

ABSTRACT
Introduction:
Pneumonia is the most serious inflammatory disease of the respiratory system and also the most common infectious disease. Even now, in the 21st century, pneumonia occupies a prominent place in clinical medicine and public health. We are confronted daily with the increased number of patients, as well as the constant increase in annual mortality due to this infectious disease.
Goal:
The goal was to investigate the prevalence and pneumonia characteristics as the most serious lower respiratory tract infection, the incidence of typical and atypical pneumonia, hospitalization duration of the patients at the Clinic of Infectious Diseases, Clinical Center of Sarajevo University CCUS.
Patients and Methods:
From January 2011 until December 2012 the study involved 100 hospitalized patients with infections of the lower respiratory tract at the Clinic of Infectious Diseases CCUS.
Results:
Among the most common infections the pneumonia is highly represented. Lung X-Ray in two planes, by all protocols, demonstrated with the auscultatory finding has the highest value in the diagnosis of clinical pneumonieae. A statistically significant difference among our hospitalized patients, compared to typical and atypical pneumonia, is in favor of the first–typical bacterial pneumonia. Hospitalization duration ranges between 7-14 days.
Conclusion:
We believe that the introduction of the pneumococcal vaccine (PCV) should reduce the number of pneumonia caused by this bacterium. Recommendations for its use also come from the WHO. Until December 2012, WHO added 86 states in the PCV immunization as a part of their national immunization programs. Pneumococcal conjugate vaccine (PCV) is safe and effective for the reduction in number of patients suffering from pneumonia caused by St. pneumoniae. In particular, the vaccine is a significant protection for children, who due to age and severity of the disease must remain under medical supervision. In elderly vaccine is important and useful as preventive measure, due to their biological characteristics and life circumstances which mark this group as vulnerable population, like the youngest, and can be fatal for them.
Keywords: pneumonia, increased mortality, vaccine
NTRODUCTION
Pneumonia is an acute, potentially severe disease with the rapid development of a number of symptoms and complications so it represents an important cause of morbidity and mortality, especially in older people with chronic diseases (1,2). Pneumonia is now classified into three groups according to the location and cause of the occurrence into:
Community-acquired pneumonia;
Hospital acquired (nosocomial) pneumonia;
Pneumonia in patients with impaired immunity.
Epidemiologic causes
The most important bacterial cause of community-acquired pneumonia is Streptococcus pneumoniae, which is responsible for 80% of cases and is represented in all age groups (5,6,7). Out of 82 Streptococcus pneumoniae serotypes the disease is caused by nine (1, 3, 4, 5, 7, 8, 9, 10 and 12), while the most severe clinical presentation causes serotype 3 (2).
By frequency it is followed by Haemophilus influenza, which is the second most important bacterial pathogen in the incidence of pneumonia and other gram-negative bacteria, Staphylococcus aureus and anaerobic bacteria. Gram–negative bacteria, like H. influenza, Moraxella catarrhalis and Klebsiella pneumoniae cause pneumonia in people with weakened resistance, in newborns, infants and the elderly who are chronically ill. The hospital treatment of pneumonia is almost obligatory for bacterial origin (St. aureus, followed by Legionella and anaerobic bacteria and rarely pneumococcus).
The most important cause of atypical pneumonia is Mycoplasma pneumoniae, besides which we are facing other two Chlamydia psittaci, the causative agent of psittacosis and Coxiella burnetii, the cause of Q fever. The microorganisms that cause pneumonia enters the lung in 4 ways: by inhalation of infected aerosols, nasopharyngeal aspiration from the oral cavity, hematogenous spreading of inflammatory foci, and direct expansion from the adjacent organs. The causes of atypical pneumonia, but also the bacteria enter the lungs by inhalation of infected aerosols, while other three modes are reserved for spread of bacteria (5, 6).
1.1. Clinical presentation
The main clinical symptoms of pneumonia are fever and cough, with or without sputum, accompanying by stabbing pain in the chest and shortness of breath. However these two parameters are not always present. Bacterial pneumonia, especially caused by pneumococcus, has sudden onset of symptoms. The body temperature is moderately high or very high, accompanied with chills. Fever is accompanied with tachycardia and increase in respiratory frequency. In case of the classical bacterial pneumonia also occurs productive cough. Sputum is purulent and may contain blood. Relatively often chest pain, pleural effusion and dyspnea are present. Stabbing chest pain symptoms are very important for the diagnosis of pneumonia. Characteristic physical examination finding: examination reveals flushed face, dry skin with pronounced turgid. Tachycardia and cyanosis may be present as a result of hypoxia but also the cardiovascular failure. Auscultation of the lungs is not safe diagnostic parameter and should be confirmed with the X-ray. In the developed bacterial pneumonia auscultation finding have signs of bronchial breathing and appearance of crepitations, also sometimes can be heard pleural friction. However, at the early stage of the disease only vesicular breathing is found is found. Many crecipitation sounds and moist rales which indicate exudation in the alveoli.
