

ABSTRACT
Introduction:
Professionalism is essential for the development of mature physicians but not much education is devoted to that theme. Aim: We aimed to determine the views of undergraduate medical students on medical professionalism.
Methods:
This was a qualitative study, based on focus groups of the first and fifth-year undergraduate medical students. Transcripts of the focus groups were independently evaluated by two researches. Segments of transcripts, identified as important, were marked as verbatims. A grounded theory method with open coding was applied. A list of codes was developed and reviewed by both researchers until the consensus was reached. Then, the codes were reviewed and put into the categories and dimensions.
Results:
Students recognized 10 main medical professionalism dimensions (empathy, respect, responsibility, autonomy, trust, communication, difference between professional and private life, team work, partnership) and two dimensions associated with it (physician's characteristics, external factors). Slight change of the attitudes towards a more self-centred future physicians’ figure was observed in the fifth-year medical students.
Conclusion:
The students have an appropriate picture of the physicians’ figure even at the beginning of their medical studies but still needs an education in professionalism. It seems that the fifth-year students perceive physicians as more self-centred when compared to their first-year colleagues.
Keywords: medical ethics, medical students, qualitative study
1. INTRODUCTION
In the era of sophisticated medical technology, family physicians should use technological advances but continue to practice comprehensive medicine in spite of health policy demands for more focus on public than individual outcomes (1). Consequently, the medical professionalism is slowly finding its way back to medical education (2-5). It is widely acknowledged that medical professionalism can be learned and taught (3, 6-9). However, usually it is a part of a so called hidden curriculum: it is incorporated into teaching different subjects without setting clear learning objectives (10). There are voices that medical students besides communication skills, team work, practice organization, and knowledge management also should be taught in humanism, accountability and altruism (11). However, not much is known about the role of medical education in building a future physician who will possess the appropriate professional values, attitudes and behaviors (12). Even a unifying theoretical or practical model to use as a format for developing a professionalism teaching curriculum does not exist yet (13).
There is neither an unified definition nor theoretical model of medical professionalism at the moment (14). The American Board of Internal Medicine suggested that professionalism has six components: altruism, accountability, excellence, duty, honour/integrity and respect (15). A model from USA and Europe declared that professionalism consists of three fundamental principles (patient welfare, patient autonomy and social justice) with ten professional responsibilities (16). The model from UK suggests that medical professionalism consists of integrity, compassion, altruism, continuous improvement, excellence and working in partnership with team members (17).
So far, several studies have tried to determine the views of undergraduate medical student regarding the professionalism (18-23). They showed that undergraduate students in general have a clear perception of what medical professionalism was. On the other hand, a recent qualitative study from Australia showed that undergraduate students have had some difficulties with perceiving what a professional physician was; they differentiated between the term “good” doctor and professional doctor as they perceived professionalism as an external and imposed construct (21). It also seems that some differences exist regarding the perceptions of medical professionalism in undergraduate students of different study years. Students in higher years of education reported the decline of professionalism in terms of idealism, empathy, the perception of physicians’ status and income and the rise of the negative views on primary care and the importance of lifestyle and family (6, 19, 24, 25). This change of attitudes seems to be largely dependent on the curriculum and the teaching method applied. The shift from informal to formal teaching of professionalism resulted in higher sensitivity to professionalism (19) and the early patient contact and small groups in professionalism enhanced the understanding of professionalism (7).
Medical faculty Maribor is a young faculty which was established in 2003. The study of medicine lasts for six years and is consistent with the Bologna principles. No formal subject in the undergraduate study is devoted to professionalism therefore we can say that professionalism is a part of a hidden curriculum.
2. GOAL
The aim of this study was to determine the views of undergraduate medical students on medical professionalism and recognise any potential qualitative differences in their views according to the study year.
3. METHODS
3.1. Study design and settings
This was a qualitative study, based on focus groups. It took part on the Faculty of Medicine in Maribor, Slovenia and was performed in June 2014. The study was approved by the National Ethics Board (No. 226/09/13).
