

Abstract
Background
Little is known about how investigators approach their research programs along the translational research continuum. Many consider the translational continuum to be linear, with research beginning at the bench and concluding with research at the bedside or in the community. We aimed to understand if translational investigators approach and view their research in this fashion.
Methods
We conducted semistructured individual interviews with 16 graduates of the University of Pittsburgh's Multidisciplinary Clinical Research Scholars Program (KL2) in 2012.
Results
Our research revealed three characteristic models. The first model we called “linear” and represented the traditional approach. The second we called “holistic”; these investigators began with central research questions and sought to explore them in every direction of translation, not necessarily taking linear steps. The third model we called “technical”; in this model, investigators focused on a unique technology or methodology and applied it across multiple research contexts.
Conclusion
This study found that there are multiple ways that translational investigators approach their research program. Better understanding of these models can help educators and mentors guide investigators so that they can be more productive in their clinical or translational research career.
Keywords: translational research models, bench to bedside, translational continuum, CTSA, KL2 Scholars Program
Introduction
Prior research emphasizes translational science as a continuum that begins with basic biomedical research, progresses to human studies, and ends with practice.1 Trochim et al. reviewed four of these models and concluded that all of the models represent translational research as “a temporal process” that starts with basic science and moves through clinical research to practice.2 The study further explains that the models are bidirectional and that research can move forward or backward along the translational continuum from basic to clinical and back to basic before it moves back to clinical and then to practice. For example, a discovery made during basic research may move to pilot testing in animal models and eventually testing in humans. If a component of the testing in humans is unsuccessful, the research may revert to basic or animal models for further testing and development. As Trochim et al. note, the objective is to move research along the translational continuum, from basic or bench research to practice.2
Using a very different approach, Rubio et al. characterized the model of translational research as a circular process.3 This more dynamic model suggests that translational research is composed of a continuous cycle in which research moves across any phase of the spectrum and does not follow a linear path.
Implications for the models of translation are important. Several issues have been raised regarding how we train the next generation of researchers; for example, what skills are needed3 or how we can remove the barriers to translation1 to help speed up discovery and bring new knowledge into practice. Other concerns center around how we evaluate the translational research process so that we can shorten the length of time for research to progress from discovery to patient care.2 However, we do not yet know how individual investigators approach their research programs with regard to the translational continuum. Do they translate their research in a linear fashion? Are there other approaches that investigators follow in their research careers?
To gain a better understanding of the approaches to translational research, we conducted a qualitative study of graduates of the KL2 career development program of the Clinical and Translational Science Institute at the University of Pittsburgh. We interviewed former scholars to better understand the trajectories of their research pathways and how they pursue their translational research.
Methods
Participants and setting
Participants were alumni of the University of Pittsburgh's Multidisciplinary Clinical Research Scholars Program, which is part of the Research Education and Career Development key function of the Clinical and Translational Science Institute (CTSI), funded by NIH's Clinical and Translational Science Award (CTSA), KL2 mechanism. The KL2 is similar to an NIH K12 in that it is a highly competitive career development award given to the institution, focusing on clinical and translational research. Applicants submit a grant proposal, similar to that required for an NIH K award. Proposals are reviewed similar to an NIH study section by a multidisciplinary advisory committee. The success rate for applications is 17%.
At the time of the study, we had 20 active scholars and 30 alumni. We fund scholars for up to 5 years, covering 75% of their salary so that they have protected time to conduct research and acquire training needed to develop their careers. In addition, each scholar is given start‐up funding and support (e.g., biostatistical help, editorial assistance, and advising) for their research.