Atypical pneumonia have less boisterous clinical image, because the clinical symptoms develop gradually. The body temperature rises up to high values, but it is rarely accompanied with chills. A common finding is also bradycardia. Clinical picture besides fever prevails general symptoms (headache, muscle aches, fatigue, malaise, loss of appetite). Cough is usually observed after 3-6 days and it is dry with irritation. Specific is the discrepancy between normal or small auscultation findings and X-ray clearly expressed pneumotic infiltrates (1,2).
1.2. Diagnosis
Diagnosis and treatment of pneumonia is still a big problem in everyday medical practice, which affects the clinician in the hospitals, and even more the general practitioners in case of outpatient diagnosis and treatment of pneumonia. There are many difficulties and shortcomings in reaching the final etiological diagnosis and the proper procedure. Results of bacteriological evaluation of various samples are known only after few days. That is why today, and will continue in the future, most pneumonia are treated without determined causative agent. Diagnostic sequence for pneumonia includes the following: clinical assessment (history, clinical status, particularly physical findings on the lungs), x-ray, laboratory and microbiological diagnostics (2,5,7,8).
1.3. Treatment
Penicillin has until recently been the main antibiotic in treatment of primary bacterial community-acquired pneumonia, but due to the high resistance on penicillin in the treatment of pneumonia today are mostly used oral cephalosporins and macrolides in the treatment of minor or moderate form of primary pneumonia, especially in out-patient settings. In case of hospitalized patients is administered penicillin G or more usually cephalosporins from 2nd or 3rd generation. It is important to emphasize that azithromycin in comparison to erythromycin has better effect against Haemophilus influenza. It is a unique antibiotic by shortness of application. The causes of atypical pneumonia are located intracellularly, so they are not affected by beta-lactam antibiotics and aminoglycosides. Against them are effective antibiotics from tetracycline and macrolides group (2,10,13).
2. GOAL
To investigate the incidence and characteristics of pneumonia as the most serious lower respiratory tract infection, the incidence of typical and atypical pneumonia and hospitalization duration of patients at the Clinic of Infectious Diseases CCUS.
3. MATERIAL AND METHODS
This retrospective-prospective study included 100 patients with lower respiratory tract infections hospitalized at in Clinic of Infectious Disease, Clinical Center of Sarajevo University. The study was conducted in the period from January 2011 until December 2012. It included patients suffering from infection of the lower respiratory system at all ages. As data source are used medical records of hospitalized patients with lower respiratory tract infections, which are treated in the Clinic of Infectious Diseases. Criteria for inclusion in this study were physical findings and clinical symptoms in favor of infection and X-ray finding with lung infiltration, increased parameters of laboratory parameters suggestive of infection of the lower respiratory tract, while the criteria for exclusion from the study were patients with PA X-ray of the lungs with infiltrations that by differential diagnosis does not correspond to infections of the lower respiratory tract.
4. METHODS
The diagnosis is based on: clinical evaluation (medical history, clinical status, particularly physical findings of the lungs), X-ray of the lungs, laboratory and microbiological diagnostics. From history data analysis included leading clinical symptoms due to which the patient was admitted at the Clinic of Infectious Diseases CCUS (fever, cough, sputum, shortness of breath, shivering, fatigue). From clinical findings we analyzed age, gender and local auscultatory findings which was different in case of infections in the lower respiratory tract. In case of developed bacterial pneumonia auscultatory finding is characterized by bronchial breathing and appearance of crepitation, while occasionally can also be heard pleural friction. However, at the beginning of the disease only weakened vesicular breathing can be heard. In case of atypical pneumonia findings in the lungs at the beginning of the disease was generally normal, while later can be noticed crepitation and high frequency noise at the end of inhalation. From laboratory parameters were analyzed following biochemical parameters: erythrocyte sedimentation rate, blood count and hematocrit, differential blood count (mostly focused on neutrophils), C-reactive protein, X-ray findings (the majority of patients with infections of the lower respiratory tract had a standard PA and left lateral chest X-ray on which can be seen various pulmonary infiltrations and the remaining patients had normal X-ray of lungs) and microbiological analysis (analysis of the nose and throat swabs, sputum smear). All the above tests were performed at the Clinic of Infectious Diseases, Clinic of Radiology, Institute of Microbiology and the Department of Pulmonary Diseases CCUS.
