and were compensated $25 for completing the survey. Non-completers received additional e-mail and telephone reminders. Of 1,877 eligible participants, 1,099 completed the survey. All measures and procedures were reviewed and approved by the local Institutional Review Board.
Measures
Internalized Homophobia
Lesbian Gay Bisexual Identity Scale (LGBIS (Mohr & Fassinger, 2000; Mohr & Kendra, 2011)
The LGBIS is comprised of six subscales: need for privacy, need for acceptance, homonegativity, difficult process, identity confusion, and superiority. For the current study, we focused on the homonegativity subscale, which is a measure of internalized homophobia and encompasses the following five items: “I would rather be straight if I could;” “I am glad to be an LGB person;” “Homosexual lifestyles are not as fulfilling as heterosexual lifestyles;” “I’m proud to be part of the LGB community;” and “I wish I were heterosexual.” Response options were based on a 7-point Likert scale ranging including 1 = strongly disagree to 7 = strongly agree. In the current study, Cronbach’s alpha was .78.
Psychological distress (Depression and Anxiety)
Center for Epidemiologic Studies Depression Scale (CESD; (Radloff, 1977)
The CESD includes 20 items such as “I felt lonely,” “I was bothered by things that usually don’t bother me,” and “I had crying spells.” We utilized the full measure, and participants were instructed to report how often, if ever, they experienced each item in the past month. Response options were based on a Likert scale ranging from 0 = rarely or none of the time (less than 1 day) to 3 = most or all of the time (5–7 days). Composite scores can range from 0 to 60. A score of 16 or higher is considered a clinically significant level of psychological distress (Radloff, 1977). In the current study, Cronbach’s alpha was .92.
Generalized Anxiety Disorder-7 (GAD-7; (Spitzer, Kroenke, Williams, & Löwe, 2006; Swinson)
Participants were asked to indicate how often, if at all, they were bothered in the past month by each of seven items (e.g., not being able to stop or control worrying; feeling nervous, anxious or on edge). Response options ranged from 0 = not at all to 3 = nearly every day. We utilized the full measure, and total score ranges from 0 to 21, and cut off scores for mild, moderate, and severe anxiety are 5, 10, and 15 respectively (Swinson). In the current study, Cronbach’s alpha was .91.
Coping Strategies
Brief Cope (BC; Carver, 1997) was used to examine how often participants used any of the 28 items presented as coping strategies. The BC can be broken down into the following 14 subscales: planning, instrumental support, emotional support, active coping, positive reframing, acceptance, venting, humor, religion, behavioral disengagement, denial, self-blame, self-distraction, and substance use. Response options included 1 = I haven’t been doing this at all, 2 = I’ve been doing this a little bit, 3 = I’ve been doing this a medium amount, and 4 = I’ve been doing this a lot. For the purpose of the present study, we aimed to identify adaptive and maladaptive coping. However, the scoring suggested by Carver (1997) does not lend itself to identify which items fall in any particular coping category. Moreover, Carver (2012) suggested that investigators use their own data to identify higher order coping factors from among the scales. Given these scoring instructions and in accordance with prior work in this area (Glass et al., 2009; Shnider, Elhai, & Gray, 2007), researchers have divided Brief Cope into more adaptive (planning, instrumental support, emotional support, active coping, positive reframing, acceptance, venting, humor, religion) and more maladaptive coping strategies (behavioral disengagement, denial, self-blame, self-distraction, and substance use). As such we next conducted a principal component analysis with Viramax orthogonal rotation forcing a two factor solution. Similar subscales identified by past research (Glass et al., 2009; Lehavot, 2012; Schnider et al., 2007) loaded on the maladaptive and adaptive coping factors. The adaptive factor had an Eigenvalue of 4.02 and explained 28.69% of variance while the maladaptive factor had an Eigenvalue of 2.47 and explained 17.63% of variance. Given a large number of subscales (i.e. 14), we decided to retain only subscales with loadings >.6 for parsimony. After removing emotional support, venting, humor, and religion, we ended up with the following subscales representing adaptive coping: active coping, planning, instrumental support, acceptance, positive reframing. For the maladaptive coping factor, subscales loadings were at least .67 Thus, we retained all subscales for this factor: behavioral disengagement, denial, self-blame, self-distraction, and substance use. In the current study, Cronbach’s alpha was .81 for maladaptive coping and .81 for the adaptive coping subscales.
Lesbian, Gay, Bisexual, Transgender (LGBT) Coping Scale (Molina, Balsam, & Beadnell, 2011)
We assessed LGBT-specific coping strategies using an unpublished 15 item scale that asked participants how often they used each coping method to cope with the challenges of being LGBT in the past 12 months. This instrument consists of 5 subscales that were initially developed from focus groups with diverse LGBT adults (Molina, Balsam, & Beadnell, 2011). The subscales (with sample items in parentheses) include Confronting Homophobia (“Having conversations with people who are homophobic in order to educate them”), Avoidance (“Trying not to be too ‘in your face’ about being LGBT”), Self-Acceptance (“Reminding myself that there is nothing wrong with being LGBT”), Spirituality (“Praying or Meditating”), and Online Support (“Connecting with a virtual community of LGBT people on the internet”). Response options were on a Likert scale of 0 = I have not been doing this at all to 3 = I have been doing this a lot. Cronbach’s alpha was .67 in this sample. In a prior study of 984 LGBT adults, the subscales showed good internal consistency reliability and construct validity (Molina, Balsam, & Beadnell, 2011). Due to our interests in the adaptive aspects of LBT-specific coping as well as to low factor loading, we elected to remove the avoidance subscale from our final model (see Model Fit Evaluation for more detail).
