

Abstract
The disease concept of clear cell (tubulo) papillary renal cell carcinoma (CCP-RCC) as a distinct subtype of renal cell carcinoma has been recently established. First described in the setting of end stage renal disease, this tumor type is more frequently recognized and encountered in a sporadic setting. In this article, we provide an overview of the recent understanding of this tumor. Macroscopically, tumors are well circumscribed with well-developed tumor capsule. Histologically, the tumor cells are cuboidal to low columnar cell with clear cytoplasm and papillary and tubulo-papillary configuration. Immunohistochemically, tumor cells generally show diffuse expression for cytokeratin 7, CA9 (cup-shaped pattern), HIF-1, GLUT-1 and high molecular weight cytokeratin, but negative for AMACR, RCC Ma and TFE3. CD10 is negative or focally positive in most tumors. Genetically, this tumor has no characteristics of clear cell RCC or papillary RCC. Prognostically, patients with CCP-RCC behave in an indolent fashion in all previously reported cases. In conclusion, although this tumor has been integrated into recent International Society of Urologic Pathology Classification of renal neoplasia, both aspects of disease concept and clinical behavior are yet to be fully elucidated. Further publications of large cohorts of patients will truly help understand the biologic potential and the molecular underpinnings of this tumor type.
Keywords: Clear cell (tubulo) papillary renal cell carcinoma, pathology
Introduction
The concept of clear cell papillary renal cell carcinoma (CCP-RCC) has been recently proposed through the analyses of renal epithelial neoplasms arising in end-stage renal disease by Tickoo et al, including the senior author of this review paper [1]. Actually, Michal et al. described the disease entity of renal angiomyoadenomatous tumor (RAT) six years earlier before the report of Tickoo et al. [2,3] which has several overlapping features of CCP-RCC. Aydin et al. in a large series designated similar tumors as clear cell tubulopapillary RCC (CCTP-RCC) [4]. In the International Society of Urological Pathology (ISUP) Vancouver Classification of renal neoplasia, these three entities have been unified using the diagnostic term “clear cell (tubulo) papillary renal cell carcinoma (CCP-RCC)” [5]. However, concepts of this tumor are still evolving on various fronts including its biologic potential and the molecular underpinnings. In this article, we review CCP-RCC with focus on clinical and pathobiological aspects and comment future perspectives.
Epidemiology
The frequency of this tumor is estimated to account for 1 to 4.3% of all renal epithelial neoplasms [5-9]. CCP-RCC is considered to be the fourth most common histologic type of RCC in one study, but the diagnostic criteria should be steadily established in order to exclude mimickers of CCP-RCC [9]. CCP-RCC comprises 9.3% of all renal tumors occurring in young adults [11]. The age of patients with CCP-RCC range from 18 to 88 years with a mean age of 70 years [5]. There is no sex predilection [4,5,9]. CCP-RCC can occur in normal kidney (sporadic, non familial setting), non-cystic end-stage renal disease (ESRD) and acquired cystic disease (ACD) [1,6-9,12-14]. Two cases with CCP-RCC occurred within less than 10 years of hemodialysis [15]. Some cases associated with von Hippel-Lindau disease have been reported [4,6,9,10]. The association with other renal tumors has been described including clear cell RCC, papillary RCC, chromophobe RCC, multilocular cystic RCC, acquired cystic disease-associated RCC (ACD-RCC) and renal oncocytoma [6-9].
Clinical symptoms and signs
Patients with CCP-RCC usually are asymptomatic, but may present with flank or abdominal pain [9]. Some tumors are found during the follow-up of dialysis.
Imaging findings
The computed tomography (CT) scan of the tumor discloses the low density with cystic change or cystic formation. The magnetic resonance imaging of the tumor reveals the isointensity on T1-weighted images and hypointensity on T2-weighted images [16].
Pathological findings
Macroscopic findings
CCP-RCC is generally well defined and well encapsulated [5,8,12-14,17,18]. Cystic change or cystic formation is very frequent [4,5,8,13,14,18]. The tumors are usually small [4,6,7,12,14,17]. The tumor is usually solitary and unilateral, but multifocality and bilaterality have been reported [4,6,7,13,19,20]. The cut surface of the tumor shows tan-white, pink-tan, yellow or red-brown color [5,7,14]. Necrosis is absent, but focal hemorrhage may be present [8,14].
