

Abstract
Primary malignant melanoma of esophagus is a rare but highly aggressive neoplasm, with an incidence less than 0.2% of all primary esophagus neoplasms. There are no clinical differences from other forms of esophagus cancer. Because initial symptoms are nonspecific, the patients are usually diagnosed at a late stage. The prognosis is poor, and curative effect seems disappointed. Several reports suggest that most of patients die from distant metastases, and the 5-year survival rate is approximately 4.2%. This case report includes a review of the surgical pathology, clinical features and treatment of primary malignant melanoma of esophagus. This case report presents a 56-year-old female with primary malignant melanoma of esophagus, treated by surgical resection. Till now, the patient is still alive for 5 months without any chemotherapy, radiotherapy and immunomodulatory therapy.
Keywords: Malignant melanoma, esophagus neoplasm, immunohistochemistry
Case presentation
A 56-year-old female presented with a 6 month history of dysphagia and weight loss of 2 kg, without retrosternal pain. A barium swallow was arranged and showed an irregular filling defect in the mid-lower esophagus (Figure 1). Gastroscopy revealed a large lobulated, black pigmented mass at 25 cm. Because of hemorrhage on contact surface and friable, biopsy was not taken (Figure 2). Computed tomography (CT) of thorax revealed an intra- luminal mass in the mid-lower of esophagus, which was well-defined. There was no apparent invasion and mediastinal lymph nodes enlargement (Figure 3).
Figure 1.
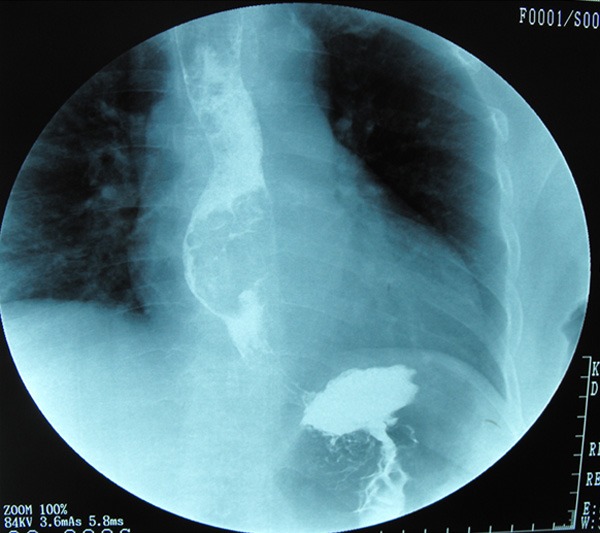
Barium swallow showed an irregular filling defect in the mid-lower third of esophagus.
Figure 2.
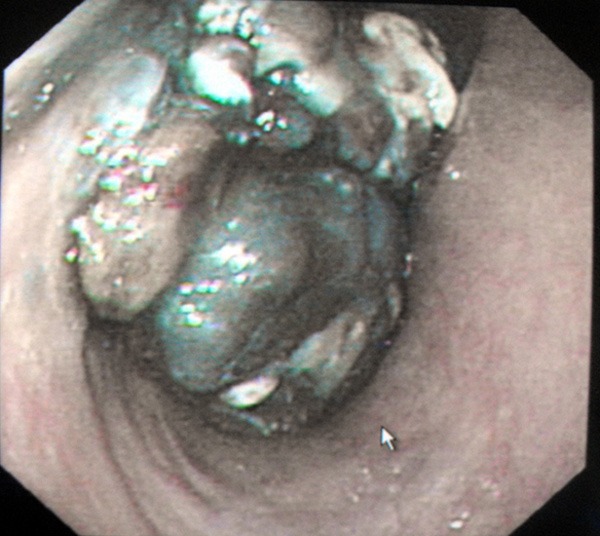
Gastroscopy showed a large lobulated and black pigmented nodule.
Figure 3.
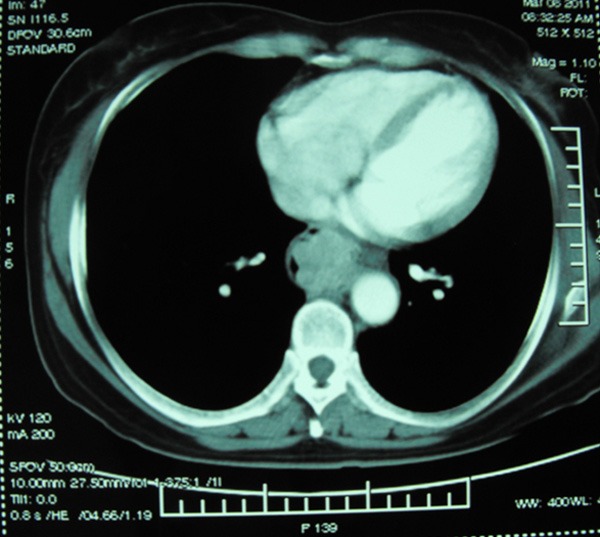
Computer tomography of the thorax revealed an intra-luminal mass, which was well-defined.
