

Abstract
Background:
Preoperative preparation (assessment) of patients reduces cancellations on the day of surgery. A Center for Reviews and Dissemination review (2007) concluded “the evidence was weak and it was uncertain that preassessment reduced cancellations.” The aim of this study was to observe the impact of a preoperative preparation clinic on cancellations of operating room cases on the day of surgery, and in particular on those causes of cancellation on the day of surgery which were expected to be affected by preoperative preparation.
Materials and Methods:
Observational study conducted in a 194 bed District General Hospital in the United Kingdom from April 1, 2006 to March 31, 2011. 42,082 operating room cases were scheduled for operation during this period. Surgical sessions which did not require anesthetic input were excluded. Contemporaneous data were collected and analyzed on a monthly basis, and also grouped by year over a 5-year period. The cancellations on the day of surgery were divided into two groups: Those considered to be affected by preoperative preparation and those which were not. Comparisons were made between these two groups and between individual reasons for cancellation.
Results:
A total of 28,928 cases met the inclusion criteria. The clinic introduction reduced cancellations considered to be affected by preoperative preparation from 462 to 177 (78% and 42% total cancellations, respectively) (P < 0.001). There was a decrease in cancellations due to patients who did not arrive (P < 0.001) and medical reasons (P < 0.001), but an increase in the number of cancellations by the patients themselves (P = 0.002). Cancellations due to lack of beds and “other” reasons both increased (P < 0.001) across the study period.
Conclusions:
This study suggests that the introduction of preoperative preparation clinics for patients reduces cancellations on the day of surgery.
Keywords: Anesthesia, assessment, cancelled procedures, preoperative care
INTRODUCTION
Preoperative assessment's raison d’être is the assessment, preparation and management of patients prior to surgery. This includes not only a physical assessment of the patient, but also a psychological preparation and information imparting/sharing, which are recognized as being equally important.[1] Preoperative preparation rather than preoperative assessment is therefore a more accurate description as the term encompasses a more holistic approach to patient care.
Preoperative preparation of patients before elective surgery has many advantages, not least reduction in patient cancellations on the day of surgery.[2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]
Cancellation of surgery on the scheduled day of surgery is inefficient for both the health service and the patient. It results in wastage of operating time through either under-utilization of operating lists or delays incurred by preparing the patients on the day of surgery;[2,4,6,7,10,11,14,15] increased costs through wastage of hospital resources;[2,4,19,22] and potential loss of earnings through time off work, as well as inconvenience and increased anxiety for the patient.[1,14,15,22]
The potential for a reduction in operating room cancellations in hospitals with no preoperative preparation clinic has been well-established.[2,6,8,10] It has been inferred that a reduction in operating room cancellations by optimizing coexisting morbidities[5,7,19,21] or by comparison to other regional hospitals[18] might be achieved in hospitals with an existing preoperative preparation unit. However, the impact on operating room cancellations during the introduction of a preoperative preparation clinic on reducing cancellations on the day of surgery for elective procedures (both inpatients and day surgery) for all the surgical specialties has been reported in only a few studies.[22]
Knox et al.[22] in 2009 demonstrated a significant reduction in cancellations for medical reasons, and a nonsignificant reduction in failure to attend and patient cancellations for all elective surgical procedures performed over a 2-year period. Other studies have demonstrated a reduction in cancellations for medical reasons for specific specialties only: Cardiac surgery;[3] general surgery;[16] and vascular surgery.[12]
A Center for Reviews and Dissemination (CRD) review in 2007 reported that “the evidence was weak and it was uncertain that preassessment reduced cancellations” on the day of surgery.[23] The CRD summary was based on a single review,[24] which was felt to be an appropriate interpretation of the evidence reviewed. However, the CRD acknowledged limitations namely only including nurse-led preassessment clinics and excluding day surgery and studies from outside the United Kingdom. The review was also limited since it was conducted by a single author who did not demonstrate any methods used to minimize reviewer bias or errors in the study selection, data extraction, or validity assessment processes. Whilst several databases were searched in the review, other relevant studies, which were not indexed within these databases could have been missed.
The current study was undertaken to describe and provide an evidence-base for the roll-out of a preoperative preparation clinic to all surgical specialties.