5. RESULTS
Between January 2011 and December 2012 analysis involved 100 hospitalized patients with infections of the lower respiratory tract from the Clinic of Infectious Diseases CCUS. In relation to the total number of patients pneumonia was present in 79 (79%) cases, more among men 62.025% then among women 37.97%. The most common age group in our study was over 65 years of age, and the pneumonia occurred the least among patients at age from 25-44 years.
Figure 1 shows the incidence of infections of the lower respiratory tract, of which the largest number represented pneumonia with 79%. Next by the frequency is acute bronchitis with 10%, chronic obstructive pulmonary disease (COPD) with 7%, while chronic bronchitis was present in only 4%.
Figure 1.
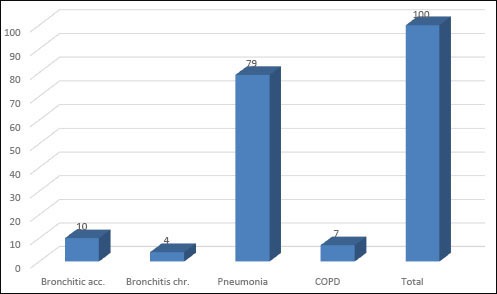
The incidence of infections of the lower respiratory tract
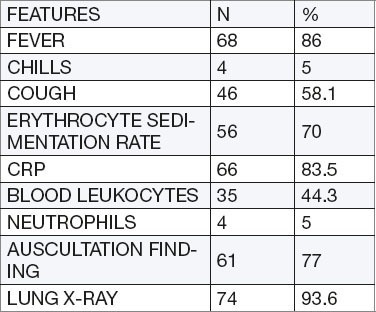
In patients with pneumonia are the most common is characteristic X-ray of the lung represented in 93.6% and auscultatory pathological findings of the lungs in 77%. From clinical symptoms follows fever with 86%, cough 58.1% and shivering with 5%. Among laboratory parameters dominated the pathological CRP (C-reactive protein) 83.5%, erythrocyte sedimentation rate (SE) 70%, leukocytes count 44.3% and 5% neutrophils (Table 1).
Table 1.
Characteristics of the pneumonia
X-ray of the lungs in two planes in all the protocols has a key value for clinical diagnosis of the pneumonia. It gives a decisive answer to the question “which part of the respiratory system is affected by inflammation?” In our research, we found that X-ray of the lung was the most common pathological characteristic among the patients.
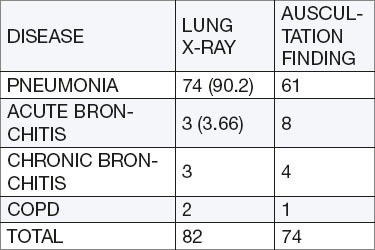
During the analysis of the lung X-ray was observed that in the group of patients with infections of the lower respiratory tract most common disease is the pneumonia with 74%, followed by acute and chronic bronchitis with 3% and 2% with COPD. Similar data were obtained during auscultatory examination, where pneumonia was the most common with 61%, followed by acute bronchitis.
When analyzing the relationship of auscultation findings and x-ray of the lungs, in all lower respiratory tract infections, was used “t” test (Student) for significance of the difference, which amounted to 0.93 for paired samples (Table 2).
Table 2.
Analysis of the auscultation findings and X-ray of the lungs in case of the lower respiratory tract infections
The incidence of bacterial (typical) and atypical pneumonia was significantly higher in favor of typical with 97.47% (77 patients), whereas atypical were represented only 2.53% (2 cases) as shown in Figure 2. In support of bacterial pneumonias speaks also the parameters of inflammation (erythrocyte sedimentation rate) and CRP (C-reactive protein), which have been elevated. Mean CRP was 107.19 mg/dl and ranged from 6 to 335.3 mg/dl. While sedimentation rate ranged between 11mm/hour and 125 mm/hour with the mean value of 55.05 mm/hour (Figure 3).
Figure 2.