Macroscopic pathological assessment: The specimen consisted of 8 cm length of esophagus. A black pigmented nodule (5 cm ×3 cm ×3 cm) was located at the resected esophagus. The tumor was lobulated in appearance, intra-luminal growing. More than 90% of tumor lesions were black pigmented, containing several areas of hemorrhage and necrosis (Figure 4).
Figure 4.

Gross specimen, a black pigmented lobulated mass located at the resected esophagus.
Microscopic examination: The most of covering epithelium was intact and part was ulcerated. The tumor cells extended downward from the epithelium, with polymorphism. Most of tumor cells presented round or ovoid similar to epithelioid cells. The other tumor cells presented spindle-shapes with abundant cytoplasm. The nuclei were large, containing remarkable red nucleoli. The tumor arranged in nests or fascicular structure with melanin deposition (Figure 5A, 5B). By immunohistochemistry (IHC), tumor cells were positive to HMB-45, Melan-A, S-100 protein and cytokeratin (CK) pan (Figure 5C-F). All of these supported the diagnosis of melanoma. The melanocytes were mainly located in the mucosa, few invaded into submucosa. There was no muscular layer invasion. Two of eleven lymph nodes were found with metastasis melanocytes. The incisal margins of the specimen were clear.
Figure 5.
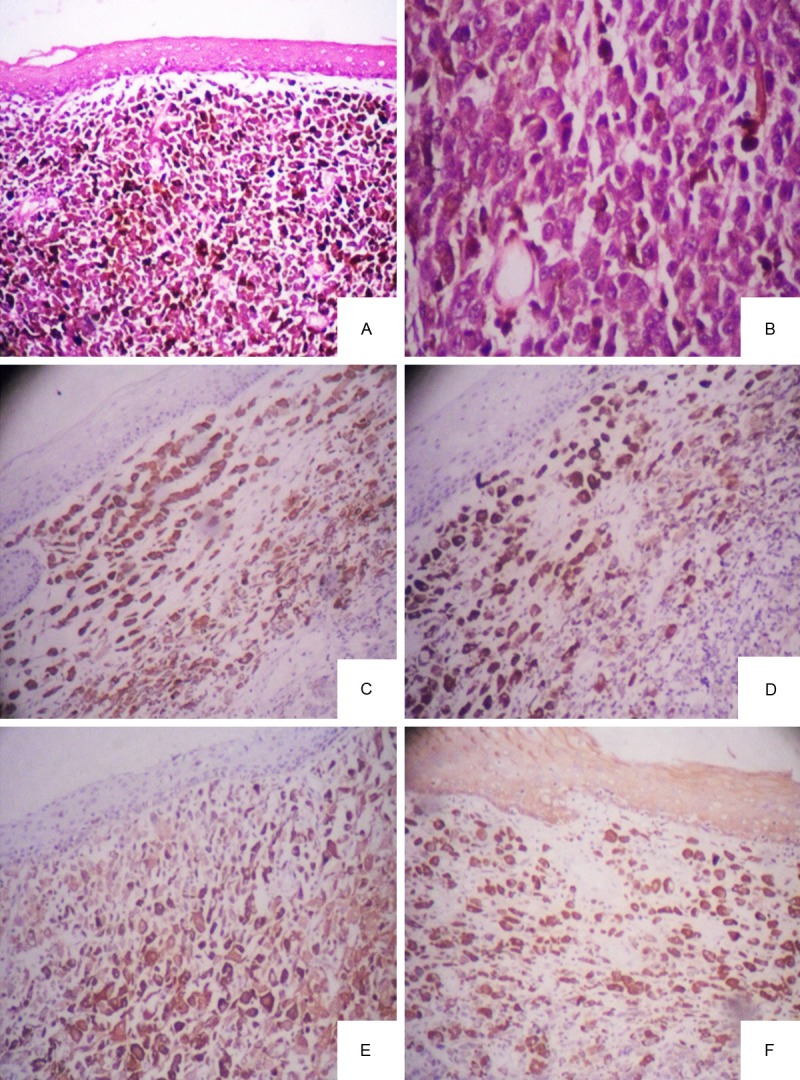
A. Low power microscopy showed the tumor cells extended downward from the epithelium, melanin deposition (H&E ×40); B. High power microscopy showed tumor cells presented spindle-shapes with abundant cytoplasm, remarkable red nucleoli (H&E ×100); C. Tumor cells were positive to HMB-45; D. Tumor cells were positive to Melan-A; E. Tumor cells were positive to S-100 protein; F. Tumor cells and overlying epithelium were both positive to cytokeratin (CK) pan.