The aim of this study was to observe the impact of the roll-out of the preoperative preparation clinic on cancellations of operating room cases on the day of surgery, and in particular, the impact of this clinic on those causes of cancellation on the day of surgery, which were expected to be affected by preoperative preparation.
MATERIALS AND METHODS
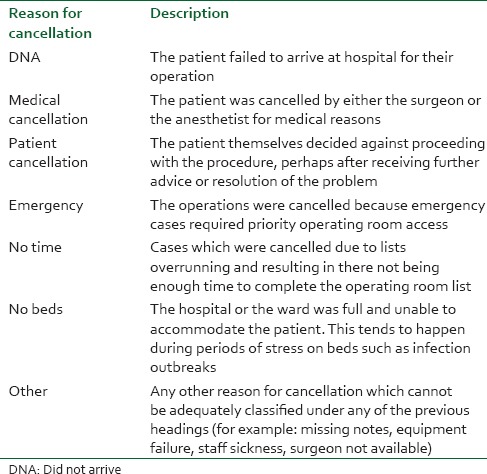
We collected contemporaneous data from monthly hospital operating room activity reports for all cases scheduled to have a surgical procedure. This data included the total number of cases going through the operating room and the number of cancellations on the day of surgery. These cancellations were made on clinical grounds by either the anesthetist/surgeon or patient and were recorded and categorized by the duty lead operating room nurse/practitioner into predefined categories [Table 1]. Patient cancellations made by telephone were received either by the admitting ward or the surgeon's secretary who would then notify the operating room reception desk who would log the reason for the cancellation.
Table 1.
Descriptions used to categorize the reason for cancellation on the day of surgery at Dr. Gray's Hospital
Individual patient records were not examined in this study because the aim was to examine the overall impact on cancellations with the introduction of a preoperative preparation service.
The categories of cancellation due to emergency intervention, lack of operating room time, lack of hospital beds, and “other” were not deemed to be affected by preoperative preparation. However, with the introduction of preoperative preparation, it is expected that the number of patients who did not arrive (DNA) for their operations, cancellations for medical reasons and cancellations by the patient themselves should decrease.
Patients listed for an operation but who did not require anesthetic input were excluded from all analyses (for example, patients undergoing endoscopic procedures, flexible cystoscopy, general practitioner (GP) minor surgical lists under local anesthesia, chronic pain procedure lists, cardiac pacing lists, and minor plastic surgical lists).
This study was conducted in a 194 bed District General Hospital in the United Kingdom. It involved four operating rooms which undertook surgical procedures covering the disciplines of orthopedics, obstetrics and gynecology, general surgery and urology, ophthalmology, maxillofacial surgery, ear, nose and throat and pediatric dental surgery.
In 2006, consultant-led preoperative preparation was only undertaken for those patients who were to undergo joint replacement orthopedic surgery. An initial unpublished audit demonstrated the potential of preoperative preparation across all surgical specialties to reduce operating room cancellations by up to 77% (n = 462/604) on the day of surgery. This preliminary data formed part of the business case to commission a dedicated preoperative preparation clinic, which involved a new build. Such a dedicated clinic was opened in August 2009.
This preoperative preparation clinic is nurse-led with clearly defined pathways to triage patients. Nurses with extensive experience on surgical wards are recruited to the preoperative assessment unit where they are trained by their peers with additional training by the consultant anesthetists. The clinic has full anesthetic support with a consultant anesthetist staffing clinics every Monday-Friday (reviewing those patients triaged to be seen by them, as well as dealing with any other problems identified by the nursing staff).
All patients in the preoperative preparation clinic are initially seen by the nurse. They complete a validated questionnaire with the patient and investigations are performed according to National Institute for Clinical Excellence guidance.[25]
All patients who are having minor surgery and are classified as American Society of Anesthesiologists (ASA) 1 or 2 are seen only by the nurse and provided with advice and information. This advice includes a verbal discussion of risks and benefits and the provision of information leaflets covering the hospital stay (generic-hospital or ward-specific dependent on the planned operation); surgery (provided by the surgeons); and possible anesthetic options (Royal College of Anesthetists patient information leaflets). Should the patients request further information they are booked to see the consultant anesthetist. There is no separate anesthetic consent in the United Kingdom at present so the surgical consent covers the anesthetic. Informed anesthetic consent was therefore not obtained in the preoperative preparation clinic.