3.2. Participants and focus groups
The first and fifth-year undergraduate medical students took part in this study. They were recruited by the researchers through the personal contact. In the study year 2013/2014, there were 89 students in the first year and 90 students in the fifth year.
The students were included in two focus groups. The first one consisted of the five first-year medical students (three women and two men), each 19 years old. The second one consisted of seven fifth-year medical students (two men and five women), each 23 years old. Both focus groups were moderated by one of the researchers (HV) and observed by the second researcher (ZKK). The focus groups participants discussed upon the several questions (Box 1).
Box 1.
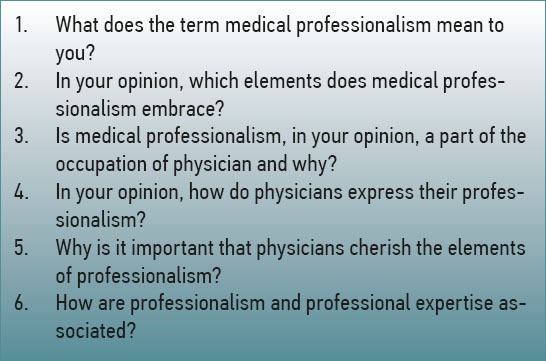
The questions discussed in focus groups
Focus groups were audio-recorded. Oral informed consent was sought from the participants prior to the session.
3.3. Analysis
The interviews were typed to word documents. Transcripts were independently evaluated by both researches (HV and ZKK). Segments of transcripts, identified as important, were marked as verbatim. A grounded theory method with open coding was applied. A list of codes was developed and reviewed by both researchers until the consensus was reached. Then, the codes were reviewed and put into the categories and dimensions.
4. RESULTS
Students recognized 10 main medical professionalism dimensions (Table 1) and two dimensions associated with it (Table 2).
4.1. Objectivity
Students of both study years expressed the importance of setting a clear line between objectivity and subjectivity in order not to let the subjective feelings influence the management of the patients.
“The sympathy towards a patient should not blur your professional objectivity.” (Fifth-year female student)
“…exactly here…in the attitude towards the patient…to set the line between subjective and objective.” (First-year female student)
4.2. Empathy
First-year students perceived empathy as something you could learn but not in order to really become an empathic person but in to make an impression that you are an empathic person.
“I think it is important that the physicians do not feel sorry for the patient as their primary goal is to cure the patients” (First-year female student)
“I think it is important to ask the patients how they are feeling. Not because you are really interested but to show them that you care. (First-year female student)
“…(empathy) is learned not innate…you can act that you care for someone but you really don’t.” (First-year male student)
Fifth-year students were more concerned with how to draw a line between being too empathic and being not empathic at all.
“It is necessary to find a healthy line between taking the emotional stuff home and not being able to sleep and between being a misanthrope and a cold person.” (Fifth-year female student)
“Not only that we write in the patient's record that we will keep him for another week in the hospital because he has nowhere to go but also to understand his situation and to adjust the management and communication.” (Fifth-year male student)
4.3. Respect
Students of both study years recognized the importance of a respectful relationship towards coworkers and patients.
“I cannot imagine the relationship my colleague will have towards patients if he is not able to say hi to me when we meet even though he has been my classmate for the last five years. ” (Fifth-year female student)
“To show respect to the patients by addressing them with sir or madam.” (First-year female student)
4.4. Responsibility
Students expressed the need for responsibility in form of continuous professional education and being able to recognize your limits.
“…to engage in continuous education, to try to follow guidelines, not to rest on laureates.” (Fifth-year female student)
“…being responsible to your patients in a way to be able to help them as much as you can.” (Fifth-year female student)
“If the physician does not know what is wrong with you he refers you to other physicians.” (First-year female student)
4.5. Autonomy
The first-year students perceived autonomy as the right of patients to make their own decisions and also as their obligation for taking more responsibility. The fifth-year students referred also to the autonomy of the physicians.