Using purposive sampling, we selected former scholars based on their career stage. We wanted scholars who were more advanced in their careers, as opposed to scholars who were still on a K award. Our goal was to interview scholars who had moved out of training, but were still relatively junior in their research careers, which would enable them to recall each research project in which they have been involved. Of the 30 alumni, three were still on a K award and were not eligible. We were not able to locate contact information for two alumni, leaving 25 as our sampling pool. We initially approached 18 alumni scholars for participation; one did not respond, and one canceled our meeting prior to his interview. Therefore, we conducted interviews with the remaining 16 scholars. Of the 16 interviewees, all but one were still employed at the University of Pittsburgh, enabling us to conduct interviews in person with 15 participants; we interviewed the scholar who had changed institutions by telephone. We planned on interviewing the remaining seven eligible alumni, but did not because we had reached thematic saturation.
Data collection
We were primarily interested in learning how emerging investigators approached their research programs with regard to the translational continuum. We also wanted to understand fully the factors that motivated scholars to take different approaches. Qualitative methods allow researchers to ask about motivations and experiences that require respondents to engage in reflection and explanation, rather than short, structured answers.4 Because we anticipated scholars each having unique approaches, depending on their research questions, we used individual semistructured interviews so that scholars could tell the “story” of their approach to conducting their research. We thus used a narrative approach to qualitative research, inviting scholars to articulate the relationship between events, subsequent actions, and reasoning, making their thought processes visible.5
We, therefore, prepared semistructured interview questions and prompts that asked participants to describe all of their research projects since they entered the KL2 program. We included questions about obstacles or facilitators to moving between different points on the translational continuum, and we inquired about future research plans. To assess whether their research has had a ripple effect in their field—stimulating translational work without conducting it themselves—we included a question that probed for information about other investigators who might have expanded upon their work. As we developed the interview questions, we anticipated discerning from the data that scholars moved along the continuum, linearly.
Using standardized definitions established by the University of Pittsburgh's CTSA for each phase of translational research, we also developed a linear continuum of translational research on which participants could locate each of their projects. We defined translational research as comprising five components: basic research, T1, clinical research, T2, and practice (Figure 1 ). Since the interview questions were few, and relatively simple (“Once your current work is complete, what is your next step for its advancement?”), the interview questions were piloted with one alumni scholar and revised accordingly.
Figure 1.
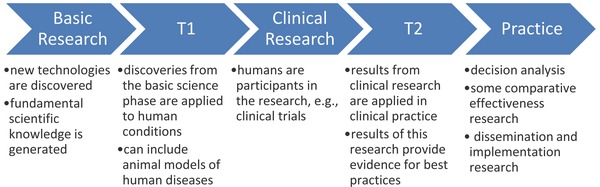
Translational research continuum.
We sent the interview questions, the linear model, and the standardized definitions to participants in advance of the interview. Interviews were semistructured and scholars were free to introduce topics or points of their own. Interviews were recorded and transcribed verbatim. Two interviewers (DR, VG) were present; one conversed with the participant while the other took notes. One interviewer (DR) is a co‐director of the KL2 program and serves as an advisor to the scholars. We conducted interviews between April and August, 2012. The main principle guiding determination of sample size in qualitative research is “thematic saturation,” a process by which a researcher collects and analyzes data until he or she is not learning anything new.6 We noted thematic saturation or redundancy at 16 interviews and, therefore, stopped data collection.
Given the ongoing research evaluation efforts of the University of Pittsburgh CTSA, we solicit University of Pittsburgh IRB‐approved informed consent from the scholars for concurrent and future potential participation in research related to their educational programs as they enter the KL2 program. Prior to the interviews, we reminded scholars of this previously signed informed consent, asked for verbal recommitment to participate in the interview, and for permission to record the current interview.
Data analysis
Interview transcripts were coded by one member of the research team (GR) using ATLAS.ti V. 6.2 (Berlin, Germany). This member has interacted with some of the scholars but has not served in a mentoring or leadership capacity in the KL2 program. While computer‐assisted qualitative data analysis software (CAQDAS) can help the researcher elicit a theory from the data more efficiently,4 it does not create the theory itself.5, 6 We created codes deductively, based on our interview questions, and added inductive codes as themes emerged. We used memoranda to maintain records of developing patterns and models and to describe refinements to our codes.