All patients having major surgery, who are ASA 3 or higher or who have abnormal blood results or ECG must be reviewed by the consultant anesthetist in the preoperative preparation clinic. It is not feasible in our hospital for each anesthetist to assess their own cases. Therefore a “generic” preoperative assessment is conducted whereby the consultant anesthetist will assess and discuss options with the patient. They may recommend a further course of action which might include: Scheduling for surgery (with or without recommendations for actions prior to or on admission dependent on coexisting conditions), referral back to the GP, referral to other specialties (e.g., cardiac or respiratory), referral for further investigation (e.g., ECHO), or cancellation if the patient is not fit for their procedure. Any patient who after discussion of risk/benefits in preoperative preparation decides not to proceed with surgery will be removed from the waiting list at that stage and will not be booked onto an operating room list. If major anesthetic problems are anticipated the preoperative preparation anesthetist will make every effort to notify the anesthetist who will be administering the anesthetic for the patient. The consultant anesthetist undertaking the anesthesia for the case takes ultimate responsibility and must ensure that they are satisfied with the information to hand.
Data analysis
Data were analyzed on a month by month basis, and grouped by year over the 5-year study period. The financial year (beginning of April to the end of the following March) rather than calendar year was used to present the data. The cancellations on the day of surgery were divided into two major groups, those which were considered to be affected by preoperative preparation and those which were not. Data available for the time period before (40 months) and after the introduction of the preoperative clinic (20 months) were compared using the Chi-squared test. In addition, data from the last 12 months of the study (April 2010-March 2011) were compared with that from a comparable initial period of the study (April 2006-March 2007) using the Chi-squared test. Each of these major groups was then subdivided into the original categories of reasons for cancellation on the day of surgery [Table 1]. The annual data from each of these categories were compared across the 5 years of the study to determine if there were any differences within any specific categories, and to relate any such change to the introduction of the preoperative preparation service. The Chi-squared test for linear trend was used to examine trends across the 5-year period.
All analyses were performed using the Statistical Package for the Social Sciences (SPSS version 17; SPSS Inc., Chicago, IL, USA). A two-tailed P ≤ 0.05 was used throughout to denote statistical significance.
RESULTS
During the 5 years of the study 42,082 operating room cases were scheduled for operation. After excluding all surgical specialties which did not require anesthetic services, the total number included for subsequent analysis were 28,928 operating room cases. Of this study group, 2689 patients (9.3%) were cancelled on the day of surgery.
The introduction of the clinic reduced the total number of cancellations from 9.7% (n = 1771/18 288) in the 40 months (April 2006 to July 2009) prior to the clinic opening in August 2009 to 8.6% (n = 918/10,640) in the 20 months (August 2009-March 2011) after the clinics introduction (P = 0.003).
The reasons for cancellation were divided into two main groups: Those reasons which might be affected by preoperative preparation and those reasons, which would not be affected by preoperative preparation. The annual total number of cancellations on the day of surgery categorized by each group is illustrated in [Figure 1]. for the first and last years of the study. The introduction of the clinic reduced the number of cancellations, which were expected to be affected by preoperative preparation from 462 (78% of the total cancellations) in the April 2006-March 2007 period to 177 (42% of the total cancellations) in the April 2010-March 2011 period (P < 0.001).
Figure 1.
