

Abstract
Mask ventilation, along with tracheal intubation, is one of the most basic skills for managing an airway during anesthesia. Facial anomalies are a common cause of difficult mask ventilation, although numerous other factors have been reported. The long and narrow mandible is a commonly encountered mandibular anomaly. In patients with a long and narrow mandible, the gaps between the corners of the mouth and the lower corners of the mask are likely to prevent an adequate seal and a gas leak may occur. When we administer general anesthesia for these patients, we sometimes try to seal the airway using several sizes and shapes of commercially available face masks. We have found that the management of the airway for patients with certain facial anomalies may be accomplished by attaching a mask upside down.
Key Words: Airway management, Facemask, Ventilation
Mask ventilation, along with tracheal intubation, is one of the most basic skills for managing an airway during anesthesia. Facial anomalies are a common cause of difficult mask ventilation, although numerous other factors have been reported.1,2 The long and narrow mandible is a commonly encountered mandibular anomaly. In patients with a long and narrow mandible, the gaps between the corners of the mouth and the lower corners of the mask are likely to prevent an adequate seal, and a gas leak may occur. When we administer general anesthesia for these patients, we sometimes try to seal the airway using several sizes and shapes of commercially available face masks. We have found that management of the airway for patients with facial anomalies may be accomplished by attaching a mask upside down (see Figure 1).
Figure 1.
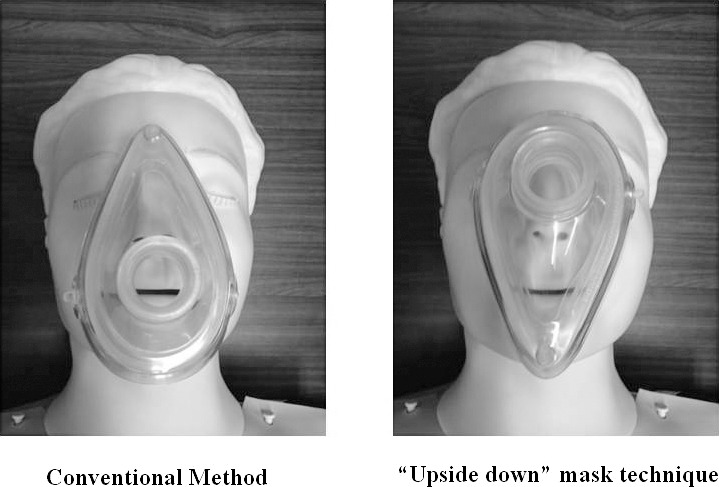
The conventional method and the upside-down mask technique.
A 27-year-old man (155 cm height, 56 kg body weight) with Opitz syndrome presented for the removal of bilateral mandibular impacted wisdom teeth. He had a long and narrow mandible (Figure 2). Before induction of anesthesia, we attempted to fit a mask on his face using the conventional method. However, there were gaps between the corners of the mouth and the lower corners of the mask. These gaps were associated with air leakage during spontaneous breathing when assessed by measuring tidal volume. We turned the face mask upside down and fitted the mask to his face once again. The gap between face and mask completely disappeared, and there was almost no significant leakage during inflation and deflation within an appropriate range of tidal volumes. General anesthesia was induced with propofol 70 mg and a remifentanil infusion of 0.5 μg/kg/h. Immediately after induction, we were not able to perform sufficient ventilation because of the gas leak from the gaps when we attempted to ventilate the patient with the conventional method. Airway pressure could not reach 10 cm H2O, although we increased the total gas flow rate. However, with the upside-down mask technique, we were able to ventilate the patient easily (Figure 3), being careful to avoid excess pressure on the eyes.
Figure 2.

The frontal view of the patient with a long and narrow mandible.
Figure 3.

Ventilation with the upside-down mask technique for the patient with a long and narrow mandible.
There are several methods and techniques of mask ventilation that have been previously reported. This technique may be useful for a patient with a long and narrow mandible. We believe that this technique may be useful in clinical practice in anesthesia.
ACKNOWLEDGMENT
The authors would like to thank Prof Paul Moore (University of Pittsburgh) for his understanding and suggestions in editing this report.
REFERENCES
- 1.El-Orbany M, Woehlck HJ. Difficult mask ventilation. Anesth Analg. 2009;109:1870–1880. doi: 10.1213/ANE.0b013e3181b5881c. [DOI] [PubMed] [Google Scholar]
- 2.Nargozian C. The airway in patients with craniofacial abnormalities. Paediatr Anaesth. 2004;14:53–59. doi: 10.1046/j.1460-9592.2003.01200.x. [DOI] [PubMed] [Google Scholar]