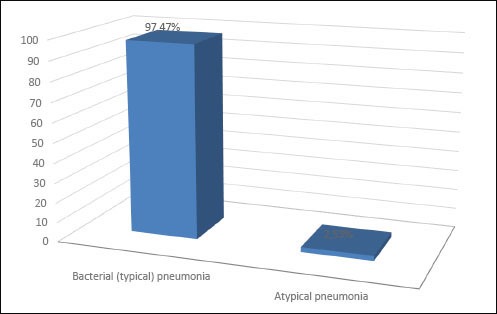
The ratio of typical and atypical pneumonia
Figure 3.
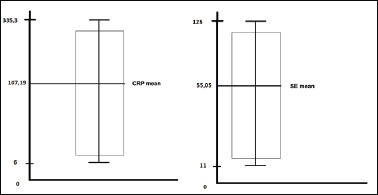
Analysis of inflammation parameters in pneumonia: a) erythrocyte sedimentation rate (SE) and b) C-reactive protein (CRP)
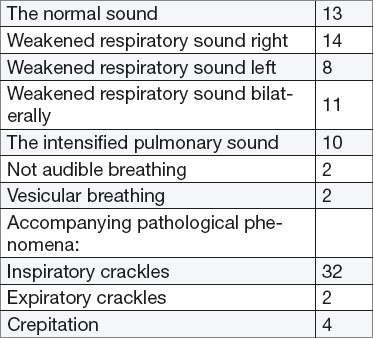
In the study group of patients was evaluated auscultatory findings in the lungs. Weaker breathing on the right side was present in majority of patients 17.72% with concomitant pathological inspiratory crackles 40.50% (Table 3).
Table 3.
Analysis of the auscultation findings of the lungs
In case of patients with pneumonia hospitalization duration in our analysis was most often from 7-14 days and the smallest number of the patients stayed at the clinic up to 6 days (Figure 4).
Figure 4.
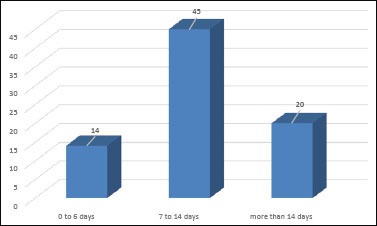
Duration of the hospitalization
6. DISCUSSION
Donowitz and Mandell in their study conducted in the UK showed that pneumonia is responsible for 10 times more deaths than any other infectious disease. While in the U.S. the pneumonia is among the leading causes of death (6,7). In developing countries, infections of the lower respiratory tract are the most common cause of death, especially when it comes to pneumonia as determined by the WHO (World Health Organization). In our research, we reached the similar results that the most common infectious disease of the lower airways is pneumonia. Our study showed a predominance of male patients suffering from pneumonia with 62.025% as also noticed by other authors. Kuzman in his study found that there were more men than women and the ratio is higher in favor of men 1.5:1 (2). Also, all causes of pneumonia are more common in men than in women. One of the several studies conducted by Champam and his associates suggest that adults over 65 get sick more than 915,000 times each year in the USA. They claim that the age is one of the important factors for the development of pneumonia (7). Certainly these data coincide with our research. Berntsson et al. simultaneously examined the ratio of typical and atypical pneumonia in theirs studies and came to the fact that bacterial pneumonia are more common in hospitalized patients then atypical because such patients are hospitalized because of severe symptoms and complications. It is evident that our results coincide with the results of authors dealing with the same topic. A statistically significant difference is found among our hospitalized patients between typical and atypical pneumonia in favor of the first–typical bacterial pneumonia. In our study, the mean value of C–reactive protein (CRP) in patients with pneumonia who had elevated levels amounted to 107.19 mg/dL. Lehtomäki and associates in their research found the average value of CRP that was 149 mg/dL, with 90% of bacterial pneumonia, which is similar to results of our research (15) Kuzman et al. found high mean value of 232.1 mg/dL in bacterial and 132.6 in case of atypical pneumonia (1). Kerttula et al. in their study of pneumonia in hospitalized patients found the mean value of C-reactive protein, which amounted to 164 mg/dL in bacterial and 51 mg/dL in atypical (14). Like our results, Holmberg and colleagues found that in bacterial pneumonias the mean value of the sedimentation was 57 mm/hour (13). Unlike Harambasic and collaborators who conducted two large studies and shown that pneumonia is more often present in lower than in the upper parts and that there are no major differences in the involvement of the left and right lung (16). Research by Fill and Mandell showed that pneumonia without complications and without major associated chronic diseases should be treated for 7-10 days, with a tendency of shortening of this period (6,11).
