

Abstract
Aim:
To evaluate effect on intraocular pressure (IOP) during sub-Tenon's local anesthesia (LA) during cataract surgery with 4 ml of anesthetic injected without and with addition of hyluronidase to anesthetic solution.
Materials and Methods:
This randomized controlled study included 65 eyes of 65 patients undergoing phacoemulsification and lens implant for cataract. The patients were randomized to a standardized procedure of administration of 4 ml of sub-Tenon's LA without and with addition of 15 IU/ml hylaluronidase to 2% lidocaine (control group and intervention group respectively). IOP measurements were carried out immediately prior to and at 2, 5, and 10 and 15 min after sub-Tenon's injection using a hand held tonometer (Tonopen).
Results:
All patients achieved satisfactory akinesia and complete analgesia during surgery. The mean age of patients in control group was 59.56 ± 14.3 years, and 61.77 ± 11.91 years in intervention group (P = 0.507). The mean preinjection and 15 min IOP was 19.16 ± 4.39 and 20.21 ± 5.49 mm Hg, respectively in control group (P = 0.220); and 19.81 ± 3.8 and 19.68 ± 5.19 mmHg respectively in intervention group (P = 0.911). No statistical difference from baseline was detected between preinjection and at 2, 5, 10, and 15 min after injection in control (P = 0.124, 0.310, 0.804, 0.220, respectively) and intervention group (P = 0.367, 0.879, 0.765, 0.911 respectively).
Conclusion:
No significant rise in IOP occurs following injection of sub-Tenon's LA, when up to 4 ml of anesthetic is injected. The addition of hyaluronidase to 2% lignocaine has no beneficial lowering effect on IOP in sub-Tenon's LA. Hence, the practice of addition of this agent may not be necessary during cataract surgery.
Keywords: Cataract surgery, hyaluronidase, intraocular pressure, local anesthesia, Phacoemulsification, sub-Tenon's
INTRODUCTION
Various local anesthesia (LA) techniques such as retrobulbar,[1] peribulbar,[2] sub-Tenon's[3] and topical anesthesia[4] are used in cataract surgery. Following injection of LA agent, intraorbital pressure and consequently intraocular pressure (IOP) increases, depending on volume of LA agent injected into the orbital cavity.[5] An excessive local anesthetic volume may cause high IOP at the start of surgery, which can be associated with positive vitreous pressure and risk of intraoperative complications such as posterior capsule (PC) rupture, vitreous prolapse and suprachoroidal hemorrhage,[6] and it is desirable that IOP be normal or low at the commencement of surgery. Addition of hyaluronidase to anesthetic solution promotes spread of anesthetic through the tissues,[7] and may contribute to fewer rises in intraorbital pressure, quick onset of action and less positive vitreous pressure at the start of surgery.
Sub-Tenon's LA provides good analgesia and akinesia during surgery, and is becoming an increasingly popular technique for LA in cataract surgery. The rate of reported serious complications with sub-Tenon's LA compared with retrobulbar and peribulbar techniques is lower, and currently this method methods may be preferred by many surgeons for routine cataract surgery.[8] Although relatively low volume of LA agent is used in sub-Tenon's anesthesia to achieve adequate analgesia and akinesia during cataract surgery, no studies have been conducted to evaluate whether addition of hyaluronidase to anesthetic solution may be useful in its effect on IOP at the time of onset of surgery in sub-Tenon's LA. The aim of this prospective randomized study is to evaluate effect on IOP during sub-Tenon's LA during cataract surgery with 4 ml of anesthetic injected without and with addition of hyluronidase to anesthetic solution.
MATERIALS AND METHODS
Patients
This randomized controlled study included 65 eyes of 65 patients undergoing phacoemulsification and lens implant for cataract. The study was approved by institutional review board of the hospital, and informed consent was obtained. The patients were randomized to a standardized procedure of administration of 4 ml of sub-Tenon's LA without and with addition of 15 IU/ml hylaluronidase to 2% lidocaine (control group and intervention group respectively). No adrenaline was added to the anesthetic solution in either group. Eyes with glaucoma, uveitis, age <25 years, history of trauma, and previous ocular surgery were excluded from the study.