Microscopic findings
CCP-RCC is composed of various proportions of papillary, tubular/acinar, cystic and solid sheet-like or nested architectures with clear cytoplasm (Figure 1A) [4-9,12,14,18,21,22]. Small blunt papillae, focal branching papillae/acini and interconnecting ribbon are common findings [4,7,12,14]. However, extensively branching papillae are uncommon [7]. Foci of large cells or eosinophilic cells may be present [4,7,21]. Proteinaceous secretion is frequently observed within lumina of the tubules or acini, and cystic spaces contain seroanguinous fluid or colloid-like section [4]. Nuclei of most CCP-RCCs have a horizontally linear arrangement apart from the basement membrane (Figure 1B) [4,5,7,8,12,14,19,21,22]. According to the Fuhrman’s criteria, nuclear atypia corresponds to Fuhrman Grade 1 or 2 [4-9,12,14,17,19,21]. In many cases, the stroma demonstrates smooth muscle metaplasia usually connecting with the tumor capsule [2,3,8,14,19]. Fibrous stroma is also common [21]. However, the aggregation of foamy macrophages, psammoma bodies and hemosiderin depositions are basically absent [23]. Lymphovascular invasion, renal sinus invasion and tumor necrosis have not been documented to date [23].
Figure 1.
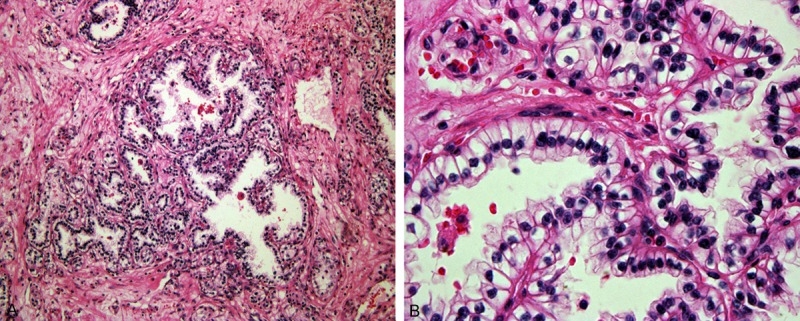
Histological findings of clear cell (tubulo) papillary renal cell carcinoma (CCP-RCC). A: The tumor consists of clear cell arranged with papillary architecture. Small blunt papillae and focal branching papillae/acini are common. B: The nuclei are detached from basal membrane.
Immunohistochemical findings
Tumor cells are diffusely positive for cytokeratin 7 (Figure 2A), cytokeratin 34betaE12, CA9, vimentin, HIF-1 and GLUT-1, PAX2 and PAX8, but negative for α-methyacyl-CoA racemase (AMACR) (Figure 2B), RCC Ma, TFE3, TFEB, parvalbumin, vinculin, and cathepsin K [1,4-9,12-15,17-24]. CA9 staining is of characteristic “cup”-like pattern with atypical surface of the tumor cells devoid of staining. CD10 is negative or focally positive in most cases [4-7,12,14,17,21,23,24]. Parafibromin, protein encoded by HRPT2, whose germline mutation leads to hereditary hyperparathyroidism-jaw tumor syndrome is diffusely positive in all cases with CCP-RCC [25]. Nuclear expression of cyclin D1 has been described [26]. The smooth muscle stroma shows labelling for alpha smooth muscle actin, but no labelling for ER and PgR [7].
Figure 2.
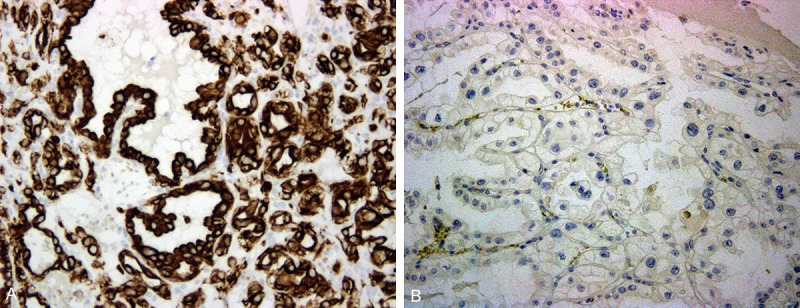
Immunohistochemical findings of CCP-RCC. A: The tumor shows diffuse labelling for cytokeratin 7. B: AMACR staining shows a negative result.