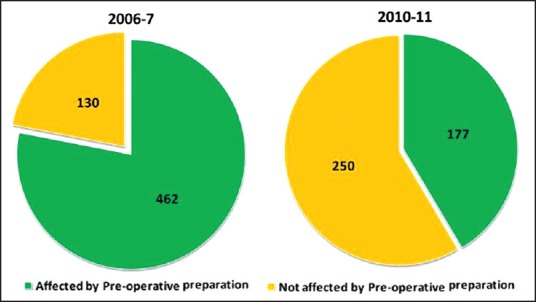
A comparison of total annual operating room cancellations between the first and last years (April-March) of the audit period. The cancellations are grouped according to reasons for cancellation which might be affected by preoperative preparation and those reasons for cancellation which should not be affected by preoperative preparation
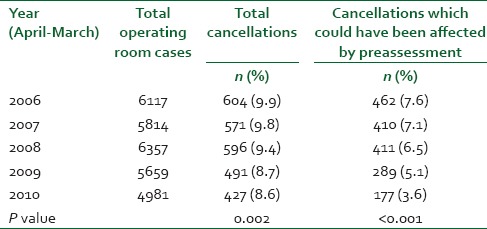
[Table 2]. shows the relationship between total operating room cases, total cancellations and the cancellations on the day of surgery which might have been affected by preoperative preparation. Total cancellations had declined from 9.9% in 2006 to 8.6% in 2010 (p-linear trend = 0.002). The cancellations which could have been affected by preoperative preparation decreased from 7.6% to 3.6% across the study period (P < 0.001).
Table 2.
Cancellations for reasons which might have been affected by preoperative preparation
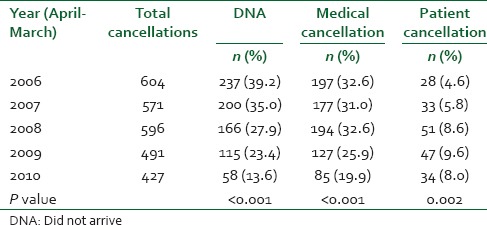
The cancellations which were expected to be affected by preoperative preparation can be further subdivided as shown in [Table 3]. This shows a decrease in cancellations due to DNA (from 39.2% to 13.6%, P < 0.001), medical reasons for cancellations (from 32.6% to 19.9%, P < 0.001) and an increase in the number of cancellations by the patients themselves (from 4.6% to 8%, P = 0.002) during the 5 years of the study.
Table 3.
Reasons for cancellation expected to be affected by preoperative preparation subdivided into “DNA”, cancellations due to medical reasons and cancellations by the patients themselves
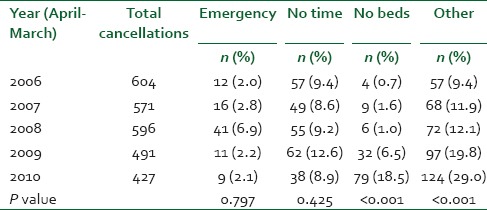
The cancellations which should not have been affected by preoperative preparation were further subdivided as shown in [Table 4]. Cancellations due to emergency operating room access and lack of time did not change significantly over time (P = 0.797 and P = 0.425, respectively). Cancellations due to lack of beds increased significantly from 0.7% to 18.5% and for “other” reasons from 9.4% to 29% (both P < 0.001) during the 5 years of the study.
Table 4.
Reasons for cancellation which would not have been affected by preoperative preparation. These are subdivided into cancellation due to emergency access being required, lack of operating room time, lack of hospital beds and other reasons
In the final year of the study, after excluding all surgical specialties not requiring anesthetic services, a total of 4981 operating room cases were available for analysis. Of these, 427 cases (8.6%) were cancelled and rescheduled. [Figure 2]. illustrates how these cancellations were distributed throughout the year according to the reason for cancellation. There was a marked increase in the number of cancellations in January 2011 (n = 81), which was almost entirely due to cancellations because of a lack of hospital beds (73%, 59/81).
Figure 2.