Administration of sub-Tenon's local anesthesia and intraocular pressure monitoring
One of the surgeons blinded to the type of local anesthetic solution being used, injected local anesthetic and checked IOP before and after injection. After arrival in the anesthetic induction room, intravenous access was established and monitoring of blood pressure, ECG and pulse oximeter was commenced. Topical anesthesia of conjunctiva was achieved by instillation of benoxinate 0.4% drops. An eye speculum was inserted, and conjunctiva was incised in the lower inferonasal quadrant. Dissection with a Moorefield's forceps and Westcott's scissors was carried out to gain access to the sub-Tenon space. Using a sub-Tenon cannula mounted on a 5 ml syringe, 4 ml anesthetic solution was injected into the sub-Tenon space. The speculum was removed, and with eyelids closed, gentle digital massage of orbit was carried out for 10 s to help promote spread of anesthetic through the tissues. No ocular compression or balloon was used subsequent to this maneuver. IOP measurements were carried out immediately prior to and at 2, 5, and 10 and 15 min after sub-Tenon's injection using a hand held tonometer (Tonopen).
Statistical analysis
Statistical analysis of the results was carried out with SPSS statistical software (version 13.0, professional statistics release, Chicago, USA). A t-test and was used to compare means for paired and unpaired parametric numerical data, while Chi-squared (χ²) test was used for categorical data.
RESULTS
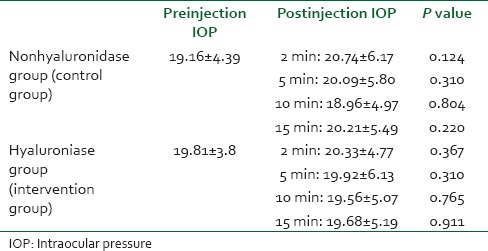
A total of 65 patients were included in this randomized study, 25 patients received sub-Tenon's LA without hyaluronidase added to the anesthetic solution (control group), while 39 patients received LA with 15 IU/ml hyaluronidase added to the anesthetic solution (intervention group). All patients achieved satisfactory akinesia and complete analgesia during surgery, and no additional anesthetic injection was required in any patient. The mean age of patients in control group was 59.56 ± 14.3 years, and 61.77 ± 11.91 years in intervention group. Table 1 shows the demographics of the patients, which shows that both groups had similar characteristics in terms of age, sex, and laterality. Table 2 shows statistical analysis of IOP between control group and intervention group, before and at 2, 5, 10 and 15 min after injection of sub-Tenon's LA. The mean preinjection and 15 min IOP was 19.16 ± 4.39 and 20.21 ± 5.49 mmHg respectively in control group; and 19.81 ± 3.8 and 19.68 ± 5.19 mmHg respectively in intervention group. There was no statistically significant difference between preinjection and postinjection IOP at 2, 5, 10 and 15 min between control and intervention groups. Table 3 shows statistical analysis of IOP within groups, and no statistical difference was detected between preinjection and at 2, 5, 10 and 15 min after injection in each group.
Table 1.
Characteristics of two groups of patients undergoing cataract surgery using sub-Tenon's LA with and without hyaluronidase added to anesthetic solution
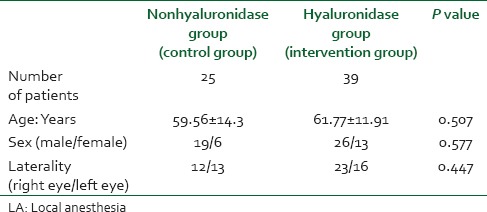
Table 2.
Statistical analysis of IOP pre and post injection between groups
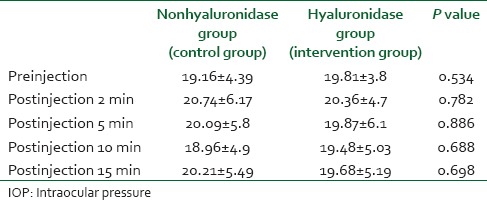
Table 3.
Statistical analysis of IOP within groups from baseline
DISCUSSION
Sub-Tenon's LA is an increasingly popular technique for LA in cataract surgery. Comparison of trends of use of various anesthesia techniques[8] for ocular surgery in the UK for the year 2002-2003 found that 42.6% surgeons preferred sub-Tenon's, 30.6% peribulbar and 20.9% topical anesthesia. The increasing popularity of the technique is due to its effectiveness and inherent safety profile, as it involves use of a blunt rather than a sharp needle, thus almost completely eliminating risk of globe perforation. The anesthesia is delivered by conjunctival dissection in a “pin point” fashion into the muscle cone, which has rapid onset of action, achieving ocular akinesia even with low volume of anesthesia.