During data analysis, clear, but unexpected, broad themes emerged, suggesting the emergence of three fundamentally different ways to approach one's research. Therefore, after each interview had been coded in detail, we reviewed each transcript looking for participants' broader descriptions of their approach to their research. This approach yielded the models we report here. Rather than using multiple coders to ascertain intercoder reliability of the transcripts,7 we opted to use a team approach for reviewing the codes and delineating the appropriate model for each participant. We considered the model to be appropriately assigned to the participant if team members all agreed, with minimal discussion, on the model.
Qualitative researchers tend to use words such as “credibility,” “trustworthiness,” and “consistency,”8, 9, 10 rather than “validity,” to represent a good correspondence between reality and the perspectives of participants. One method of corroborating qualitative findings is “member checking” or the process of reviewing the interpretive results with project participants.6 Having devised and refined our models based on the data, we sent the participants templates that represented the three models. We asked them which model they felt best fit their research program without informing them of our categorization of their research. When scholars required clarification, we sent them our depiction of their research in one or two of the models and asked them to choose which model better reflected their approach to their research.
Results
Sample
Nine of the 16 participants (56%) were male and two were underrepresented minorities (12.5%). Six scholars (38%) either had a PhD or ScD. Of the remaining 10 (62%), all but one of the MDs had either completed a PhD or Master's degree. All of the alumni scholars were actively engaged in clinical and translational research, as evidenced by the fact that they averaged 41 publications each (662 total publications) and had secured an average of 13 grants per person (212 total grants for the 16 scholars). All of the participants had either completed the KL2 after five years (n = 6) or left the program early, having secured additional funding (n = 9), with the exception of the one who had relocated to another university.
Translational models
During the analyses, three distinct approaches to research emerged, which we characterized as “linear,” “holistic,” or “technical.” Here, we describe the models and provide quotes from participants that reinforce the design of the models and demonstrate how their research fits into a particular one.
Linear model
The first model (Figure 2 ) is the one we had originally hypothesized and showed to participants. It depicts a linear path of bench research eventually being translated across the continuum to patients' bedside and into the community. Research can move in either direction and sometimes skip a translational component; however, the process remains linear, and researchers take a stepwise approach in planning the course of their various research projects as they progress to the bedside and into the community.
Figure 2.
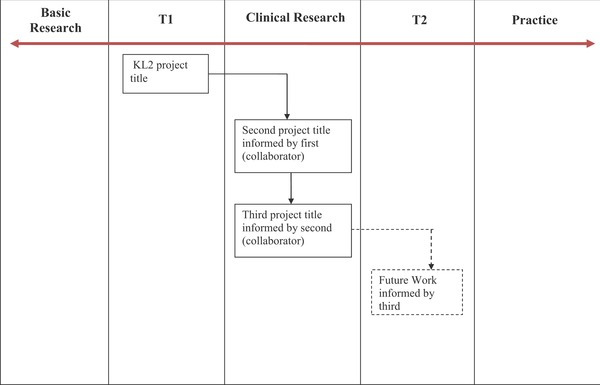
Linear model.