Discussions
Most of malignant melanomas have been detected in skins. Primary malignant melanoma of esophagus (PMME) is a rare but highly aggressive neoplasm, with an incidence less than 0.2% of all primary esophageal neoplasms [1]. A comprehensive computerized (PubMed/Medline) review of the world literature was carried out, there were 337 cases ever published in total [2]. Most of them were individual case reports.
The tumor generally occurs in the sixth and seventh decades of life, with a male-to-female ratio of 2:1 [3]. Almost 86% of PMME locate at the lower two-thirds of esophagus [4]. Most of patients would complain about dysphagia, non-specific retrosternal pain, and weight loss, similar to other forms of esophagus cancer. The patients usually endure a symptomatic history of 3.5 months on average before a diagnosis is established [5].
The pathogenesis of PMME is still suspicious. In the middle of the twentieth century, it was thought that there were short of melanoblasts in the esophagus epithelium. Until 1963, de la Pava demonstrated the presence of melanoblasts and granules in the basal layer of esophageal epithelium. They speculated that these melanoblasts migrated from the neural crest and differentiated into melanocytes in the esophageal wall [6].
As usual, a detailed history and clinical examination is important in distinguishing between primary and secondary disease. Other organs of primary malignant melanoma must be excluded before the diagnosis is made [7]. In this case, examinations have been done that there was no evidence of cutaneous or ocular and mucosal primary melanoma at the same time, also demonstrated the tumor was primary rather than secondary.
The diagnosis of malignant melanoma may be difficult in surgery pathology, because of its great variability on histological appearance. IHC is helpful in the diagnosis of PMME. Histology and IHC alone have limitations due to the wide differential diagnoses for PMME, specially the tumor with few or no melanin granules. If that, it may be difficult to recognize as melanoma. Originally, S-100 protein was used for diagnosing melanoma [8]. Afterwards, HMB-45 was found more specific for melanoma, because it indicated active melanosome formation [9]. Melan-A was another immunohistochemical marker, which was positive in small percentage of HMB-45 negative melanomas [10]. As for cytokeratin, in the literature reviewed, it was reported that the rate of positivity with cytokeratin was 7% [11]. S-100 seemed the most sensitive marker for melanoma, while HMB-45 and Melan-A demonstrated relatively good specificity but not as good sensitivity as S-100 [12]. The combination of these antibodies could improve the accuracy of diagnosis.
Because initial symptoms are nonspecific, the patients are usually diagnosed at a late stage. Haematogenic and lymphogenic metastases are common. According to reports in the literature, the most common metastasis organ is the liver (31%), followed by mediastinum (29%), lung (18%), brain (13%) and other intra-abdominal organs [4].
The prognosis of PMME is extremely poor. In most of cases, the patients are usually diagnosed at a late stage, 30-40% of them have metastases at the same time, and 5-year survival rate is approximately 4.2% [13]. Nowadays, treatment protocols are not well established. Surgical resection should be the first choice of treatment when patients have no distal metastases or extensive lymph node enlargement [14]. At present, adjuvant therapy includes, chemotherapy, radiotherapy and immunomodulatory therapy, while the curative effect seems disappointed. They may play a palliative role when the patient is in the poor functional condition [15]. Some authors have reported disease control after administration of chemoradiotherapy, there are no definitive data about the effect of postoperative chemotherapy or radiotherapy on overall 5 year survival [16]. In this case, the patient with PMME treated by surgical resection. Till now, the patient is still alive for 5 months without any chemotherapy, radiotherapy and immunomodulatory therapy.
In conclusion, PMME is a rare but highly aggressive tumor. The diagnosis of PMME should combine with clinical symptoms, auxiliary examination, pathological examination and immunohistochemistry. The problem of early detection, exact diagnosis and effective treatment still a challenge.
Disclosure of conflict of interest
None.