Ultrastructural findings
The neoplastic cell membrane showed short apicolateral microvilli and cytoplasmic interdigitation. Well-developed desmosomes are observed. The cytoplasm contain abundant intermediate filaments, free ribosomes, rough-surfaced endoplasmic reticulum, mitochondria, lysosomes and scanty lipid deposits [8], or consists of numerous glycogen granules with scanty cell organelles reminiscent of clear cell RCC [17].
Molecular genetic findings
This tumor generally lacks genetic abnormalities observed in either clear cell RCC or papillary RCC [5,18]. Namely, this tumor does not have chromosome 3p deletion or polysomy of chromosomes 7 and 17 [4,12,14,17,19]. Neither mutation nor promoter methylation of VHL gene has been reported to date [4,17,19,20,27]. VHL mRNA is generally overexpressed, compared with normal renal tissue and clear cell RCC [19]. The array comparative genomic hybridization (CGH) of seven tumors showed no chromosomal imbalances [21]. In contrast, CCP-RCC in CGH analysis of patients with ESRD showed similar profile to papillary RCC, particularly in cases with coexistent CCP-RCC and papillary RCC arising in ESRD [28]. However, the frequency of gain of chromosome 16 or gain of chromosomes 7 and 17 in CCP-RCC is higher or lower than that of papillary RCC arising in ESRD, respectively. Copy number changes using single-nucleotide polymorphism arrays showed the difference between CCP-RCC and clear cell RCC in 3p losses, 5q gains and 8p losses [19]. However, losses of chromosome 3 have been detected in three cases [17]. A case with trisomy of chromosomes 7, 10 and 12 [20], and another case with gain of chromosomes 7 and 17 have been reported [4].
Pathogenesis
The activation of HIF pathway by non-VHL-dependent mechanisms may involved in the pathogenesis of CCP-RCC because of the immunohistochemical co-expression of CA9, HIF-1, and GLUT-1 in the absence of VHL gene alterations [17,19]. Elevated intra-tumoral sorbitol levels are the likely mechanism of HIF pathway activation [29]. In target next-generation sequencing and non-coding RNA analysis in CCP-RCC showed the different pathological mechanism from clear cell RCC or papillary RCC [30]. Namely, miR200 family is overexpressed in CCP-RCC, whereas low-expressed in clear cell RCC and papillary RCC.
Differential diagnosis
CCP-RCC should be distinguished from clear cell RCC, papillary RCC, Xp11.2 RCC, multilocular cystic RCC, tuberous sclerosis complex-associated RCC and VHL disease-associated CCP-RCC-like RCC. Some clear cell RCCs show focal or extensive papillary architecture [31-33]. This finding may be attributed to pseudopapillae formation due to fragmentation of acinar growth in high grade clear cell RCC with necrosis. High nuclear grade, the immunohistochemical negativity of cytokeratin 7 and AMACR, and loss of chromosome 3p or VHL gene alterations can achieve the final diagnosis of clear cell RCC [23,34]. On rare occasions, CK 7 may be positive in clear cell carcinoma with papillary/pseudopapillary features, though other markers including high molecular weight cytokeratin are negative and RCC Ma and CD 10 are positive. However, such tumors with low nuclear grade have been previously reported, and may be difficult to make a definitive diagnosis without molecular genetic studies [34]. Additionally, clear cell RCC may have areas resembling CCP-RCC [35,37]. Some papillary RCC may show focal or extensive clear cell change [33,34,37]. Clear cell change in papillary RCC is usually in combination with hemosiderin deposition and/or necrosis and this cytoplasmic clearing may reflect phagocytic activity of carcinoma cells or caused by the change of local metabolic environment [23,33]. Pathologists should pay attention that a diagnosis of papillary RCC may be possible even in tumors with a minor papillary growth pattern [38]. In this situation, the confirmation of positivity for cytokeratin 7 and AMACR and polysomy of chromosomes 7 and 17 and loss of chromosome Y can lead to the diagnosis of papillary RCC [34,37,38]. In Xp11.2 RCC, voluminous tumor cells, psammoma bodies or hyaline nodules may be observed. In this setting, the immunohistochemistry of TFE3 and cathepsin K may be helpful in the distinction between CCP-RCC and Xp11.2 RCC [39]. The break apart FISH for TFE3 gene or the identification of chimeric transcripts using RT-PCR is also available. Multilocular cystic RCC grossly lacks solid portion and immunohistochemically express CD10 and RCC Ma in most cases [40,41]. Pathologists may rarely encounter combined clear cell RCC and papillary RCC of sporadic type showing admixture of clear/eosinophilic cytoplasm and papillary/solid architecture [34,38]. In this situation, the immunohistochemical combination of CA9, cytokeratin 7 and AMACR and molecular genetic study including chromosomes 3p, 7 and 17 may serve in the conclusive diagnosis [34,38]. RCC in tuberous complex may resemble CCP-RCC. However, this tumor possesses delicate eosinophilic cytoplasmic thread-like strands and eosinophilic globules [42]. Tumors with morphology and immunoprofile similar to CCP-RCC have been reported in von Hippel-Lindau disease [4,6,9,10]. In one study, CCP-RCC-like tumors arising in patients with von Hippel-Lindau disease morphologically mimic true CCP-RCC, but immunohistochemical and genetic features significantly resemble those of clear cell RCC [43].