The majority (9 out of 16) of scholars followed this linear approach to research. Scholars in this model saw their work as progressing from basic science discovery to clinical interventions. One participant articulated the approach by saying “I've tried to approach this in a very linear fashion.” [S1]
In many instances, participants' research questions originated in their clinical practice. They either were curious about a lack of evidence for a human condition or saw the need to develop a new system or treatment to improve clinical practice. The scholar would then work backwards on the continuum to develop an intervention and then move forward on the continuum to test and incorporate the intervention in practice:
I originally started with a T2 research model, which was largely necessary because it was difficult for me to actually do the T1 and clinical research without building a clinical platform upon which to do it. So the first step for us was building a clinical model … that got us access to this patient group … and got all of the patients on the same kind of clinical care model. … And so we published on that, describing how we implemented best practices in our local facility and improved outcomes. … After that was set up, it provided us with a platform to be able to do the T1 research and clinical research. [S13]
A few scholars in this category displayed adherence to this overall model but had not yet showed movement along the continuum. These scholars were developing evidence in a particular area of the continuum before progressing across it. Some of these scholars showed signs of “stretching” their research across the boundaries between their research's current position on the continuum and another place on the continuum. For example, clinical trialists might “stretch” into T1 by developing a pilot project to help inform their area of study. We classified these scholars as linear because they conceptualized their future research as progressing linearly.
Holistic model
The holistic model (Figure 3 ) differed from the linear model. Rather than plotting a series of steps along a linear path, the four scholars representing this model were driven by a focused desire to address a specific health problem or issue. As one participant said, “If it sounds like I'm on a mission, part of it is a mission because you really want to help people.” [S14]. This same participant rationalized the need for studies in different fields that may otherwise appear unrelated because they had the potential to help her target population. She was driven to pursue this range of studies because “it's near to my heart.”
Figure 3.
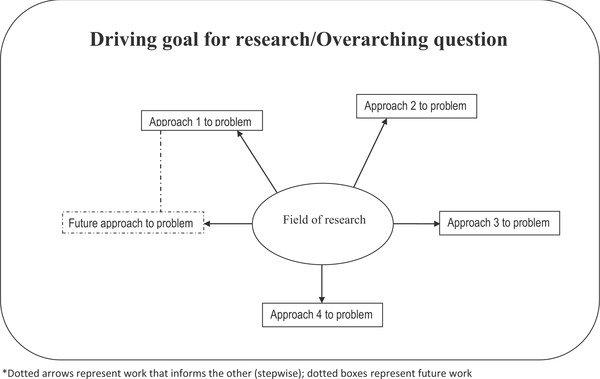
Holistic model.
Scholars taking the holistic approach to their research (4 out of 16) had a broad but distinct research area and tried to understand the problem from a variety of perspectives. They sought whatever path was necessary to generate evidence to answer their overarching research question. As one alumni scholar stated:
I think my strength lies at being able to deeply appreciate and sometimes investigate mechanisms of things and then be able to find good ways to apply efficacious therapies to large groups of people. … I really like, and I think need as a researcher, the ability to cross those … columns [referring to the different types of research on the linear model]. I've been trying to find ways to remain cognitively broad enough that I can see a problem… or see a really big picture item like how do our individual traits which are formed at birth and influenced over the first 2–3 decades of our life influence our health, our physical health, and aging over our lifespan. That's a big picture question and it's impossible to focus permanently, but what I've done is focus through my grants. So each grant is on one particular piece, and that's how I've done it. … That's the way I've been able to stay broad, but keep focused enough to be funded. [S7]
Participants whose research fit into the holistic model saw their work as occupying “one big bucket,” where they applied different approaches, irrespective of where those approaches fell along the translational continuum, sometimes working on multiple projects, each a different type of research, simultaneously.
These scholars tended to be more multidisciplinary, not only in how they approached their research but also within their research teams. They were often trained in various disciplines. One of the scholars who follows this approach has 10 different disciplines represented on her research team. Another scholar indicated that she has been “shifting around in many different disciplines.” [S11]
The scholars who take a holistic approach to their work appear to do so because that is the only way they can work. They naturally think of the “big picture” and are not satisfied taking an incremental approach to one part of the problem. Although they have been very successful, they have been aware of being criticized for being “spread too thin,” or lacking in focus.
Technical model
The third and final model is, again, categorically different from the other two (Figure 4 ). At the center of this model is a participant's innovative and novel approach. This may be a particular technology that the participant has developed or a special methodology in which he or she is an expert. The participant pursues his or her own research projects to use or expand this technology or methodology, but it is also in high demand by other investigators for use in their research. The scholar's research is driven by the potential for various applications of the approach.
