

ABSTRACT
Introduction:
Elimination of stone is determined by size and its localization. Stone from the ureter in 80% of cases can be eliminated spontaneously. If the stone by its characteristics is not spontaneously eliminated, taken are further steps and therapeutic protocols to solve this problem.
Material and methods:
The study was prospective, open and comparative. It was conducted at the Urology Clinic Clinical Center of Sarajevo University in the period from 2007 to 2013. The study included 404 patients with urinary tract lithiasis treated by ESWL. ESWL treatment is performed on the machine Siemens Model Lithostar Multiline, which has a combined ultrasonographic and fluoroscopic display, large energy density in order to obtain optimum focus (without damaging surrounding tissue) and minimal pain that on rare occasions requires for mild sedation-sedation.
Results:
From a total of 404 patients included in the study there were 234 (57.92%) male and 170 (42.08%) female patients. The most common type of stone both in female and male patients was calcium type. From a total of 262 calcium stones, 105 of them (40.07%) was present in female patients and 157 (59.92%) in male. Share of infectious type of stone in female patients was 63 (49.60%) and 64 among males (50.39%). Other stones were less abundant in both the gender groups and their total number was only 17. In women their frequency was 2 (13.33%) and 13 among males (86.67%). There was a significant difference in the frequency of different types of stones by gender (x2 = 11.47, p = 0.009).
Conclusion:
There was no statistically significant correlation between the number of treatments and localization of stones in the ureter, as well as a statistically significant correlation between the size of the stone and the localization of calculus in the ureter.
Keywords: stone in urinary tract, ESWL method of urinary stone treatment
1. INTRODUCTION
One of the most common pathological conditions in human medicine is the presence of a stone in the urinary tract, also characterized as urolithiasis (1-5). In countries with developed industry this disease affects approximately 1500 to 2000 people per million inhabitants (6-10). The stunning fact is that with more than 2/3, and even in 80% of cases this is recurrent disease in the period over the next 20 years (1). The disease is more common in men, comparing with the population of the opposite sex and it is believed that 5% of women and 12% of men during their lifetime can expect at least one renal colic. The disease usually affects people in the fourth and fifth decade of life who are working, and their absence from work to the society has significant social and economic implications. Stone can be localized in different areas of the urinary system. Localization of stone is determined by several factors, including the demographic characteristics. In developed countries, 97% of the stones are localized in the kidney and ureter from which in 59% of cases in the ureter. Urethral stone is in 75% of cases located in the iliac and pelvic part of the ureter (1).
Elimination of stone is determined by size and its localization (11-15). Stone from the ureter in 80% of cases can be eliminated spontaneously. If the stone by its characteristics is not spontaneously eliminated, taken are further steps and therapeutic protocols to solve this problem. Stone larger than 7 mm in diameter, which practically cannot be spontaneously eliminated, threatening kidney development by urostasis and infection (1). Indications for an active therapeutic approach of ureteric stones are: diameter over 7 mm and with low (below 20%) probability of spontaneous elimination or absence of spontaneous stone elimination of any size for a period longer than 30 days from the first renal colic, urinary infection develop, sepsis, calculous anuria, as well as the interest of patients. Treatment of urolithiasis includes conservative, surgical treatment and treatment with extracorporeal shock wave lithotripsy (ESWL) depending on the evaluation by professional medical team. Recently, endoscopic procedures, such as ureterorenoscopy (URS) and percutaneous lithotripsy (PCNL), together with the aforementioned ESWL included, have been almost entirely replaced open surgery in case of stones in urinary tract and thus, in just 30 years, radically changed the approach and functional outcome of this disease (1).
But sometimes the cost of treatment can have an impact on the choice of the primary approach to solving urolithiasis. Grasso et al compared the costs of endoscopic treatment and ESWL for ureteric stones (16). Although the price of sessions ESWL and endoscopic methods were similar, the cost of ESWL, because statistically significantly more frequent additional intervention (31% versus 3%), were incomparably greater.