Analytic Plan
We used M-plus software, version 7 (Muthen and Muthen) to test the model (Figure 1). Four measures of model fit were calculated: Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), Standardized Root Mean Square Residual (SRMR), and the Root Mean Square Error of Approximation (RMSEA). Based on recommendations by Hu and Bentler (1999), models were considered to have adequate fit if CFI and TLI > .90, and SRMR and RMSEA < .08. In addition, we report the chi square, χ2; however, it should be noted that due to the large sample size in this study (N=1,099), it is likely that the χ2 would be significant despite being an adequate fitting model. We examined indirect effects of internalized homophobia through coping variables. Bootstrapped standard errors were estimated with 5,000 iterations in order to obtain 95% confidence intervals for the indirect effects.
Figure 1.
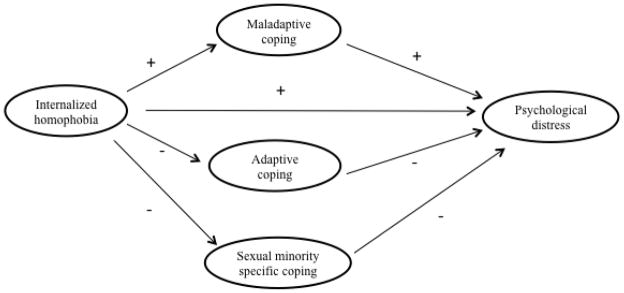
Hypothesized Path Model.
Note. Paths where a positive association was predicted are represented with a (+) sign, and paths where a negative association was predicted are represented with a (−) sign.
Missing data for the primary study variables ranged from .2% to 2.5%. To retain as much data as possible, we used full-information maximum likelihood estimation which provides valid estimates under the assumption that data were missing at random after accounting for measured variables (Schafer & Graham, 2002).
Results
The degree of mental health concerns was high among this sample of sexual minority women. Based on a cut off score of 16 on the CES-D, 69.4% of the current sample experienced clinically significant levels of recent depressive symptoms. In addition, based on the cut off scores for GAD-7, 15.6% reported subclinical symptoms of generalized anxiety, 14.8% mild symptoms, 25.8% moderate symptoms, and 43.8% severe symptoms.
Model Fit Evaluation
Measurement Model
The measurement model consists of all assessment instruments which map onto each latent factor represented in any given tested model. Descriptive statistics for the main study variables are summarized in Table 1. The following latent variables were included in our model: (1) internalized homophobia; (2) adaptive coping (active coping, planning, instrumental support, emotional support, positive reframing); (3) maladaptive coping (self-distraction, denial, substance use, behavioral disengagement, self-blame); (4) sexual minority-specific coping (confronting homophobia, avoidance, self-acceptance, spirituality, online support); and (5) psychological distress (depression and anxiety). Each of the latent factors is based on theory and/or prior research. Specifically, both adaptive and maladaptive coping factors are consistent with prior research with sexual minority women (Lehavot, 2012).
Table 1.
Descriptive Statistics for Psychological Distress, Coping, and Internalized Homophobia
| Variable | N | Mean (SD) |
|---|---|---|
| Psychological distress 1 | 1019 | 36.86 (18.84) |
| Anxiety | 1080 | 13.49 (7.68) |
| Depression | 1069 | 23.37 (12.43) |
| Internalized homophobia 2 | 1084 | 1.95 (1.01) |
| Rather be straight | 1062 | 2.00 (1.58) |
| Glad to be LGB person 3 | 1063 | 2.06 (1.35) |
| LGB lifestyle not fulfilling | 1065 | 1.70 (1.30) |
| Glad part of LGB community 3 | 1057 | 2.01 (1.27) |
| Wish was heterosexual | 1062 | 1.93 (1.43) |
| Maladaptive coping 1 | 1047 | 20.15 (5.81) |
| Self-distraction | 1079 | 5.34 (1.59) |
| Denial | 1072 | 2.93 (1.46) |
| Substance use | 1075 | 3.62 (1.99) |
| Behavioral disengagement | 1076 | 3.48 (1.63) |
| Self-blame | 1073 | 4.77 (1.92) |
| Adaptive coping 1 | 1057 | 25.98 (6.51) |
| Active coping | 1073 | 5.07 (1.71) |
| Planning | 1073 | 5.24 (1.79) |
| Acceptance | 1080 | 5.63 (1.63) |
| Positive reframing | 1078 | 4.97 (1.76) |
| Instrumental Support | 1084 | 5.04 (1.85) |
| Sexual minority-specific coping 1 | 1082 | 5.78 (2.51) |
| Confronting homophobia | 1083 | 1.07 (0.77) |
| Avoidance | 1082 | 1.09 (0.71) |
| Self-acceptance | 1082 | 2.25 (0.78) |
| Spirituality | 1083 | 0.45 (0.73) |
| Online support | 1082 | 0.91 (0.97) |
Scale score calculated as the sum of the subscales
Calculated as mean of items
Item was reverse coded
When we tested the measurement model, the latent factors were allowed to freely correlate. The model demonstrated close to acceptable fit, χ2 (220) = 2081, p <.001; CFI=.78; TLI=.75; SRMR=.08; and RMSEA=.09. Factor loadings for the indicators of each latent variable were >.30. After inspecting the modification indices, we chose to remove the lowest loading indicators for each of the coping factors. We removed the “self-distraction” indicator from maladaptive coping factor, “avoidance” (loading= .37) was removed from the sexual minority coping factor and “instrumental support” (loading=.51) was removed from the adaptive coping factor. Further, we allowed residuals of internalized homophobia indicators to correlate with one another. With the changes to the measurement model, we achieved acceptable fit of the measurement model, χ2 (158) = 768.6, p <.001, CFI=.91, TLI=.89, SRMR=.06, and RMSEA=.06. Table 2 shows more detailed information for the final measurement model.