Figure 4.
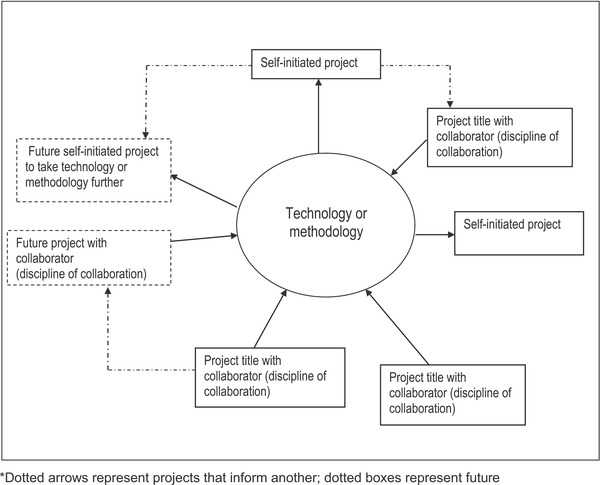
Technological model.
One scholar developed his methodology and learned how to explain its utility and potential during his KL2 award. Referring to its use in a wide variety of projects, he said, “I think that it's a powerful methodology that is a potential game changer in many areas. We're finding that as people get better acquainted with it, they tend to gravitate towards it; they see the value of it.” [S4]
Similar to the holistic model, those who follow the technical model (3 out of 16) interact with various disciplines. As one scholar put it, “We are more of a collaborator. We developed some core technology, and we help our collaborators solve the problem.” [S10] However, unlike the holistic model, the scholar does not usually initiate the collaborations. It is also a model that occupies all the types of research across the translational continuum: “This is a methodology that can [bring people together], so that acts, by definition, cross all these boundaries.” [S4]
One participant, whose technology has been showing success with collaborations in dental medicine, transplantation, and dermatology, among other fields, said, “These are the kind of things we are doing, and that's just three different directions of one arm of the basic research that stems from the original idea!” [S5]. The excitement and passion about their research was tangible as these scholars discussed the widespread potential impact for their research. One commented about his discoveries, in a manner that did not seem to be hyperbole, “I think that's really the future of medicine!” [S5]
Model validation
To validate our model selection for the scholars, we sent the scholars all three models and asked that they select the model that best fits their research program. Only 2 of the 16 (12%) participants classified their research into a different model than we had, indicating greater than 80% agreement with our selections. It is interesting to note that the academic degree of the scholars were not predictive of which model they followed.
Discussion
Most of the literature on translational research discusses the translational continuum as linear. This study found that the linear model was one pathway that investigators use to approach their research program. We found that, in addition to the linear model, our scholars used two alternative models (holistic and technical) to advance their research. The way that scholars think about their research determined the model to which each scholar adhered.
Understanding that there are more approaches to one's research beyond the linear path can have an impact on how we conceptualize and implement training. Many approaches to teaching research emphasize the linear pathway to translation. If a naturally holistic investigator is schooled in the linear approach, it may be difficult for that investigator to conceptualize his/her research trajectory. That investigator may struggle with the direction of his or her research as he/she plans the next project.
These models can inform how we mentor junior investigators. If an investigator follows a linear model, then having a mentor who understands the translational continuum as well as the common translational roadblocks would be critical. In contrast, if an investigator follows the holistic model, it may be important to select several mentors from different disciplines. Furthermore, it may be valuable for this individual's mentoring team to meet with enough regularity to understand and appreciate the investigator's multiple projects and their relationship to each other. Mentors of investigators who align with the technical model may be able to provide important guidance on the balance of collaborative projects with investigator‐led projects to satisfy institutional promotion and tenure expectations.