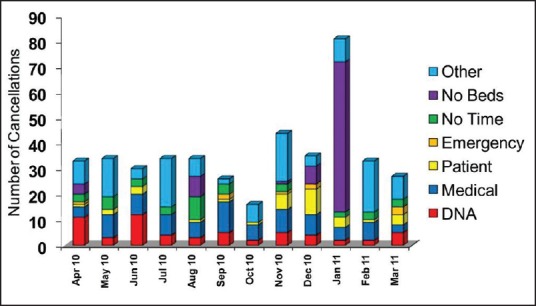
Operating room cancellations during the 2010-2011 year. The cancellations are grouped according to the reason for cancellation: Did not attend; cancellation by medical staff (medical); cancellation by the patient themselves (patient); interruption by emergency activity (emergency); lack of operating room time (no time); lack of hospital beds (no beds); and other reasons (other)
DISCUSSION
There was a significant reduction in total cancellations during the entire 5-year study period. Two of the three categories expected to have been affected by the introduction of a preoperative preparation clinic (medical cancellation and DNA) were significantly reduced during the period of the study. This study therefore supports data from previous studies showing that maximizing the health of patients in the preoperative preparation clinic before their surgery reduces the risk of cancellation on the day of surgery.[3,12,16,22] Unlike previous studies[3,22] where a nonsignificant reduction was demonstrated, we have shown that cancellations due to patient's not arriving for their surgery (DNA) were significantly reduced. However, contrary to expectation patient self-cancellation on the day of surgery increased. The suggestion is that the increase occurred in the early part of the study with a possible reversal of the trend toward the latter part. This is worthy of further investigation to determine if this trend is real. Previous studies have also been unable to demonstrate a significant reduction in patient reasons for cancellation with the introduction of a preoperative preparation clinic.[3,22]
Other studies[22] have further subdivided the reasons for patient cancellations (e.g., no reason, changed mind, unsuitable date etc.). Such a subdivision may have assisted in clarifying the unexpected increase which we found in patient self-cancellations. However, we were limited to the data provided by the hospital reports in which the categories had been predefined and had been in use for some time prior to the study being undertaken. From those categories available to us, we selected those categories which we felt “should” or “should not” be affected by preoperative preparation. The data for rescheduled operations at our hospital only includes patients cancelled after the creation of the final operating room list at 1600 on the day before surgery. Any cancellations made prior to this, such as unsuitable date, would not be recorded as a rescheduled operation and would therefore not be included in this data.
The categories which were expected not to have been affected by preoperative preparation (emergency access and lack of operating room time) did not show a significant reduction. Farasatkish et al.[3] also concluded that lack of operating room time was unaffected by preoperative assessment.
Knox et al.[22] demonstrated an increased bed availability following the introduction of their preoperative assessment clinic. In our study, cancellations due to lack of beds and “other” reasons showed a significant increase during the period of the study. However, as demonstrated in Figure 2 this lack of beds effect occurred almost entirely in January 2011. At the end of December 2010, one of the community hospitals was closed for refurbishment resulting in a diminished number of beds available for chronic care thereby reducing medical discharges from hospital. Shortly afterwards, in the 1st week of January 2011, two of the wards in the District General Hospital had to be closed due to an infection outbreak. The day-case unit was turned into an inpatient ward and all elective surgery was cancelled. These two factors produced the abnormal shortage of beds in January 2011. There was a similar peak in lack of beds in January 2010, which was due to extreme weather conditions in our local area with very heavy snowfalls. This created havoc with transport and thereby affected discharges from both the wards and community hospitals. Whilst these two abnormal periods contributed to the peaks shown, there has been a reduction in total bed numbers from 194 beds in 2006 to 170 beds in 2011 due mainly to reconfigurations to accommodate new infection control and fire guidance. This has led to higher numbers of outliers from the medical wards and a reduced ability to cope during periods of stress as outlined above.
Individual patient records were not examined in this study because the aim was to examine the overall impact on cancellations with the introduction of a preoperative preparation service. These data collection methods did not allow for collection of ASA and patient age data.
Our ultimate aspiration is that every patient who will require anesthesia (general or regional) administered by an anesthetist at our hospital will undergo preoperative preparation. Nursing shortages and the current financial constraints have dictated that this goal can only be achieved through a gradual roll-out to the various surgical specialties. This roll-out had not been completed by the end of the current study period. The study is unable to be continued or repeated because of the introduction of new operating room software which changes methods of recording of data.
The manual hospital record keeping system did not record the number of patients attending the preoperative preparation clinics, so we are unable to provide data to delineate the percentage uptake of the service. This was rectified with the introduction of the new operating room software at the end of the study period. The temporal roll-out of the preoperative preparation clinic is therefore, the only data available to estimate the relationship to the cancellations. Prior to 2007 (in the 1st year of the study) only patients for major orthopedic surgery and/or ASA 3 or higher patients were seen in a preoperative assessment clinic. From 2007, the service underwent a moderate expansion to include ophthalmology, ENT and pediatric dental surgery. In 2010, patients scheduled for major surgery or with major medical problems (ASA 3 or higher) for both general surgery and gynecology were rolled into the system. At the end of the study period, the only group of patients still not undergoing preoperative preparation was those general, orthopedic, and gynecological surgical patients scheduled for minor surgical procedures and with an ASA 2 or less. We have now achieved 100% preoperative preparation of elective cases, but are unable to include this data in the study due to the introduction of new operating room software, which changed methods of recording data.