Table 2.
Unstandardized and Standardized Coefficients for Indicators of Latent Constructs in the Measurement Model
| Unstandardized (SE) | Standardized | |
|---|---|---|
| Internalized homophobia | ||
| Rather was straight | 1 | .83 *** |
| Glad to be LGB | .43 (.03) | .42 *** |
| LGB lifestyle not fulfilling | .38 (.03) | .38 *** |
| Glad part of LGB community | .45 (.03) | .46 *** |
| Wish was heterosexual | .99 (.04) | .90 *** |
| Maladaptive coping | ||
| BC denial | 1 | .54 *** |
| BC substance use | 1.35 (.10) | .53 *** |
| BC behavioral disengagement | 1.48 (.09) | .72 *** |
| BC self-blame | 1.70 (.11) | .70 *** |
|
| ||
| Adaptive coping | ||
| BC positive reframing | 1 | .66 *** |
| BC active coping | 1.11 (.06) | .75 *** |
| BC planning | 1.25 (.07) | .81 *** |
| BC emotional support | .79 (.06) | .51 *** |
|
| ||
| SM coping | ||
| LBC confront homophobia | 1 | .67 *** |
| LBC self-acceptance | .82 (.07) | .54 *** |
| LBC spirituality | .46 (.06) | .32 *** |
| LBC online support | 1.05 (.09) | .55 *** |
|
| ||
| Psychological distress | ||
| Depression | 1 | .94 *** |
| Anxiety | .52 (.02) | .80*** |
Note. N = 1,099. χ2 (118) = 681.6, p < .001, CFI=.94, TLI=.92, SRMR=.05, and RMSEA=.06. BC = Brief cope. SM = Sexual minority-specific. LBC= Lesbian bisexual coping.
p < .001.
Structural Model
The structural model consists of all hypothesized relationships (i.e. causal, correlational) among study constructs represented in any given tested model. The hypothesized model (Figure 2) demonstrated close to acceptable fit (χ2 (143) = 806.8, p <.001, CFI=.89, TLI=.88, SRMR=.08, and RMSEA=.07). A close inspection of the model revealed that the adaptive coping factor did not add significantly to the model. Therefore, we removed adaptive coping and re-estimated the model. The new model (Figure 3) demonstrated acceptable fit, χ2 (83) = 402.9, p <.001, CFI=.94, TLI=.92, SRMR= .07, and RMSEA=.06. This model accounted for 73% of variance in the psychological distress factor.
Figure 2.
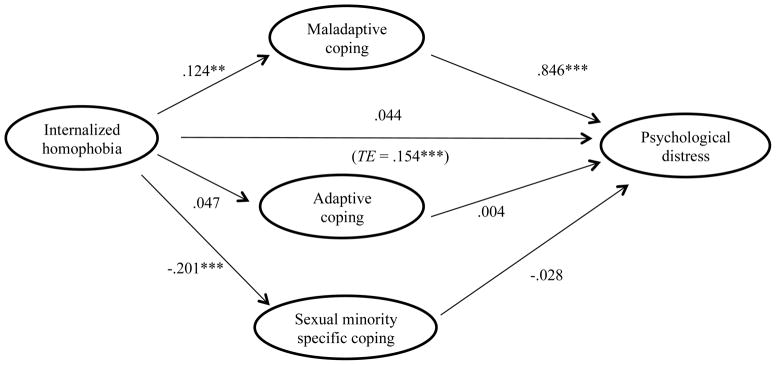
Structural Model and Standardized Path Coefficients
Note: * p < .05. ** p < .01. *** p < .001.
TE refers to the Total Effect
Figure 3.

Re-estimated Structural Model and Standardized Path Coefficients
* p < .05. ** p < .01. *** p < .001.