“I think that nowadays patients have way to much autonomy and very little responsibility and this is not right.” (First-year female student)
“…that you do not let the patient to control you i.e. to tell you which drug to prescribe, to set this line.” (Fifth-year female student)
“That the explanatory duty/informed consent does not become some kind of a blackmail and a form of persuasion that your truth is the only truth for this patient but that you only try to explain and present different treatment options.” (Fifth-year female student)
4.6. Trust
The students agreed that trust and confidentiality were essential parts of medical professionalism.
“I perceive professionalism as the relationship where patient's problems stay between you and him. That you do not talk about them outside your office.” (First-year male student)
“You have to gain confidence, that he trust you, that your knowledge is sufficient and he can put his health into your hands.” (First-year female student)
Communication
Students perceived communication as an essential part of professionalism practice. They considered that patient should understand physician and also physician should understand patient.
“It is important to now that nowadays patients read a lot and then they can mislead their physician that they understand something but they really don’t. They just talk about something they’ve read somewhere and do not understand it.” (Fifth-year female student)
“I think that medicine has become a service activity ad people seek service when they go to the doctor. They sometimes forget how good it felt when physicians took the time and listened to them.” (Fifth-year male student)
“Professionalism is being able to communicate in such a way that the patient understands you. If he comes from low social class you communicate in a more lay language and if he comes from a high class you can communicate in a more sophisticate way.” (First-year male student)
Difference between professional and private life
The students recognized the importance of drawing the line between professional and private life. First-year students were very strict about it, whereas fifth-year students allowed the possibility to do so but being aware of the consequences.
“…if you take this home as a luggage then this can limit your ability to perform your work. Which also affects the patients.” (Fifth-year female student)
“When you come home you must leave your work at work. There is no other way.” (First-year female student)
4.7. Team work
Team work as a part of professionalism was only recognized by fifth-year students.
“…meaning that there is not any gossiping and malicious imputation in the team so you can focus on work. This is what patients deserve.” (Fifth-year male student)
“For example, the patients can see if there are some disputes within the team and this is a sign for them that they will not receive a quality management.” (Fifth-year female student)
4.8. Partnership
Partner relationship with patients was only recognized by fifth-year students.
“That you do not give the patient the feeling that he has no clue and that you do not place yourself above him.” (Fifth-year female student)
“I think that the patient has to feel as he has the possibility to participate in the decisions but that is our duty to present out professional opinion in such a way that he will agree with it and still think that it was solely his decision.” (Fifth-year female student)
4.9. Physician's characteristics
Physician's personality
Students perceived the personality of the physician to be an important part of professionalism. However, they thought it was greatly a matter of family patterns.
“I think that this is a thing that people bring it from their childhood, from their families.” (Fifth-year female student)
“Some people always ignore those who for example fall on the street while others always stop and help. This is not something you could learn.” (Fifth-year female student)
“Professionalism largely depends on the personality. Some are more collegial and help their colleagues even now and lend them their notes while others keep the things to themselves. You know that they will be like that with their patients — they will not be willing to listen to anybody or to recognize their mistakes.” (First-year male student)
Role modelling
This was recognized only by fifth-year students.
“To be a good mentor to students and trainees and others you ought to educate. Nowadays, many are involved in the education process as teachers but they fail to remember that.” (Fifth-year male student)
Expertise
Students perceived expertise to be a part of medical professionalism but not necessary a positive part.
“Someone can be a great expert but has a very low professional relationship towards patients.” (Fifth-year female student)
“I think that there are also doctors who are not very professional but are great experts. They can diagnose a patient very good but are not considered to be good doctors by patients.” (First-year female student)
4.10. External factors
Education
According to fifth-year students, professionalism can be learned and the education system can affect it, especially in a negative way.
“I think that professionalism or at least one part of it, can be learned.” (Fifth-year male student)
“I think that the medical profession can soon become inhuman. So, the humanistic part of it should be constantly a part of education. Otherwise, we can quickly start regarding patients as objects and not humans.” (Fifth-year male student)
“I think that you change a lot during your study. You start to hate people.” (Fifth-year female student)
Health care system
Students regarded health care system as an obstacle to professionalism.