Therapy
Partial nephrectomy or total nephrectomy is generally the treatment provided for a solitary tumor when surgical resection is feasible [21]. As this tumor is generally indolent, the active surveillance with strict follow-up may be possible for selective cases and if the diagnosis can be reliably established preoperatively such as by a core biopsy.
Prognosis
To date, no patients have developed local recurrence, lymph-node or distant metastasis [4-9,12,14,17,18,20]. Accordingly, the possibility that this tumor be designated as a “low malignant potential” tumor has been suggested [5].
Future perspectives
In diagnostically difficult cases, the diagnosis should be supported by immunohistochemistry. CCP-RCC has different genetic features from clear cell RCC and papillary RCC [4,5,12,14,18,19,21,23,27]. Hence, molecular genetic studies including VHL gene mutation/methylation, 3p LOH and FISH of chromsomes 7 and 17 may be helpful though they are resource intensive and expensive. CCP-RCC-like tumors which are morphologically similar to CCP-RCC share genetic features of both clear cell RCC and papillary RCC and have also been reported [36,44]. Reliable histologic differences between both tumors must be clearly defined in future. Recently, Nagashima et al. have divided similar categories into the putative subgroups in histological and molecular genetic classification of RCC [45]. However, the precise positioning is yet not completely certain now with respect to tumors arising in the setting of end stage renal disease and in the setting of VHL disease. It is possible that future studies including genomic profiling may differ in CCP-RCC patients with and without ESRD/ACD [21,28]. Additionally, the morphological differences between CCP-RCC and CCP-RCC-like tumor in VHL disease should be more clarified. Although previous reports have demonstrated both immunohistochemical and genetic differences [4,6,9,10,43], the overall characteristics of the latter resemble those of clear cell RCC [43]. Another aspect that has been recently elucidated is that the leiomyomatous stroma in RCC including RAT is polyclonal and not part of the neoplastic process [46]. Accordingly, we can recognize that three entities including CCP-RCC (sporadic, end stage renal disease), RAT and CCTP-RCC actually represent the same entity and none of previously reported more than 100 cases in these categories have had neither recurrence nor metastasis [4-9,12,14,17,18,20]. CCP-RCCs with lymphovascular invasion, renal sinus invasion and tumor necrosis have not been described to date and, furthermore interestingly, the great majority of CCP-RCC showed the Stage I except for two cases showing Stage II [1,4,6-9,12-14,17,19,21,25]. In the recent ISUP classification, the term of “low malignant potential” similar to that of multilocular cystic RCC has been proposed on the basis of these indolent clinical features [5]. Recently, the first author of this review article has referred the diagnostic terminology of “clear cell papillary adenoma (CCPA)” for small clear cell papillary lesions less than 5mm in size occurring in end-stage renal disease, like papillary adenoma [47]. It is possible that the spectrum of CCPA may be expanded to include most, if not all, CCP-RCC in the future, if further studies prove CCP-RCC exhibit universally benign clinical behavior. Further investigation of CCP-RCC to address these unresolved or evolving issues will be necessary to confirm the indolent clinical behavior and emerging understanding of the pathogenesis of this tumor, and tumors related to it.
Disclosure of conflict of interest
None.