TE refers to the Total Effect
Direct Effects
Direct effects represents direct relationships between independent and dependent variables above and beyond the effects of other specified variables. Sexual minority women with higher levels of internalized homophobia reported higher levels of maladaptive coping (β = .12, p = .002) and lower levels of sexual minority-specific coping (β = −.21, p < .001). In turn, higher levels of maladaptive coping were associated with higher levels of psychological distress (β = .85, p < .001), but no statistically significant association was observed between sexual minority-specific coping and psychological distress (β = −.03, p = .41). Further, there was no statistically significant direct effect of internalized homophobia on psychological distress above and beyond the coping variables (β = .04, p = .12).
Indirect Effects
There was a statistically significant total effect of internalized homophobia on psychological distress prior to inclusion of mediators (β = .15; 95% CI: .08, .22; p < .001). The total effect refers to the sum of the direct and indirect effects of internalized homophobia on psychological distress; and it can also be considered the effect of internalized homophobia prior to inclusion of mediators. An indirect effect represents mediation (i.e., intervening third variable) that explains the direct relationship between independent and dependent variables. Indirect effects here represent the effect of internalized homophobia on psychological distress that occurs through the coping variables. As indicated in Table 3, we observed a statistically significant indirect effect of internalized homophobia on psychological distress through maladaptive coping such that maladaptive coping fully mediated the relationship between internalized homophobia and psychological distress (indirect effect β = .11; 95% CI: = .04, .17; p = .002). However, sexual minority-specific coping did not mediate the relationship between internalized homophobia and psychological distress (indirect effect β = .005; 95% CI: −.01, .02; p = .43).
Table 3.
Indirect Effects of Internalized Homophobia via Coping Measures on Psychological Distress.
| Indirect Pathway | Indirect effect | 95% CI | p-value |
|---|---|---|---|
| Effects from internalized homophobia to psychological distress | |||
| Via sexual minority-specific coping | 0.005 | −.008, .019 | .43 |
| Via maladaptive coping | 0.100 | . 038, .171 | .002 |
Discussion
Mental health disparities between sexual minority and heterosexual women have been well documented in the literature (Bostwick et al., 2010; Hughes et al., 2010; King et al., 2008; Meyer, 2003), with observed disparities in both mental health disorders as well as general psychological distress. In the current study, we focused on examining psychological distress among young sexual minority women, as this construct has been examined in numerous epidemiologic studies and applies broadly to clinical and non-clinical populations (Cox et al., 2002; Kessler et al., 1994; Krueger, 1999). Our objective was to evaluate both general coping and sexual minority-specific coping as mediators between internalized homophobia and psychological distress. The proposed model predicted a large proportion of the variance in depression and anxiety among lesbian and bisexual women. As hypothesized, internalized homophobia was related to psychological distress directly (Newcomb & Mustanski, 2010) and indirectly through maladaptive coping. Maladaptive coping appeared to be more of a contributor to depression and anxiety than either adaptive coping or sexual minority-specific coping strategies (Szymanski & Owens, 2008). To our knowledge, our study is the first attempt to test both general and sexual minority-specific coping strategies as mediators. Doing so allowed for direct comparison of these different constructs among a national sample of young lesbian and bisexual women.
Our findings support the association between internalized homophobia and psychological distress. Consistent with extant literature, sexual minority women with higher levels of internalized homophobia reported experiencing more psychological distress (Newcomb & Mustanski, 2010). Indeed, there is a growing body of literature suggesting experiences of discrimination and negative societal messages may contribute to higher levels of psychological distress among sexual minority women through internalized cognitions about self. This suggests that therapies may be beneficial in addressing depression and anxiety in this population through providing corrective feedback that is incongruent with these negative beliefs about self and others (Kaysen, Lostutter, & Goines, 2005; Pachankis & Goldfried, 2004; Pachankis, 2008). As an example, cognitive behavioral therapies could directly utilize cognitive restructuring strategies to address internalized homophobia as examples of maladaptive cognitions.
Internalized homophobia was also associated with higher maladaptive coping and lower use of sexual minority-specific coping as predicted. These results illustrate mechanisms by which internalized negative societal messages about sexual minority women may in turn influence behaviors. It is possible that those individuals with higher internalized homophobia may then isolate more and thus be less likely to engage with the larger sexual minority community. Similarly, those with higher internalized homophobia may then be more likely to use minimization or denial in response to stressors associated with discrimination and bias rather than challenging or evaluating their beliefs (Szymanski, & Henrichs-Beck, 2013). Due to the correlational nature of this study, we cannot determine the directionality of these relationships. It is also possible that individuals who engage in more maladaptive coping strategies or who avoid involvement in the sexual minority community are less likely to encounter positive images of other sexual minority women and may therefore be less likely to change or disconfirm societal messages regarding sexual minorities. Future research should examine these relationships and how they develop and influence each other over time.