“The problem is the health care system itself. You do not have time to engage in a humanistic and professional relationship.” (Fifth-year female student)
“I still think that the health care system made the people to perceive the health care workers as their slaves or as salesmen in the store – they expect to get some kind of drug each time they go to the doctor.” (First-year female student)
5. DISCUSSION
Students in this study recognized the majority of professionalism components as recognized in several theoretical models (15-17). The also recognized some external and internal factors that were associated with or could in their opinion affect the medical professionalism. Although there were no significant differences in the attitudes towards medical professionalism between first-and fifth-year students, a change in the perceptions of the fifth-year medical students was observed in terms of recognizing more professionalism categories and more self-centred perceptions about the physician figure.
As previously stated, there is no unified theoretical model of medical professionalism (14) and it is therefore difficult to relate our results to the theoretical concepts. If we compare the medical professionalism categories recognized by the undergraduate students to the aforementioned theoretical models (Table 1), we can see that the main professionalism components have been recognized: altruism, autonomy, integrity, relationship, empathy and confidentiality. Of course, the wording and the terms of some components are sometimes different but the meaning is similar, i.e. objectivity and responsibility relate to altruism and autonomy relates to integrity. However, the students failed to recognize some professionalism components, i.e. continuous improvement (17), quality of care, access to care, distribution of finite resources and scientific knowledge (14). If we take a look at some studies that dealt with professionalism attitudes in undergraduate students (20, 22,26), we can see that students recognized a very wide range of professionalism components and some of them are comparable to the categories in our study. For example, five out of seven components reported by Blackall et al (26) were recognized in our study: accountability, altruism, duty, honour and integrity and respect. In another study (20), similar to our study, respect, relationship and partnership were recognized. Yet another study (22) put forward confidentiality – similar to our study. However, the students in our study also recognized empathy, communication, team work and difference between professional and private life which other studies failed to recognize.
Some factors which are not professionalism components but rather relate to professionalism or even affect it were recognized by the students in our study. These were physician's characteristics and external factors (Table 2). These factors act either as facilitators or inhibitors of professionalism. They are also not recognized in the aforementioned theoretical models. However, some of them were recognized in some other studies on students’ attitudes to professionalism, i.e. physician's self-development (20). Also, some of them were recognized in some studies as the possible influences on professionalism (i.e. role modelling) (22, 27,28). In our study, the students recognized the expertise of the physicians to be among possible influential factors whilst in some other studies and/or theoretical models this entity was one of professionalism components (15, 17, 22). In our study, the students also expressed the role of external factors. One of them is the role of education which has already been studies and agreed that professionalism can be learned and taught (3). Also, the students recognized a very important role of the health care system which can have a (mainly) negative influence on professionalism (29).
In this study, some differences were detected between the first-and fifth-year students’ attitudes towards professionalism. First of all, some categories were recognized only by the fifth-year students: teamwork, partnership, role modelling and education. It seems that students do learn about professionalism through their medical studies. Also, they seem to grasp the importance of education in developing a figure of a professional physician. Additionally, there were some qualitative differences in perception of several professionalism components. Although the students of both study years recognized empathy as one of the components, first-year students expressed a very pragmatic attitude towards it whereas fifth-year students were concerned about how to cope with too much empathy. Similar findings were reported regarding drawing the line between personal and professional life. Several studies reported on the decline of empathy through the medical studies (24, 25). Although our study was qualitative and hence the differences are hard to detect, our results suggest that the students become more sensible to empathy as they move towards the end of their studies. Based on the results of our study, we cannot claim that they become more or less empathic; we can only say that they become aware of potential harm empathy could have on their personal lives. This finding relates also to the finding about the autonomy. Namely, the fifth-year students also recognized the autonomy of the physician not only of the patient.
The finding that the first-year students recognized the majority of the professionalism components points to the fact that the students have an appropriate picture of the physicians’ figure even at the beginning of their medical studies. The finding that the fifth-year students recognized more components then their first-year colleagues confirms the need for professionalism education. A slight change of the attitudes detected in our study might point to the development of a more self-centred future physicians’ figure which is also consistent with other studies (6, 24,25). There is a need for quantitative prospective studies which will evaluate these qualitative findings and critically assess the role of education.