References
- 1.Yano M, Shiozaki H, Murata A, Inoue M, Tamura S, Taniguchi M, Monden M. Primary malignant melanoma of the esophagus associated with adenocarcinoma of the lung. Surg Today. 1998;28:405–8. doi: 10.1007/s005950050150. [DOI] [PubMed] [Google Scholar]
- 2.Bisceglia M, Perri F, Tucci A, Tardio M, Panniello G, Vita G, Pasquinelli G. Primary malignant melanoma of the esophagus: a clinicopathologic study of a case with comprehensive literature review. Adv Anat Pathol. 2011;18:235–52. doi: 10.1097/PAP.0b013e318216b99b. [DOI] [PubMed] [Google Scholar]
- 3.Volpin E, Sauvanet A, Couvelard A, Belghiti J. Primary malignant melanoma of the esophagus: a case report and review of the literature. Dis Esophagus. 2002;15:244–49. doi: 10.1046/j.1442-2050.2002.00237.x. [DOI] [PubMed] [Google Scholar]
- 4.Chalkiadakis G, Wihlm JM, Morand G, Weill-Bousson M, Witz JP. Primary Malignant Melanoma of the Esophagus. Ann Thorac Surg. 1985;39:472–5. doi: 10.1016/s0003-4975(10)61963-7. [DOI] [PubMed] [Google Scholar]
- 5.Sabanathan S, Eng J. Primary malignant melanoma of the esophagus. Scand J Thorac Cardiovasc Surg. 1990;24:83–5. doi: 10.3109/14017439009101830. [DOI] [PubMed] [Google Scholar]
- 6.De la Pava S, Nigogosyan G, Pickren JW, Cabrera A. Melanosis of the esophagus. Cancer. 1963;16:48–50. doi: 10.1002/1097-0142(196301)16:1<48::aid-cncr2820160107>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 7.Sabanathan S, Eng J, Pradhan GN. Primary malignant melanoma of the esophagus. Am J Gastroenterol. 1989;84:1475–81. [PubMed] [Google Scholar]
- 8.Yu HC, Ketabchi M. Detection of malignant melanoma of the uterine cervix from Papanicolaou smears. A case report. Acta Cytol. 1987;31:73–6. [PubMed] [Google Scholar]
- 9.Skelton HG 3rd, Smith KJ, Barrett TL, Lupton GP, Graham JH. HMB-45 staining in benign and malignant melanocytic lesions. A reflection of cellular activation. Am J Dermatopathol. 1991;13:543–50. doi: 10.1097/00000372-199113060-00004. [DOI] [PubMed] [Google Scholar]
- 10.An J, Li B, Wu L, Lu H, Li N. Primary malignant amelanotic melanoma of the female genital tract: report of two cases and review of literature. Melanoma Res. 2009;19:267–70. doi: 10.1097/CMR.0b013e32831993de. [DOI] [PubMed] [Google Scholar]
- 11.Bishop PW, Menasce LP, Yates AJ, Win NA, Banerjee SS. An immunophenotypic survey of malignant melanomas. Histopathology. 1993;23:159–66. doi: 10.1111/j.1365-2559.1993.tb00474.x. [DOI] [PubMed] [Google Scholar]
- 12.Ohsie SJ, Sarantopoulos GP, Cochran AJ, Binder SW. Immunohistochemical characteristics of melanoma. J Cutan Pathol. 2008;35:433–44. doi: 10.1111/j.1600-0560.2007.00891.x. [DOI] [PubMed] [Google Scholar]
- 13.Simpson NS, Spence RA, Biggart JD, Cameron CH. Primary malignant melanoma of the oesophagus. J Clin Path. 1990;43:82–3. doi: 10.1136/jcp.43.1.82-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lin CY, Cheng YL, Huang WH, Lee SC. Primary malignant melanoma of the esophagus: a study of clinical features, pathology, management and prognosis. Dis Esophagus. 2011;24:109–13. doi: 10.1111/j.1442-2050.2010.01111.x. [DOI] [PubMed] [Google Scholar]
- 15.Lin CY, Cheng YL, Huang WH, Lee SC. Primary malignant melanoma of the oesophagus presenting with massive melena and hypovolemic shock. ANZ J Surg. 2002;72:62–4. doi: 10.1046/j.1445-2197.2002.02297.x. [DOI] [PubMed] [Google Scholar]
- 16.Kranzfelder M, Seidl S, Dobritz M, Brücher BL. Amelanotic esophageal malignant melanoma: case report and short review of the literature. Case Rep Gastroenterol. 2008:224–31. doi: 10.1159/000137376. [DOI] [PMC free article] [PubMed] [Google Scholar]