Contrary to our expectations adaptive coping was not predicted by internalized homophobia, nor did it predict psychological distress (Glass et al., 2009; Mahmoud, Staten, Hall, & Lennie, 2012; Szymanski, & Henrichs-Beck, 2013). It is possible that over reliance on maladaptive coping strategies may lead to more symptoms of psychological distress, making the use of adaptive coping less likely (Schnider, Elhai & Gray, 2007). We found that maladaptive coping in particular mediated the relationship between internalized homophobia and psychological distress such that women who used more maladaptive coping strategies reported higher levels of psychological distress. Future longitudinal studies are necessary to evaluate relationships between coping and distress. In addition, as suggested by others (Szymanski & Owens, 2008), other factors, such as community support, may be more important than adaptive coping in predicting psychological distress. We did not include measures of community involvement or social support in our model. However, given the potential importance of these factors for sexual minorities (Meyer, 2003), it would be important for future studies to investigate the relationship among these variables with coping and psychological distress
Contrary to our hypothesis, sexual minority-specific coping did not significantly mediate the relationship between internalized homophobia and psychological distress, although women reporting more internalized homophobia reported significantly less engagement in sexual minority-specific coping. It is possible that our measure of sexual minority-specific coping strategy did not fully capture the domain of positive behaviors specific to sexual minority women. However, we did find that internalized homophobia was associated with lower sexual minority-specific coping. Although this did not necessarily relate to anxiety and depression per se, this type of coping may help sexual minority women in other ways through increasing community engagement and helping build resilience within the population.
These findings also highlight the importance of considering the resilience of many sexual minority women. Many do not experience elevated depression or anxiety nor do they develop high internalized homophobia. Much of the literature to date examining minority stressors focuses on deficits rather than examining resilience within sexual minority populations (Kwon, 2013). One’s ability to be open, utilize social support, emotionally process experiences, and retain a sense of optimism all are thought to predict more resilience in the face of discrimination and stress. Consistent with this theoretical framework, our findings that sexual minority women who do not use more maladaptive strategies such as disengaging or blaming themselves for their experiences remain resilient despite minority stress. At the same time, more research is needed to understand the role of adaptive coping, which was not significantly associated with either internalized homophobia or psychological distress in our model.
Strengths of the current study include evaluation of coping in understanding the relationship between internalized homophobia and distress among sexual minority women, which has been relatively understudied (Szymanski and Owens, 2008; Szymanski, & Henrichs-Beck, 2013), as well as assessing the unique role of sexual minority-specific coping as a possible mediator. Nonetheless, longitudinal studies are necessary in order to better test mediation and assess the directionality of these relationships. Thus, although existing theory suggests that internalized homophobia suppresses adaptive coping and increases maladaptive coping, which thereby lead to psychological distress, the model would fit equally as well were the relationships reversed. Only longitudinal studies will help us better evaluate the proposed relationships. Another limitation of the present investigation is use of self-report data. There is a substantial body of research supporting the validity of self-report measures of potentially stigmatizing behavior such as substance use (Babor, Stephens, & Marlatt, 1987; Babor, Steinberg, Anton, & Del Boca, 2000; Chermack, Singer, & Beresford, 1988). In addition, although the use of the internet to attract a national sample of young women is a study strength there are also limitations associated with this method of recruitment. Participants may have concerns about confidentiality and security of data. There also can be concerns about data validity. We attempted to address this concern by obtaining phone numbers and collateral contact information from participants and evaluating key demographic variables during longitudinal data collection to remove participants with inconsistent responding. Use of the internet for recruitment also potentially limits the generalizability of our findings. Lastly, there were potential issues with our measure of sexual-minority specific coping in that the measure is new and will need further validation, more research on psychometrics, and application of the measure to other LGBT populations. Although this measure attempts to capture many of the ways in which sexual minority individuals may uniquely cope with their experiences of discrimination, it is possible it does not fully sample this behavioral domain. Future studies should include multiple measures to assess behaviors that a broad cross-section of individuals may use in response to stressors associated with their sexual orientation.
Despite these limitations, results have important clinical implications regarding possible means by which internalized homophobia may in turn affect psychological distress, both directly and through maladaptive coping. Moreover, these results have direct clinical intervention implications, suggesting that cognitive interventions directly addressing negative cognitions about self in relation to one’s sexual orientation and identity, coupled with behavioral interventions to decrease maladaptive coping strategies, may be most efficient at reducing depression and anxiety among young lesbian and bisexual women.
Acknowledgments
Data collection and manuscript preparation was supported by the National Institutes of Health, Grant R01 AA018292 awarded to D. L. Kaysen. Manuscript preparation is the result of work supported by resources from the Department of Veterans Affairs Office of Academic Affiliations, Advanced Fellowship Program in Mental Illness Research and Treatment and the VA Puget Sound Health Care System, Seattle, Washington (KL).
Footnotes
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Alcohol Abuse and Alcoholism, the National Institutes of Health, the University of Washington, or the Veterans Affairs Puget Sound Health Care System.