This study had a qualitative methodology which was appropriate for determination of the attitudes but less appropriate for the evaluation of differences between first-and fifth-year medical students. With qualitative methodology, we cannot detect quantitative differences in attitudes but only the substantive differences. However, the study gave us the insight to the attitudes of students towards professionalism and will serve for the development of a quantitative tool for measuring these attitudes.
6. CONCLUSION
The students seem to have an appropriate picture of the physicians’ figure even at the beginning of their medical studies. It seems that the fifth-year students perceive physicians as more self-centred when compared to their first-year colleagues. Therefore, an education on professionalism is essential also at the undergraduate level. Further studies are needed to assess the differences in attitudes among medical students in different study years.
Acknowledgments
We thank all students who participated in the study. We also thank professor Janko Kersnik, assistant professor Davorina Petek and assistant professor Polona Selič for their valuable advice. This study was partially supported by unrestricted programme grant from Slovenian National Research Agency P3 0339.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Kersnik J. Learning and teaching to educate future GPs. Eur J Gen Pract. 2012;18(4):199–200. doi: 10.3109/13814788.2012.742060. [DOI] [PubMed] [Google Scholar]
- 2.Mueller PS. Incorporating professionalism into medical education: the Mayo Clinic experience. Keio J Med. 2009;58(3):133–143. doi: 10.2302/kjm.58.133. [DOI] [PubMed] [Google Scholar]
- 3.Hilton S. Education and the changing face of medical professionalism: from priest to mountain guide? Br J Gen Pract. 2008;58(550):353–361. doi: 10.3399/bjgp08X280128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Klemenc-Ketis Z, Kersnik J. Using movies to teach professionalism to medical students. BMC Med Educ. 2011;11:60. doi: 10.1186/1472-6920-11-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Petek-Ster M, Ster B, Petek D, Cedilnik-Gorup E. Validation of Slovenian version of Jefferson scale of empathy for students. Zdrav Var. 2014;53(1):89–100. [Google Scholar]
- 6.Baingana RK, Nakasujja N, Galukande M, Omona K, Mafigiri DK, Sewankambo NK. Learning health professionalism at Makerere University: an exploratory study amongst undergraduate students. BMC Med Educ. 2010;10:76. doi: 10.1186/1472-6920-10-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Monrouxe LV, Rees CE, Hu W. Differences in medical students’ explicit discourses of professionalism: acting, representing, becoming. Med Educ. 2011;45(6):585–602. doi: 10.1111/j.1365-2923.2010.03878.x. [DOI] [PubMed] [Google Scholar]
- 8.Finn G, Garner J, Sawdon M. ‘You’ re judged all the time! ‘Students’ views on professionalism: a multicentre study. Med Educ. 2010;44(8):814–825. doi: 10.1111/j.1365-2923.2010.03743.x. [DOI] [PubMed] [Google Scholar]
- 9.Svab I. Education in medicine. Zdrav Var. 2012;51:225–226. [Google Scholar]
- 10.White CB, Kumagai AK, Ross PT, Fantone JC. A qualitative exploration of how the conflict between the formal and informal curriculum influences student values and behaviors. Acad Med. 2009;84(5):597–603. doi: 10.1097/ACM.0b013e31819fba36. [DOI] [PubMed] [Google Scholar]
- 11.Kersnik J, Wensing M. Improving the quality of care for patients with chronic diseases: what research and education in family medicine can contribute. Eur J Gen Pract. 2012;18(4):238–241. doi: 10.3109/13814788.2012.742059. [DOI] [PubMed] [Google Scholar]
- 12.Daaleman TP, Kinghorn WA, Newton WP, Meador KG. Rethinking professionalism in medical education through formation. Fam Med. 2011;43(5):325–329. [PubMed] [Google Scholar]