References
- 1.Tickoo SK, deParalta-Venturia MN, Harik LR, Worcester HD, Salama ME, Young AN, Moch H, Amin MB. Spectrum of epithelial neoplasms in end-stage renal disease. An experience from 66 tumor-bearing kidneys with emphasis on histologic patterns distinct from those in sporadic adult renal neoplasia. Am J Surg Pathol. 2006;30:141–153. doi: 10.1097/01.pas.0000185382.80844.b1. [DOI] [PubMed] [Google Scholar]
- 2.Michal M, Hes O, Havlicek F. Benign renal angiomyoadenomatous tumor: a previously unreported renal tumor. Ann Diagn Pathol. 2000;4:311–315. doi: 10.1053/adpa.2000.17890. [DOI] [PubMed] [Google Scholar]
- 3.Michal M, Hes O, Nemcova J, Sima R, Kuroda N, Bulimbasic S, Franco M, Sakaida N, Danis D, Kazakov DV, Ohe C, Hora M. Renal angiomyoadenomatous tumor: morphologic, immunohistochemical, and molecular genetic study of a distinct entity. Virchows Arch. 2009;454:89–99. doi: 10.1007/s00428-008-0697-3. [DOI] [PubMed] [Google Scholar]
- 4.Aydin H, Chen L, Cheng L, Vaziri S, He H, Ganapathi R, Delahunt B, Magi-Galluzzi C, Zhou M. Clear cell tubulopapillary renal cell carcinoma: A study of 36 distinctive low-grade epithelial tumors of the kidney. Am J Surg Pathol. 2010;34:1608–1621. doi: 10.1097/PAS.0b013e3181f2ee0b. [DOI] [PubMed] [Google Scholar]
- 5.Srigley JR, Delahunt B, Eble JN, Egevad L, Epstein JI, Grignon D, Hes O, Moch H, Montironi R, Tickoo SK, Zhou M, Argani P The ISUP Renal Tumor Pane. The International Society of Urological Pathology (ISUP) Vancouver Classification of renal neoplasia. Am J Surg Pathol. 2013;37:1469–1489. doi: 10.1097/PAS.0b013e318299f2d1. [DOI] [PubMed] [Google Scholar]
- 6.Park JH, Lee C, Suh JH, Moon KH. Clear cell papillary renal cell carcinoma: A report of 15 cases including three cases of concurrent other-type renal cell carcinomas. Korean J Pathol. 2012;46:541–547. doi: 10.4132/KoreanJPathol.2012.46.6.541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Williamson SR, Eble JN, Cheng L, Grignon DJ. Clear cell papillary renal cell carcinoma: differential diagnosis and extended immunohistochemical profile. Mod Pathol. 2013;26:697–798. doi: 10.1038/modpathol.2012.204. [DOI] [PubMed] [Google Scholar]
- 8.Alexiev BA, Drachenberg CB. Clear cell papillary renal cell carcinoma: incidence, morphological features, immunohistochemical profile, and biological behavior: a single institution study. Pathol Res Pract. 2014;210:234–241. doi: 10.1016/j.prp.2013.12.009. [DOI] [PubMed] [Google Scholar]
- 9.Zhou H, Zheng S, Troung LD, Ro JY, Ayala AG, Shen SS. Clear cell papillary renal cell carcinoma in the fourth most common histologic type of renal cell carcinoma in 290 consecutive nephrectomies for renal cell carcinoma. Hum Pathol. 2014;45:59–64. doi: 10.1016/j.humpath.2013.08.004. [DOI] [PubMed] [Google Scholar]
- 10.Rao P, Monzon F, Jonasch E, Matin SF, Tamboli P. Clear cell papillary renal cell carcinoma in patients with von Hippel-Lindau syndrome-clinicopathologic features and comparative genomic analysis of 3 cases. Hum Pathol. 2014;45:1966–1972. doi: 10.1016/j.humpath.2014.06.004. [DOI] [PubMed] [Google Scholar]
- 11.López JI, Mereno V, Garcia H, Anton I, Robles A, Onate JM, Banos A, Escandon J, Ugalde A. Renal cell carcinoma in young adults: A study of 130 cases and a review of previous series. Urol Int. 2010;84:292–300. doi: 10.1159/000288231. [DOI] [PubMed] [Google Scholar]
- 12.Gobbo S, Eble JN, Grignon DJ, Martignoni G, MacLennan GT, Shah RB, Zhang S, Brunelli M, Cheng L. Clear cell papillary renal cell carcinoma. A distinct histopathologic and molecular genetic entity. Am J Surg Pathol. 2008;32:1239–1245. doi: 10.1097/PAS.0b013e318164bcbb. [DOI] [PubMed] [Google Scholar]