References
- Babor TF, Steinberg K, Anton R, Del Boca F. Talk is cheap: Measuring drinking outcomes in clinical trials. Journal of Studies on Alcohol and Drugs. 2000;61:55–63. doi: 10.15288/jsa.2000.61.55. [DOI] [PubMed] [Google Scholar]
- Babor TF, Stephens RS, Marlatt GA. Verbal report methods in clinical research on alcoholism: Response bias and its minimization. Journal of Studies on Alcohol and Drugs. 1987;48:410–424. doi: 10.15288/jsa.1987.48.410. [DOI] [PubMed] [Google Scholar]
- Bostwick WB, Boyd CJ, Hughes TL, McCabe SE. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. American Journal of Public Health. 2010;100:468–475. doi: 10.2105/AJPH.2008.152942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowleg L, Craig ML, Burkholder G. Rising and surviving: A conceptual model of active coping among Black lesbians. Cultural Diversity and Ethnic Minority Psychology. 2004;10:229–240. doi: 10.1037/1099-9809.10.3.229. [DOI] [PubMed] [Google Scholar]
- Brown LS. Feminist psychotherapies: Integration of therapeutic and feminist systems. Westport: Ablex Publishing; 1988. Feminist therapy with lesbians and gay men; pp. 206–227. [Google Scholar]
- Brown LS. Subversive dialogues: Theory in feminist therapy. New York, NY US: Basic Books; 1994. [Google Scholar]
- Carver CS. You want to measure coping but your protocol’s too long: Consider the Brief COPE. International Journal of Behavioral Medicine. 1997;4:92–100. doi: 10.1207/s15327558ijbm0401_6. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF. Situational coping and coping dispositions in a stressful transaction. Journal of Personality and Social Psychology. 1994;66:184–195. doi: 10.1037/0022-3514.66.1.184. [DOI] [PubMed] [Google Scholar]
- Carver CS, Weintraub JK, Scheier MF. Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology. 1989;56:267–283. doi: 10.1037/0022-3514.56.2.267. [DOI] [PubMed] [Google Scholar]
- Cass VC. Homosexual identity formation: A theoretical model. Journal of Homosexuality. 1979;4:219–235. doi: 10.1300/J082v04n03_01. [DOI] [PubMed] [Google Scholar]
- Chermack S, Singer K, Beresford T. Screening for alcoholism among medical inpatients: How important is corroboration of patient self-report? Alcoholism: Clinical and Experimental Research. 1988;22:1393–1398. doi: 10.1111/j.1530-0277.1998.tb03925.x. [DOI] [PubMed] [Google Scholar]
- Chung YB, Williams W, Dispenza F. Validating work discrimination and coping strategy models for sexual minorities. Career Development Quarterly. 2009;58:162–170. doi: 10.1002/j.2161-0045.2009.tb00053.x. [DOI] [Google Scholar]
- Cox BJ, Clara IP, Enns MW. Posttraumatic stress disorder and structure of common mental disorders. Depression and Anxiety. 2002;15:168–171. doi: 10.1002/da.10052. [DOI] [PubMed] [Google Scholar]
- Czech EA, Waidzunas TJ. Navigating the heteronormativity of engineering: The experiences of lesbian, gay and bisexual students. Engineering Studies. 2011;3:1–24. doi: 10.1080/19378629.2010.545065. [DOI] [Google Scholar]
- David S, Knight BG. Stress and coping among gay men: Age and ethnic differences. Psychology and Aging. 2008;23:62–69. doi: 10.1037/0882-7974.23.1.62. [DOI] [PubMed] [Google Scholar]
- Fleishman JA, Fogel B. Coping and depressive symptoms among young people with AIDS. Health Psychology. 1994;13:156–169. doi: 10.1037/0278-6133.13.2.156. [DOI] [PubMed] [Google Scholar]
- Folkman S, Lazarus RS. An analysis of coping in a middle-aged community sample. Journal of Health and Social Behavior. 1980;21:219–239. [PubMed] [Google Scholar]
- Folkman S, Lazarus RS. If it changes it must be a process: Study of emotion and coping during three stages of a college examination. Journal of Personality and Social Psychololgy. 1985;48:150–170. doi: 10.1037//0022-3514.48.1.150. [DOI] [PubMed] [Google Scholar]
- Glass K, Flory K, Hankin BL, Kloos B, Turecki G. Are coping strategies, social support, and hope associated with psychological distress among hurricane Katrina survivors? Journal of Social and Clinical Psychology. 2009;28:779–795. doi: 10.1521/jscp.2009.28.6.779. [DOI] [Google Scholar]
- Gonsiorek JC. Homosexual issues in the workplace. Washington, DC US: Taylor & Francis; 1993. Threat, stress, and adjustment: Mental health and the workplace for gay and lesbian individual; p. 243. [Google Scholar]
- Hatzenbuehler ML, Corbin WR, Fromme K. Discrimination and alcohol-related problems among college students: A prospective examination of mediating effects. Drug and Alcohol Dependence. 2011;115:213–220. doi: 10.1016/j.drugalcdep.2010.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatzenbuehler ML, Nolen-Hoeksema S, Erickson S. Minority stress predictors of HIV risk behavior, substance use, and depressive symptoms: Results from a prospective study of bereaved gay men. Health Psychology. 2008;27:455–462. doi: 10.1037/0278-6133.27.4.455. [DOI] [PubMed] [Google Scholar]