The aim of our study were to ascertain whether sub-Tenon's LA was associated with increase of IOP following injection, and whether addition of hyaluronidase to anesthetic solution may mitigate significant rise of IOP following sub-Tenon's anesthesia in cataract surgery. When anesthetic solution is injected around the globe, the rise of IOP is related to factors such as orbital volume, size of globe, size of orbital structures and strength of orbital septum. In older people, as compared to young individuals, rise of IOP for a given volume of injected anesthetic solution is likely to be less due to age related atrophy of orbital structures and orbital septum. The results of our study suggest that a volume of 4 ml used for sub-Tenon's LA does not cause any significant rise of IOP when used alone (control group) or in combination with hyaluronidase (intervention group). In our study, it was difficult to take into account all such factors. However, both groups in our study were matched for age and sex to take account of above mentioned factors. There was no statistically significant difference between preinjection and postinjection IOP at 2, 5, 10 and 15 min between control and intervention groups. Also, there was no statistical difference in IOP within each group at 2, 5, 10 and 15 min pre and post injection.
Various studies have looked at effect of sub-Tenon's anesthesia on IOP. Alwitry et al.[9] used 5 ml unpreserved 2% lignocaine, and measured IOPs immediately prior to and at 1, 3, 5 and 10 min after injection. They found that sub-Tenon's anesthesia did not cause any significant rise in IOP. In their study Sohn et al.[10] they found that that 3-ml anesthetic volume injection was not associated with significant rise of IOP during sub-Tenon's LA for vitreoretinal surgery. However, there was a trend for larger rises in IOP with larger volumes of anesthesia. Our results are in agreement with these studies. However, we make an additional finding that, when up to 4 ml of anesthetic is injected during sub-Tenon's LA, addition of hyaluronidsase to 2% lignocaine does not have any IOP lowering effect on IOP when compared with 2% lignocaine alone.
The results of our study suggest several clinical implications. The addition of hyaluronidase to 2% lignocaine has no beneficial lowering effect on IOP in sub-Tenon's LA. Hence, the practice of addition of this agent may not be necessary during cataract surgery. Furthermore, no significant rise in IOP occurs following injection of sub-Tenon's LA, when up to 4 ml of anesthetic is injected. These points to safety of sub-Tenon's LA in reducing complications associated with high IOP at the start of surgery, such as positive vitreous pressure, PC rupture, vitreous prolapse and suprachoroidal hemorrhage.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Feibel RM. Current concepts in retrobulbar anesthesia. Surv Ophthalmol. 1985;30:102–10. doi: 10.1016/0039-6257(85)90078-5. [DOI] [PubMed] [Google Scholar]
- 2.Davis DB, 2nd, Mandel MR. Posterior peribulbar anesthesia: An alternative to retrobulbar anesthesia. J Cataract Refract Surg. 1986;12:182–4. doi: 10.1016/s0886-3350(86)80040-2. [DOI] [PubMed] [Google Scholar]
- 3.Jeganathan VS, Jeganathan VP. Sub-Tenon's anesthesia: A well tolerated and effective procedure for ophthalmic surgery. Curr Opin Ophthalmol. 2009;20:205–9. doi: 10.1097/ICU.0b013e328329b6af. [DOI] [PubMed] [Google Scholar]
- 4.Sauder G, Jonas JB. Topical versus peribulbar anesthesia for cataract surgery. Acta Ophthalmol Scand. 2003;81:596–9. doi: 10.1111/j.1395-3907.2003.00163.x. [DOI] [PubMed] [Google Scholar]
- 5.O’Donoghue E, Batterbury M, Lavy T. Effect on intraocular pressure of local anesthesia in eyes undergoing intraocular surgery. Br J Ophthalmol. 1994;78:605–7. doi: 10.1136/bjo.78.8.605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ling R, Kamalarajah S, Cole M, James C, Shaw S. Suprachoroidal haemorrhage complicating cataract surgery in the UK: A case control study of risk factors. Br J Ophthalmol. 2004;88:474–7. doi: 10.1136/bjo.2003.026179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kallio H, Paloheimo M, Maunuksela EL. Hyaluronidase as an adjuvant in bupivacaine-lidocaine mixture for retrobulbar/peribulbar block. Anesth Analg. 2000;91:934–7. doi: 10.1097/00000539-200010000-00031. [DOI] [PubMed] [Google Scholar]
- 8.Eke T, Thompson JR. Serious complications of local anesthesia for cataract surgery: A 1 year national survey in the United Kingdom. Br J Ophthalmol. 2007;91:470–5. doi: 10.1136/bjo.2006.106005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Alwitry A, Koshy Z, Browning AC, Kiel W, Holden R. The effect of sub-Tenon's anesthesia on intraocular pressure. Eye (Lond) 2001;15:733–5. doi: 10.1038/eye.2001.239. [DOI] [PubMed] [Google Scholar]
- 10.Sohn HJ, Moon HS, Nam DH, Paik HJ. Effect of volume used in sub-Tenon's anesthesia on efficacy and intraocular pressure in vitreoretinal surgery. Ophthalmologica. 2008;222:414–21. doi: 10.1159/000161556. [DOI] [PubMed] [Google Scholar]