- 13.Bhatnagar R, Alexxiev BA. Renal-cell carcinomas in end-stage kidneys: A clinicopathological study with emphasis on clear-cell papillary renal-cell carcinoma and acquired cystic kidney-associated carcinoma. Int J Surg Pathol. 2012;20:19–28. doi: 10.1177/1066896911414273. [DOI] [PubMed] [Google Scholar]
- 14.Alexiev BA, Thomas C, Zou YS. Clear cell papillary renal cell carcinoma with angiomyomatous stroma: a histological, immunohistochemical, and fluorescence in situ hybridization study. Virchows Arch. 2014;464:709–716. doi: 10.1007/s00428-014-1581-y. [DOI] [PubMed] [Google Scholar]
- 15.Nouh MAAM, Kuroda N, Yamashita M, Hayashida Y, Yano T, Manakuchi J, Taniguchi S, Nomura I, Inui M, Sugimoto M, Kakehi Y. Renal cell carcinoma in patients with end-stage renal disease: relationship between histological type and duration of dialysis. BJU Int. 2009;105:620–627. doi: 10.1111/j.1464-410X.2009.08817.x. [DOI] [PubMed] [Google Scholar]
- 16.Sahni VA, Hirch MS, Silverman SG. Renal angiomyoadenomatous tumour: Imaging features. Can Urol Assoc. 2012;6:E140–E143. doi: 10.5489/cuaj.11072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shi SS, Shen Q, Xia QY, Tu P, Shi QL, Zhou XJ, Rao Q. Clear cell papillary renal cell carcinoma: a clinicopathological study emphasizing ultrastructural features and cytogenetic heterogeneity. Int J Clin Exp Pathol. 2013;6:2936–2942. [PMC free article] [PubMed] [Google Scholar]
- 18.Kuroda N, Tanaka A. Recent classification of renal epithelial tumors. Med Mol Morphol. 2014;42:68–75. doi: 10.1007/s00795-013-0033-0. [DOI] [PubMed] [Google Scholar]
- 19.Rohan SM, Xiao Y, Liang Y, Dudas ME, Al-Ahmadie HA, Fine SW, Gopalan A, Reuter VE, Rosenblum MK, Russo P, Tickoo SK. Clear-cell papillary renal cell carcinoma: molecular and immunohistochemical analysis with emphasis on the von Hippel-Lindau gene and hypoxia-inducible factor pathway-related proteins. Mod Pathol. 2011;24:1207–1220. doi: 10.1038/modpathol.2011.80. [DOI] [PubMed] [Google Scholar]
- 20.Wolfe A, Dobin SM, Grossmann P, Michal M, Donner LR. Clonal trisomies 7, 10 and 12, normal 3p and absence of VHL gene mutation in a clear cell tubulopapillary carcinoma of the kidney. Virchows Arch. 2011;459:457–463. doi: 10.1007/s00428-011-1137-3. [DOI] [PubMed] [Google Scholar]
- 21.Adam J, Couturier J, Molinie V, Vieillefond A, Sibony M. Clear-cell papillary renal cell carcinoma: 24 cases of a distinct low-grade renal tumour and a comparative genomic hybridization array study of seven cases. Histopathology. 2011;58:1064–1071. doi: 10.1111/j.1365-2559.2011.03857.x. [DOI] [PubMed] [Google Scholar]
- 22.Crumley SM, Divatia M, Troung L, Shen S, Ayala AG, Ro JY. Renal cell carcinoma: Evolving and emerging subtypes. World J Clin Cases. 2013;16:262–275. doi: 10.12998/wjcc.v1.i9.262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ross H, Martignoni G, Argani P. Renal cell carcinoma with clear cell and papillary features. Arch Pathol Lab Med. 2012;136:391–399. doi: 10.5858/arpa.2011-0479-RA. [DOI] [PubMed] [Google Scholar]
- 24.Kuroda N, Tanaka A, Ohe C, Nagashima Y. Recent advances of immunohistochemistry for diagnosis of renal tumors. Pathol Int. 2013;63:381–390. doi: 10.1111/pin.12080. [DOI] [PubMed] [Google Scholar]
- 25.Cui C, Ziober A, Bing Z. Expression of parafibromin in clear cell papillary renal cell carcinoma. Appl Immunohistochem Mol Morphol. 2013;21:322–325. doi: 10.1097/PAI.0b013e31827362c9. [DOI] [PubMed] [Google Scholar]