- Herek GM, Garnets LD. Sexual orientation and mental health. Annual Review of Clinical Psychology. 2007;3:353–375. doi: 10.1146/annurev.clinpsy.3.022806.091510. [DOI] [PubMed] [Google Scholar]
- Holahan CJ, Holahan CK, Moos RH, Brennan PL, Schutte KK. Stress generation, avoidance coping, and depressive symptoms: A 10-Year model. Journal of Consulting and Clinical Psychology. 2005;73:658–666. doi: 10.1037/0022-006X.73.4.658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structural analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Hughes TL, Szalacha LA, McNair R. Substance abuse and mental health disparities: Comparisons across sexual identity groups in a national sample of young Australian women. Social Science and Medicine. 2010;71:824–831. doi: 10.1016/j.socscimed.2010.05.009. [DOI] [PubMed] [Google Scholar]
- Kaysen D, Lostutter TW, Goines MA. Cognitive processing therapy for acute stress disorder resulting from an anti-gay assault. Cognitive and Behavioral Practice. 2005;12:278–289. doi: 10.1016/s1077-7229(05)80050-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, McGongle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R, psychiatric disorders in the United States. Results from the National Comorbidity Surve. Archives of General Psychiatry. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- Kessler R, DuPont R, Berglund P, Wittchen H. Impairment in pure and comorbid generalized anxiety disorder and major depression at 12 months in two national surveys. American Journal of Psychiatry. 1999;156:1915–1923. doi: 10.1176/ajp.156.12.1915. [DOI] [PubMed] [Google Scholar]
- King M, Semlyen J, Tai SS, Killaspy H, Osborn D, Popelyuk D, Nazarteh I. A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay and bisexual people. BMC Psychiatry. 2008;8:70. doi: 10.1186/1471-244X-8-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohn P. Handbook of coping: Theory, research, applications. Oxford: John Wiley & Sons; 1996. On coping adaptively with daily hassles; pp. 181–201. [Google Scholar]
- Krueger RF. The structure of common mental disorders. Archives of General Psychiatry. 1999;56:921–926. doi: 10.1001/archpsyc.56.10.921. [DOI] [PubMed] [Google Scholar]
- Kwon P. Resilience in Lesbian, Gay, and Bisexual Individuals. Personality and Social Psychology Review. 2013;17(4):371–383. doi: 10.1177/1088868313490248. [DOI] [PubMed] [Google Scholar]
- Lazarus RS, Folkman S. Stress, appraisal, and coping. New York, NY US: Springer; 1984. [Google Scholar]
- Lehavot K. Coping strategies and health in a national sample of sexual minority women. American Journal of Orthopsychiatry. 2012;82:494–504. doi: 10.1111/j.1939-0025.2012.01178.x. [DOI] [PubMed] [Google Scholar]
- Lehavot K, Simoni JM. The impact of minority stress on mental health and substance use among sexual minority women. Journal of Consulting and Clinical Psychology. 2011;79:159–170. doi: 10.1037/a0022839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahmoud JS, Staten RT, Hall LA, Lennie TA. The relationship among young adult college students’ depression, anxiety, stress, demographics, life satisfaction, and coping styles. Issues in Mental Health Nursing. 2012;33:149–156. doi: 10.3109/01612840.2011.632708. [DOI] [PubMed] [Google Scholar]
- Martell CR, Safren SA, Prince SE. Cognitive-behavioral therapies with lesbian, gay, and bisexual clients. New York, NY US: Guilford Press; 2004. [Google Scholar]
- Meyer IH. Minority stress and mental health in gay men. Journal of Health and Social Behavior. 1995;36:38–56. [PubMed] [Google Scholar]
- Meyer IH. Prejudice, social stress and mental health in lesbian, gay and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin. 2003;129:674–697. doi: 10.1037/0033-2909.129.5.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH, Dean L. Stigma and sexual orientation: Understanding prejudice against lesbians, gay men, and bisexuals. Thousand Oaks: Sage; 1998. Internalized homophobia, intimacy, and sexual behavior among gay and bisexual men; pp. 160–186. [Google Scholar]
- Mohr JJ, Kendra MS. Revision and extension of a multidimensional measure of sexual minority identity: The Lesbian, Gay, and Bisexual Identity Scale. Journal of Counseling Psychology. 2011;58:234–245. doi: 10.1037/a0022858. [DOI] [PubMed] [Google Scholar]
- Mohr J, Fassinger R. Measuring dimensions of lesbian and gay male experience. Measurement and Evaluation in Counseling Development. 2000;33:66–90. [Google Scholar]
- Molina Y, Balsam KF, Beadnell B. Coping, minority stress, and mental health among ethnically diverse LGBT adults. National Multicultural Conference & Summit; Seattle, WA. 2011. [Google Scholar]
- Newcomb ME, Mustanski B. Internalized homophobia and internalizing mental health problems: A meta-analytic review. Clinical Psychology Review. 2010;30:1019–1029. doi: 10.1016/j.cpr.2010.07.003. [DOI] [PubMed] [Google Scholar]