The delay between the visit to the clinic and the date of surgery is completely variable and tends to depend on the waiting lists of individual surgeons and or specialties. It can vary from a few days for cancer or some gynecological procedures to 12 weeks or more for orthopedics. All patients are advised to contact the preoperative preparation clinic should there be any changes in coexisting morbidities or medications. The anesthetist undertaking the anesthetic also checks if any changes have occurred. In the absence of any changes, investigations are deemed valid up to 12 weeks after which they should be repeated on admission.
A limitation of the current data is that there is local anesthetic cases included in the general lists which had no anesthetic input and the present system of collating data does not allow us to identify them. However, since this practice did not change during the 5-year study period, its impact would be consistent across the years. It is quite probable that cases performed under local anesthesia would have decreased because of the introduction of dedicated local anesthetic lists. A further limitation of this study was that information was not available from patient files because they were not examined in this study as the objective of the study was to examine cancellations in theatre during the introduction of a preoperative preparation service at our hospital.
CONCLUSION
This pragmatic observational study provides evidence that the introduction of preoperative preparation clinics for patients reduces cancellations on the day of surgery and supports the business case that was made for the innovation at Dr. Gray's Hospital to roll-out preoperative preparation to all surgical specialties. The findings are contrary to those of the CRD review in 2007, which concluded that the evidence in the United Kingdom was weak that preassessment reduced cancellations on the day of surgery.[23,24]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gilmartin J. Day surgery: Patients’ perceptions of a nurse-led preadmission clinic. J Clin Nurs. 2004;13:243–50. doi: 10.1046/j.1365-2702.2003.00836.x. [DOI] [PubMed] [Google Scholar]
- 2.Fischer SP. Development and effectiveness of an anesthesia preoperative evaluation clinic in a teaching hospital. Anesthesiology. 1996;85:196–206. doi: 10.1097/00000542-199607000-00025. [DOI] [PubMed] [Google Scholar]
- 3.Farasatkish R, Aghdaii N, Azarfarin R, Yazdanian F. Can preoperative anesthesia consultation clinic help to reduce operating room cancellation rate of cardiac surgery on the day of surgery? Middle East J Anesthesiol. 2009;20:93–6. [PubMed] [Google Scholar]
- 4.Pollard JB, Zboray AL, Mazze RI. Economic benefits attributed to opening a preoperative evaluation clinic for outpatients. Anesth Analg. 1996;83:407–10. doi: 10.1097/00000539-199608000-00035. [DOI] [PubMed] [Google Scholar]
- 5.Asimakopoulos G, Harrison R, Magnussen PA. Pre-admission clinic in an orthopaedic department: Evaluation over a 6-month period. J R Coll Surg Edinb. 1998;43:178–81. [PubMed] [Google Scholar]
- 6.Conway JB, Goldberg J, Chung F. Preadmission anesthesia consultation clinic. Can J Anaesth. 1992;39:1051–7. doi: 10.1007/BF03008374. [DOI] [PubMed] [Google Scholar]
- 7.Badner NH, Craen RA, Paul TL, Doyle JA. Anesthesia preadmission assessment: A new approach through use of a screening questionnaire. Can J Anaesth. 1998;45:87–92. doi: 10.1007/BF03012002. [DOI] [PubMed] [Google Scholar]
- 8.Lacqua MJ, Evans JT. Cancelled elective surgery: An evaluation. Am Surg. 1994;60:809–11. [PubMed] [Google Scholar]