If a mentor does not understand the different approaches, he or she may have unrealistic expectations of the mentee. For example, if a mentor follows a linear model and the mentee follows the holistic model, the mentee may repeatedly be told to focus. As this study found, however, not all scholars approach their research in this fashion. If mentors know and understand the approach that their mentees are taking, they can work with them to set reasonable goals. They can also share in the mentee's “bigger picture,” guiding them in a manner that will best allow them to be successful.
However, it may also be valuable for a mentor to help his/her mentee grow by discussing whether aspects of the other approaches may be valuable to consider in the mentee's work. If a young investigator tends to follow the holistic approach, for example, it may be useful for him or her to reflect whether there are linear threads to her research that may be nurtured, or whether there are certain technologies he or she has developed that may be useful to other fields. The purpose of this growth would not be to change the investigator's primary nature; it would simply be to familiarize the investigator with other models and provide opportunities for development, if appropriate. One of the best‐known analogies for this approach is the Myers‐Briggs personality type indicator (MBTI). This psychometric instrument divides individuals based on four dichotomies related to personality. An important aim of the MBTI is for individuals to pursue growth actively by nurturing in themselves the factors for which they do not test strongly.7
It is important to note that these data suggest no connection between type of research model and the investigator's success. Rather, we infer from the data that success is related more to whether the investigator's research interests and personality traits mesh with their model, than employing a particular model merely because it has allowed others to be successful. Similarly, investigators' training background in our sample was not related to their choice of model. Future quantitative studies could usefully examine whether there exists a relationship between training background, position along the clinical and translational continuum, and type of model.
One's model of how to approach research can have implications for promotion and tenure (P&T), which typically sees translational research as linear. If a P&T committee is reviewing a dossier of someone who follows the technology model, the committee might view the candidate as too diffuse or not being able to focus on a particular substantive problem. The dossier might have significant strengths with regard to other accomplishments, but lack first authored publication or grants where the person is the principal investigator.
Similarly, the National Institutes of Health (NIH) grant review system has tended to reward those who follow the traditional, linear approach. For example, those who are highly specialized in a particular area may be likely to receive high scores for their extremely well‐honed methodologies. The new NIH review and scoring system, and certain “high risk” funding mechanisms such as the New Innovator Awards, have aimed to broaden the pool of funded investigators beyond these sharply focused researchers. In either case, however, the results of this work suggest that it may be valuable to seek out and pursue funding mechanisms linked to one's research pattern to improve likelihood of success.
The three patterns of translational research we observed are likely to be a function of multiple factors, including the trainee, the mentor, institutional characteristics, and the particular field of research. For example, holistic trainees in our study seemed to have personality traits consistent with that model, such as willingness—and indeed desire—to stretch beyond usual levels of comfort. Those who are uncomfortable with this, however, may naturally adopt the linear model. A research mentor or mentoring team may also influence a trainee by consciously and/or subconsciously instilling the pattern of research with which he/she is most comfortable. Institutions can play a role by rewarding particular types of research. For example, certain organizations may offer internal competitive funding for multidisciplinary, holistic work, and others may grow technical research by developing a robust technology transfer program with financial incentives. Finally, the research topic itself may lend itself to one of the various models. For example, the study of a rare genetic disease may inherently follow the linear model—from discovery of the mutation; to development of a treatment in the laboratory; to testing of that treatment on animals and then humans. However, the study of topic such as the “influence of health literacy on health disparities” may inherently lend itself to a more holistic approach involving multiple simultaneous quantitative and qualitative studies with a highly multidisciplinary team of biological and social scientists. While it was beyond the scope of our current research to explore fully the specific factors influencing trainees' research patterns, it may be valuable for future work to do so.