- Nicholson WD, Long BC. Self-esteem, social support, internalized homophobia, and coping strategies of HIV+ gay men. Journal of Consulting and Clinical Psychology. 1990;58:873–876. doi: 10.1037//0022-006x.58.6.873. [DOI] [PubMed] [Google Scholar]
- Pachankis JE. Disclosing gay-related stress: Psychological and physical health effects and mechanisms underlying improvement. Stony Brook: Graduate School at Stony Brook University; 2008. [Google Scholar]
- Pachankis JE, Goldfried MR. Clinical issues in working with lesbian, gay, and bisexual clients. Psychotherapy: Theory, Research, Practice, and Training. 2004;41:227. doi: 10.1037/0033-3204.41.3.227. [DOI] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- Roderick T, McCammon SL, Long TE, Allred LJ. Behavioral aspects of homonegativity. Journal of Homosexuality. 1998;36:79–88. doi: 10.1300/J082v36n01_05. [DOI] [PubMed] [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. doi: 10.1037/1082-989X.7.2.147. [DOI] [PubMed] [Google Scholar]
- Schindler KR, Elhai JD, Gray MJ. Coping style use predicts posttraumatic stress and complicated grief symptom severity among college students reporting a traumatic loss. Journal of Counseling Psychology. 2007;54:344–350. doi: 10.1037/0022-0167.54.3.344. [DOI] [Google Scholar]
- Schmitz MF, Crystal S. Social relations, coping, and psychological distress among persons with HIV/AIDS. Journal of Applied Social Psychology. 2000;30:665–683. doi: 10.1111/j.1559-1816.2000.tb02818.x. [DOI] [Google Scholar]
- Sophie J. Internalized homophobia and lesbian identity. Journal of Homosexuality. 1987;14:53–65. doi: 10.1300/J082v14n01_05. [DOI] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JW, Löwe B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine. 2006;166:1092–1097. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- Steele LS, Ross LE, Dobinson C, Veldhuizen S, Tinmouth JM. Women’s sexual orientation and health: Results from a Canadian population-based survey. Womens Health. 2009;49:353–367. doi: 10.1080/03630240903238685. [DOI] [PubMed] [Google Scholar]
- Swinson RP. The GAD-7 scale was accurate for diagnosing generalized anxiety disorder. Evidence Based Medicine. 2006;11:184. doi: 10.1136/ebm.11.6.184. [DOI] [PubMed] [Google Scholar]
- Szymanski D. Examining potential moderators of the link between heterosexist events and gay and bisexual men’s psychological distress. Journal of Counseling Psychology. 2009;56:142–151. doi: 10.1037/0022-0167.56.1.142. [DOI] [Google Scholar]
- Szymanski DM. Heterosexism and sexism as correlates of psychological distress in lesbians. Journal of Counseling Development. 2005;83:355–360. doi: 10.1002/j.1556-6678.2005.tb00355.x. [DOI] [Google Scholar]
- Szymanski DM, Carr ER. The roles of gender role conflict and internalized heterosexism in gay and bisexual men’s psychological distress: Testing two mediation models. Psychology of Men and Masculinity. 2008;9:40–54. doi: 10.1037/1524-9220.9.1.40. [DOI] [Google Scholar]
- Szymanski DM, Henrichs-Beck C. Exploring Sexual Minority Women’s Experiences of External and Internalized Heterosexism and Sexism and their Links to Coping and Distress. Sex Roles. 2013:1–15. [Google Scholar]
- Szymanski DM, Kashubeck-West S, Meyer J. Internalized heterosexism:Measurement, psychosocial correlates, and research directions. Counseling Psychologist. 2008a;36:525–574. [Google Scholar]
- Szymanski DM, Kashubeck-West S, Meyer J. Internalized heterosexism: A historical and theoretical overview. Counseling Psychologist. 2008b;36:510–524. doi: 10.1177/0011000007309488. [DOI] [Google Scholar]
- Szymanski DM, Owens GP. Do coping styles moderate or mediate the relationship between internalized heterosexism and sexual minority women’s psychological distress? Psychology Womens Quarterly. 2008;32:95–104. [Google Scholar]
- Talley AE, Bettencourt BA. The moderator roles of coping style and identity disclosure in the relationship between perceived sexual stigma and psychological distress. Journal of Applied Social Psychology. 2011;41:2883–2903. doi: 10.1111/j.1559-1816.2011.00863.x. [DOI] [Google Scholar]
- Tucker-Seeley RD, Blow AJ, Matsuo H, Taylor-Moore R. Behavioral Escape Avoidance Coping in African-American Men Who Have Sex with Men. Journal of Gay & Lesbian Social Services. 2010;22(3):250–268. [Google Scholar]
- Wagner G, Brondolo E, Rabkin J. Internalized homophobia in a sample of HIV+ gay men, and its relationship to psychological distress, coping, and illness progression. Journal of Homosexuality. 1996;32:91–106. doi: 10.1300/J082v32n02_06. [DOI] [PubMed] [Google Scholar]
- Yi H, Sandfort TG, Shidlo A. Effects of disengagement coping with HIV risk on unprotected sex among HIV-negative gay men in New York City. Health Psychology. 2010;29(2):205. doi: 10.1037/a0017786. [DOI] [PMC free article] [PubMed] [Google Scholar]