7. CONCLUSIONS
Among infections of the lower respiratory tract at the Clinic of Infectious Disease CCUS most often is present pneumonia. This information should be taken seriously, whereby we must seriously reflect on the WHO report and the fact that in some countries, pneumonia is responsible for 10 times more deaths than any other infectious disease. Infections of the lower respiratory tract are more present in male population. A statistically significant difference in our hospitalized patients sample was found in comparison of typical and atypical pneumonia, in favor of the first-typical bacterial pneumonia. Hospitalization duration ranged between 7-14 days.
We believe that the introduction of the pneumococcal vaccine (PCV) will reduce the number of pneumonias caused by this bacterium. Recommendations for their use are also set by the WHO. By December 2012, 86 WHO member states has added the PCV in the immunization protocol in their national immunization programs. Pneumococcal conjugate vaccine (PCV) is safe and effective in the reduction of number of suffering from pneumonia caused by St. pneumoniae. In particular, the vaccine is a significant protection to children, who regarding their age and severity of the disease must remain under medical supervision. Also, in elderly vaccine is important and useful preventive measure, because of their biological characteristics and life circumstances put this group in vulnerable population like the youngest, and can be fatal for them.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED
REFERENCES
- 1.Kuzman I. Pneumonije: uzrocnici i dijagnostika. MEDICUS. 2005:71–82. [Google Scholar]
- 2.Kuzman I. Pneumonije. In: Kuzman I, editor. Ur. Pneumonije - uzrocnici, dijagnostika, lijecenje. Zagreb: Medicinska naklada; 1999. pp. 341–382. [Google Scholar]
- 3.Kasper L. Dennis, Braunwald E. Manual of medicine. 16 edition. Vol. 134. USA: 2005. i sur. Harrisons principles of Internal Medicine; pp. 679–685. [Google Scholar]
- 4.Ayres JG. Seasonal pattern of acute bronchitis in general practice in the United Kingdom 1976-1983. Thorax. 1986;41:107–110. doi: 10.1136/thx.41.2.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bosnjak-Petrovic V. Beograd: Peto izdanje; 2009. Interna medicina; pp. 440–450. [Google Scholar]
- 6.Mandell LA, Wunderink RG, Anzueto A. i sur. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):27–72. doi: 10.1086/511159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Champan SW, Bradsher RW, Jr, Campbell GD, Jr, et al. Infectious Diseases Society of America. Practise guidelines for the management of patiens with blastomycosis. Clin Infect Dis. 2000;30:679–683. doi: 10.1086/313750. [DOI] [PubMed] [Google Scholar]
- 8.Donowitz GR, Mandell GL. Acute Pneumonia. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas and Bennett's Principles and Practice of Infectious Diseases. Sixth ed. Philadelphia: Elsevier, Churchill Livingstone; 2005. pp. 819–845. [Google Scholar]
- 9.Monto AS. Epidemiology of viral respiratory infections. Am J Med. 2002;112:4S–12S. doi: 10.1016/s0002-9343(01)01058-0. [DOI] [PubMed] [Google Scholar]
- 10.Hall CB, Hall WJ. Bronchiolitis. In: Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases. 4th ed. New York: Churchill Livingstone; 1995. pp. 612–619. [Google Scholar]
- 11.Bartlett JG. Diagnostic test for etiologic agents of community-acquired pneumonia. Infect Dis Clin North Am. 2004;18:809–827. doi: 10.1016/j.idc.2004.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ball P. Epidemiology and treatment of chronic bronchitis and its exacerbations. Chest. 1995;108(Suppl. 2):43–52. doi: 10.1378/chest.108.2_Supplement.43S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Holmberg H. Community-acquired pneumonia in adults. Curr Opin Infect Dis. 1998;11:147–151. doi: 10.1097/00001432-199804000-00010. [DOI] [PubMed] [Google Scholar]
- 14.Vrhovac B, Francetic I, Jaksic B. Interna medicina. Zagreb; 2003. i sur. [Google Scholar]
- 15.Bohte R, Vanfurth R, Vandenbroek PJ. Aetilogy of community-aquired pneumonia: A prospective study among adults requiring admission to hospital. Thorax. 1995 doi: 10.1136/thx.50.5.543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Harambasic H. B. Vrhovac i sur., ur., Interna Medicina II. Zagreb: Izd. Naprijed; 1997. Akutne upale pluca; p. 814. [Google Scholar]