Our study has several limitations. First, we interviewed scholars from only one KL2 program. However, the scholars were diverse in their training (e.g., MD, PhD, ScD) and disciplines (e.g., bioengineering, surgery, epidemiology and biostatistics, general medicine, dentistry). Second, when we embarked on the study, we assumed that all of the scholars followed the linear model, so our approach was biased in that direction. It is interesting to note, however, that despite this bias, we still found three different models for approaching one's research program. Finally, our sample size was limited and may not reflect the views of the junior faculty engaged in clinical and translational research; there may be more than the three models we found. However, we quickly reached thematic saturation for the study, which suggests validity and reliability in qualitative studies.11
Future research is needed to ascertain if there are more than three ways of approaching one's research. Research may also help determine whether investigators use a hybrid approach to their research or if they change models over time. Understanding more about the different models and how investigators approach their research may enable mentors to be better mentors.
Conclusion
This study found that there can be multiple ways to approach research, all of which can lead to productive research careers. If we understand the different approaches, we can better focus our training on what investigators need to be successful, which will vary by investigators' personality traits, research interests, and institutional home. With the pressure of getting findings from the bench to the bedside more quickly, we need to embrace the multiple models and so that we can better support junior investigators in launching their research careers.
Acknowledgments
The authors are grateful to all of the KL2 alumni scholars who gave us their time for the interview and graciously shared their perspectives on their research trajectories.
Funding/support: This research was supported by the National Institutes of Health through Grant Numbers KL2 TR000146 and UL1 TR000005.
Other disclosures: None.
Ethical approval: IRB approved
Disclaimer: The ideas expressed in this article are solely the views of the authors and do not necessarily represent the official views of the NCATS or NIH.
References
- 1. Sung NS, Crowley WF Jr, Genel M, Salber P, Sandy L, Sherwood LM, Johnson SB, Catanese V, Tilson H, Getz K, et al. Central challenges facing the national clinical research enterprise. JAMA. 2003; 289(10): 1278–1287. [DOI] [PubMed] [Google Scholar]
- 2. Trochim W, Kane C, Graham MJ, Pincus HA. Evaluating translational research: a process marker model. Clin Transl Sci. 4(3): 153–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Rubio DM, Schoenbaum EE, Lee LS, Schteingart DE, Marantz PR, Anderson KE, Platt LD, Baez A, Esposito K. Defining translational research: implications for training. Acad Med. 85(3): 470–475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lapan S, Quartaroli, ML , Riemer, FJ . Research Methods for the Social Sciences: Qualitative Research: An Introduction to Methods and Designs. Hoboken NJ: Jossey‐Bass; 2011. [Google Scholar]
- 5. Richardson L. Narrative and sociology. J Contemp Ethnogr. 1990; 19(1): 116–135. [Google Scholar]
- 6. Giacomini M, Cook DJ. Users' guides to the medical literature: XXIII. Qualitative research in health care B. What are the results and how do they help me care for my patients? Evidence‐Based Medicine Working Group. JAMA. 2000; 284(4): 478–482. [DOI] [PubMed] [Google Scholar]
- 7. Myers IB, Myers PB. Gifts Differing: Understanding Personality Type. Mountain View, CA: Davies‐Black Publishing; 1995. [Google Scholar]
- 8. Giacomini MK, Cook DJ. Users' guides to the medical literature: XXIII. Qualitative research in health care B. What are the results and how do they help me care for my patients? Evidence‐Based Medicine Working Group. JAMA. 2000; 284(4): 478–482. [DOI] [PubMed] [Google Scholar]
- 9. Mays N, Pope C. Qualitative research in health care: assessing quality in qualitative research. BMJ. 2000; 320: 50–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Serv Res. 1998; 34(5): 1189–1208. [PMC free article] [PubMed] [Google Scholar]
- 11. Morse JM, Barnett N, Mayan M, Olson K, Spiers J. Verification strategies for establishing reliability and validity in qualitative research. Int J Qual Methods. 2002; 1(2): 13–22. http://ejournals.library.ualberta.ca/index.php/IJQM/article/view/4603/3756. Accessed September 27, 2013. [Google Scholar]