- 26.Leroy X, Campero P, Gnemmi V, Aubert S, Flamand V, Roupret M, Fantoni JC, Comperat E. Clear cell papillary renal cell carcinoma is an indolent and low-grade neoplasm with overexpression of cyclin D1. Histopathology. 2014;64:1032–1036. doi: 10.1111/his.12359. [DOI] [PubMed] [Google Scholar]
- 27.Shahzad H, Kehar SI, Ali S, Tariq N. Expression of von Hippel-Lindau (VHL) gene mutation in diagnosed cases of renal cell carcinoma. Pak J Med Sci. 2014;30:880–885. doi: 10.12669/pjms.304.4733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Inoue T, Matuura K, Yoshimoto T, Nguyen LT, Tuskamoto Y, Nakada C, Hijiya N, Narimatsu T, Nomura T, Sato F, Nagashima Y, Kashima K, Hatakeyama S, Ohyama C, Numakura K, Habuchi T, Nakagawa M, Seto M, Mimata H, Moriyama M. Genomic profiling of renal cell carcinoma in patients with end-stage renal disease. Cancer Sci. 2012;103:569–576. doi: 10.1111/j.1349-7006.2011.02176.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tickoo SK, Hakimi AA, Xu J, Lee CH, Chen YB, Stirdivant S, Neri B, Wolfert R, Fine SW, AlAhmadie H, Gopalan A, Reuter VE, Hsieh JJ. Sorbital as a novel mechanism of Hypoxia-inducible factor (HIF) pathway activation in clear cell papillary renal cell carcinoma. Mod Pathol. 2014;27:263A–264A. [Google Scholar]
- 30.Lawrie CH, Larrea E, Larrinaga G, Goicoechea I, Arestin M, Fernadez-Mercado M, Hes O, Cáceres F, Manterola L, López JI. Targetred next-generation sequencing and non-coding RNA expression analysis of clear cell papillary carcinoma suggests distinct pathological mechanisms from other renal tumour subtypes. J Pathol. 2014;232:32–42. doi: 10.1002/path.4296. [DOI] [PubMed] [Google Scholar]
- 31.Füzesi L, Gunawan B, Bergmann F, Tack S, Braun S, Jakse G. Papillary renal cell carcinoma with clear cell cytomorphology and chromosomal loss of 3p. Histopahtology. 1999;35:157–161. doi: 10.1046/j.1365-2559.1999.00709.x. [DOI] [PubMed] [Google Scholar]
- 32.Salama ME, Worsham MJ, DePeralta-Venturina M. Malignant papillary renal tumors with extensive clear cell change. A molecular analysis by microsatellite analysis and fluorescence in situ hybridization. Arch Pathol Lab Med. 2003;127:1176–1181. doi: 10.5858/2003-127-1176-MPRTWE. [DOI] [PubMed] [Google Scholar]
- 33.Gobbo S, Eble JN, MacLennan GT, Grignon DJ, Shah RB, Zhang S, Martignoni G, Brunelli M, Cheng L. Renal cell carcinomas with papillary architecture and clear cell components. The utility of immunohistochemical and cytogenetical analyses in differential diagnosis. Am J Surg Pathol. 2008;32:1780–1786. doi: 10.1097/PAS.0b013e31818649ed. [DOI] [PubMed] [Google Scholar]
- 34.Mai KT, Faraji H, Desantis D, Robertson SJ, Belanger EC, Levac J. Renal cell carcinoma with mixed features of papillary and clear cell cytomorphology: a fluorescent in situ hybridization study. Virchows Arch. 2010;456:77–84. doi: 10.1007/s00428-009-0871-2. [DOI] [PubMed] [Google Scholar]
- 35.Kuroda N, Hosokawa T, Michal M, Hes O, Sima R, Ohe C, Lee GH. Clear cell renal cell carcinoma with focal renal angiomyoadenomatous tumor-like area. Ann Diagn Pathol. 2011;15:202–206. doi: 10.1016/j.anndiagpath.2010.03.003. [DOI] [PubMed] [Google Scholar]
- 36.Petersson F, Grossmann P, Hora M, Sperga M, Perez Montiel D, Martinek P, Cortes Gutierrez ME, Bulimbasic S, Michal M, Branzovsky J, Hes O. Renal cell carcinoma with areas mimicking renal angiomyoadenomatous tumor/clear cell papillary renal cell carcinoma. Hum Pathol. 2013;44:1412–1420. doi: 10.1016/j.humpath.2012.11.019. [DOI] [PubMed] [Google Scholar]