- 9.Holt NF, Silverman DG, Prasad R, Dziura J, Ruskin KJ. Preanesthesia clinics, information management, and operating room delays: Results of a survey of practicing anesthesiologists. Anesth Analg. 2007;104:615–8. doi: 10.1213/01.ane.0000255253.62668.3a. [DOI] [PubMed] [Google Scholar]
- 10.Jiminez A, Artigas C, Elia M, Casamayor C, Gracia JA, Martinez M. Cancellations in ambulatory day surgery: Ten years observational study. Ambul Surg. 2006;12:119–23. [Google Scholar]
- 11.Ferschl MB, Tung A, Sweitzer B, Huo D, Glick DB. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiology. 2005;103:855–9. doi: 10.1097/00000542-200510000-00025. [DOI] [PubMed] [Google Scholar]
- 12.Cantlay KL, Baker S, Parry A, Danjoux G. The impact of a consultant anaesthetist led pre-operative assessment clinic on patients undergoing major vascular surgery. Anesthesia. 2006;61:234–9. doi: 10.1111/j.1365-2044.2005.04514.x. [DOI] [PubMed] [Google Scholar]
- 13.Jackson J, Bramhall J. The preoperative association. R Coll Anaesth Bull. 2004;23:1162. [Google Scholar]
- 14.The Association of Anaesthetists of Great Britain and Ireland. The Anesthesia Team 3. 2010 May [Google Scholar]
- 15.The Association of Anaesthetists of Great Britain and Ireland. Pre-operative Assessment: the Role of the Anaesthetist 2. 2010 Jan [Google Scholar]
- 16.Reed M, Wright S, Armitage F. Nurse-led general surgical pre-operative assessment clinic. J R Coll Surg Edinb. 1997;42:310–3. [PubMed] [Google Scholar]
- 17.Barnes PK, Emerson PA, Hajnal S, Radford WJ, Congleton J. Influence of an anaesthetist on nurse-led, computer-based, pre-operative assessment. Anesthesia. 2000;55:576–80. doi: 10.1046/j.1365-2044.2000.01377.x. [DOI] [PubMed] [Google Scholar]
- 18.Rai MR, Pandit JJ. Day of surgery cancellations after nurse-led pre-assessment in an elective surgical centre: The first 2 years. Anesthesia. 2003;58:692–9. doi: 10.1046/j.1365-2044.2003.03189_3.x. [DOI] [PubMed] [Google Scholar]
- 19.Correll DJ, Bader AM, Hull MW, Hsu C, Tsen LC, Hepner DL. Value of preoperative clinic visits in identifying issues with potential impact on operating room efficiency. Anesthesiology. 2006;105:1254–9. doi: 10.1097/00000542-200612000-00026. [DOI] [PubMed] [Google Scholar]
- 20.Blanc-Jouvan M, Mercatello A, Long D, Benoit MP, Khadraoui M, Némoz C, et al. The value of anesthesia consultation in relation to the single preanesthetic visit. Ann Fr Anesth Reanim. 1999;18:843–7. doi: 10.1016/s0750-7658(00)88191-5. [DOI] [PubMed] [Google Scholar]
- 21.Emanuel A, Macpherseon R. The anaesthetic pre-admission clinic is effective in minimising surgical cancellation rates. Anaesth Intensive Care. 2013;41:90–4. doi: 10.1177/0310057X1304100115. [DOI] [PubMed] [Google Scholar]
- 22.Knox M, Myers E, Hurley M. The impact of pre-operative assessment clinics on elective surgical case cancellations. Surgeon. 2009;7:76–8. doi: 10.1016/s1479-666x(09)80019-x. [DOI] [PubMed] [Google Scholar]
- 23.The Cochrane Library, Centre for Reviews and Dissemination, Database of Abstracts of Reviews of Effects. Does nurse-led pre-operative assessment reduce the cancellation rate of elective surgical in-patient procedures: a systematic review of the research literature (Structured abstract) 2014:1. [Google Scholar]
- 24.Craig SE. Does nurse-led pre-operative assessment reduce the cancellation rate of elective surgical in-patient procedures? A systematic review of the research literature. Br J Anaesth Recovery Nurs. 2005;6:41–7. [Google Scholar]
- 25.London: NICE; 2003. National Institute for Clinical Excellence. Pre-Operative Tests, the Use of Routine Pre-Operative Tests for Elective Surgery. [Google Scholar]