- 13.Birden H, Glass N, Wilson I, Harrison M, Usherwood T, Nass D. Teaching professionalism in medical education: a Best Evidence Medical Education (BEME) systematic review. BEME Guide. No. 25. Med Teach. 2013;35(7):e1252–e66. doi: 10.3109/0142159X.2013.789132. [DOI] [PubMed] [Google Scholar]
- 14.Passi V, Doug M, Peile E, Thistlethwaite J, Johnson N. Developing medical professionalism in future doctors: a systematic review. Int J Med Educ. 2010;1:19–29. [Google Scholar]
- 15.Philadelphia: ABIM; 1995. American Board of Internal Medicine Project Professionalism. [Google Scholar]
- 16.Blank L, Kimball H, McDonald W, Merino J. Medical professionalism in the new millennium: a physician charter 15 months later. Ann Intern Med. 2003;138(10):839–841. doi: 10.7326/0003-4819-138-10-200305200-00012. [DOI] [PubMed] [Google Scholar]
- 17.Report of a Working Party of the RCP. London: Royal College of Physicians; 2005. Anon. Doctors in society: Medical professionalism in a changing world. [Google Scholar]
- 18.Kelly M, O’Flynn S, McLachlan J, Sawdon MA. The clinical conscientiousness index: a valid tool for exploring professionalism in the clinical undergraduate setting. Acad Med. 2012;87(9):1218–1224. doi: 10.1097/ACM.0b013e3182628499. [DOI] [PubMed] [Google Scholar]
- 19.Johnston JL, Cupples ME, McGlade KJ, Steele K. Medical students’ attitudes to professionalism: an opportunity for the GP tutor? Educ Prim Care. 2011;22(5):321–327. doi: 10.1080/14739879.2011.11494026. [DOI] [PubMed] [Google Scholar]
- 20.Tsai TC, Lin CH, Harasym PH, Violato C. Students’perception on medical professionalism: the psychometric perspective. Med Teach. 2007;29(2-3):128–134. doi: 10.1080/01421590701310889. [DOI] [PubMed] [Google Scholar]
- 21.Cuesta-Briand B, Auret K, Johnson P, Playford P. ‘A world of difference’: a qualitative study of medical students’ views on professionalism and the ‘good doctor’. BMC Med Educ. 2014;14(1):77. doi: 10.1186/1472-6920-14-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gale-Grant G, Gatter M, Abel P. Developing ideas of professionalism. Clin Teach. 2013;10(3):165–169. doi: 10.1111/j.1743-498X.2012.00643.x. [DOI] [PubMed] [Google Scholar]
- 23.Gillespie C, Paik S, Ark T, Zabar S, Kalet A. Residents’ perceptions of their own professionalism and the professionalism of their learning environment. J Grad Med Educ. 2009;1(2):208–215. doi: 10.4300/JGME-D-09-00018.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Morley CP, Roseamelia C, Smith JA, Villarreal AL. Decline of medical student idealism in the first and second year of medical school: a survey of pre-clinical medical students at one institution. Med Educ Online. 2013;18:21194. doi: 10.3402/meo.v18i0.21194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hojat M, Mangione S, Nasca TJ, et al. An empirical study of decline in empathy in medical school. Med Educ. 2004;38(9):934–41. doi: 10.1111/j.1365-2929.2004.01911.x. [DOI] [PubMed] [Google Scholar]
- 26.Blackall GF, Melnick SA, Shoop GH, et al. Professionalism in medical education: the development and validation of a survey instrument to assess attitudes toward professionalism. Med Teach. 2007;29(2-3):e58–e62. doi: 10.1080/01421590601044984. [DOI] [PubMed] [Google Scholar]
- 27.Byszewski A, Hendelman W, McGuinty C, Moineau G. Wanted: role models – medical students’ perceptions of professionalism. BMC Med Educ. 2012;12:115. doi: 10.1186/1472-6920-12-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Adkoli BV, Al-Umran KU, Al-Sheikh M, Deepak KK, Al-Rubaish AM. Medical students’ perception of professionalism: a qualitative study from Saudi Arabia. Med Teach. 2011;33(10):840–5. doi: 10.3109/0142159X.2010.541535. [DOI] [PubMed] [Google Scholar]
- 29.Relman AS. Medical professionalism in a commercialized health care market. JAMA. 2007;298(22):2668–70. doi: 10.1001/jama.298.22.2668. [DOI] [PubMed] [Google Scholar]