- 37.Billis A. Papillary renal cell carcinoma: Assesement of clear cell change and clinicopathologic correlation. Int Braz J Urol. 2006;32:366–368. [Google Scholar]
- 38.Haudebourg J, Hoch B, Fabas T, Chardot-Leccia N, Burel-Vandenbos F, Vieillefond A, Amiel J, Michiels JF, Pedeutour F. Strength of molecular cytogenetic analyses for adjusting the diagnosis of renal cell carcinomas with both clear cell and papillary features: a study of three cases. Virchows Arch. 2010;457:397–404. doi: 10.1007/s00428-010-0937-1. [DOI] [PubMed] [Google Scholar]
- 39.Kuroda N, Mikami S, Pan CC, Cohen RJ, Hes O, Michal M, Nagashima Y, Tanaka Y, Inoue K, Shuin T, Lee GH. Review of renal carcinoma associated with Xp11.2 translocations/TFE3 gene fusions with focus on pathobiological aspects. Histol Histopathol. 2012;27:133–140. doi: 10.14670/HH-27.133. [DOI] [PubMed] [Google Scholar]
- 40.Williamson SR, Halat S, Eble JN, Grignon DJ, Lopez-Beltran A, Montironi R, Tan PH, Wang M, Zhang S, MacLennan GT, Baldridge LA, Cheng L. Multilocular cystic renal cell carcinoma: Similarities and differences in immunoprofile compared with clear cell renal cell carcinoma. Am J Surg Pathol. 2012;36:1425–1433. doi: 10.1097/PAS.0b013e31825b37f0. [DOI] [PubMed] [Google Scholar]
- 41.Kuroda N, Ohe C, Mikami S, Inoue K, Nagashima Y, Cohen RJ, Pan CC, Michal M, Hes O. Multilocular cystic renal cell carcinoma with focus on clinical and pathobiological aspects. Histol Histopathol. 2012;27:969–974. doi: 10.14670/HH-27.969. [DOI] [PubMed] [Google Scholar]
- 42.Yang P, Cornejo KM, Sadow PM, Cheng L, Wang M, Xiao Y, Jiang Z, Oliva E, Jozwiak S, Nussbaum RL, Feldman AS, Paul E, Thiele EA, Yu JJ, Henske EP, Kwiatkowski DJ, Young RH, Wu CL. Renal cell carcinoma in tuberous sclerosis complex. Am J Surg Pathol. 2014;38:895–909. doi: 10.1097/PAS.0000000000000237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Williamson SR, Zhang S, Eble JN, Grignon DJ, Martignoni G, Brunelli M, Wang M, Gobbo S, Baldridge LA, Cheng L. Clear cell papillary renal cell carcinoma-like tumors in patients with von Hippel-Lindau disease are unrelated to sporadic clear cell papillary renal cell carcinoma. Am J Surg Pathol. 2013;37:1131–1139. doi: 10.1097/PAS.0b013e318282dab8. [DOI] [PubMed] [Google Scholar]
- 44.Petersson F, Yan B, Huang J, Thamboo TP, Bing TK, Consigliere DT. Low-grade renal carcinoma with histologic features overlapping renal angiomyoadenomatous tumor and featuring polysomy 7 and 17 and a mutation in the von Hippel-Lindau gene: report of a hybrid tumor and a few comments on renal angiomyoadenomatous tumor and papillary renal tumors with clear cells. Ann Diagn Pathol. 2011;15:213–220. doi: 10.1016/j.anndiagpath.2010.10.005. [DOI] [PubMed] [Google Scholar]
- 45.Nagashima Y, Kuroda N, Yao M. Transition of organizational categoty on renal cancer. Jpn J Clin Oncol. 2013;43:233–242. doi: 10.1093/jjco/hyt006. [DOI] [PubMed] [Google Scholar]
- 46.Petersson F, Branzonvsky J, Martinek P, Korabecna M, Kruslin B, Hora M, Peckova K, Bauleth K, Pivovarcikova K, Michal M, Svajdler M, Sperga M, Bulimbasic S, Leroy X, Rychly B, Trivunic S, Kokoskova B, Rotterova P, Podhola M, Suster S, Hes O. The leiomyomatous stroma in renal cell carcinomas in polyclonal and not part of the neoplastic process. Virchows Arch. 2014;465:89–96. doi: 10.1007/s00428-014-1591-9. [DOI] [PubMed] [Google Scholar]
- 47.Kuroda N. Microscopic small clear cell papillary lesion of the kidney with long-term hemodialysis patient: Is this clear cell papillary adenoma? Pol J Pathol. 2014;65:248–249. doi: 10.5114/pjp.2014.45790. [DOI] [PubMed] [Google Scholar]