1.1. Extracorporeal Shock Wave Lithotripsy–ESWL
It is a non-invasive method for the treatment of urinary tract calculus in adults, and its discovery led to a complete change in the therapeutic strategy for urolithiasis. ESWL–Extracorporeal shock wave lithotripsy method is inoperable disintegration and destruction of calculus in urinary and biliary system, applying to the calculus extracorporeal wave produced through the tissues of the body transmitted and focused shock waves (1). The concept of shock waves use for fragmentation of stones started in 1950 in Russia. This happened during the investigation of the supersonic aircraft when Dornie, the German airline, found that shock waves coming from passing debris into the atmosphere could to break something solid, and came to the conclusion that the body that collided with another body, whose movement velocity greater than the speed of sound, resulting shock or vibration waves (1).
The first experimental work in the field of concrement disintegration with extra corporeally produced shock wave lithotripsy (shock waves) is published in Munich in 1972. After in vitro and experiment on an animal model, it is demonstrated that shock waves can disintegrate into tiny pieces concrement susceptible to spontaneous elimination, and that doing so does not create shock waves interference with the formation of lymphocytes, not causing irreversible damage to the parenchymatous organs and muscles, without effect on bone fractures, leading to little change in the canal system of the urinary tract, which would cause difficulty excretion of disintegrated stones and empty gut was led to the development of petechiae. This research as finding showed the existence of cytotoxicity shock waves in cancer cells, which may in future direct the action of these waves to other medical problems.
In February 1980, thanks to the work of doctors from Division of Neurology, University of Munich, ESWL was introduced into clinical practice (5). During 1984 and 1985, many countries in Europe, America and Asia have begun to use appliances for ESWL, and also at our clinic this appliance started to be used in October 1988. The first ten years it was on the camera Dornier MPL 9000 which had only ultrasound guidance and the inability to break up stones in the ureter, and since 1998 used machine Siemens Model Lithostar Multiline, which also possible disintegrating stones in the ureter. This method has dramatically changed the way of treating calculi in the kidney and upper urinary tract and without exaggeration it can be said to be a revolutionary event in the treatment of these diseases. This method is simple, safe and effective (1).
Soon after the introduction, ESWL is being widely accepted in the world, and today 96% of all urinary tract stones are successfully treated by this method. Upon determination of the stone localization, with thousands shock wave lithotripter breaks the same, with an emphasis on regional focus area, which leads to its decomposition into pieces. Using ESWL, which fragment the stones and the “grain” with size of 1-2 mm, it is then spontaneously eliminated in the urine. Relaxing the smooth muscle of the ureter can be achieved before the procedure by α-adrenergic blockers or calcium antagonists. A complication of this procedure is pain like colic pain, and contraindications are cardiac decompensation, stenosis and/or anatomical abnormalities of the urinary tract, as well as coagulation disorders. Lately reports about the possible adverse effects of chronic treatment with this method are: more frequent development of diabetes and hypertension in patients treated with ESWL infection compared with control groups, which still requires additional confirmation through further research (1).
Figure 1.

Treatment of Urinary Stone by ESWL
According to the recommendations of the El-Nahas et al (17), ESWL should be recommended for renal stones localized in the renal pyelon up to 24 mm for the upper or middle stones to 15 mm, and lower stones with size up to 11 mm.
In line with a number of previous studies (1) Tarawneh and colleagues (18) showed an inverse relationship between the density of stones and performance of ESWL, while the CT measured density of stones has a positive correlation with the number of shock waves required for fragmentation.
Bearing in mind that several factors determine as indication as well as success of ESWL treatment, it is important to examine and evaluate all predictive factors that may affect the effectiveness of this treatment.
2. PROBLEM DEFINITION
ESWL treatment is the first-line treatment of urinary tract stones, but there are still no clearly defined limits and recommendations for its use in the treatment of urinary calculi, depending on their location, size and morphological structure. This raises the question of efficiency of ESWL depending on the characteristics of urinary calculi.
3. GOALS
Determine if there is any conditional optimum number of ESWL treatments that lead to disintegration and spontaneous elimination of stones.
Also to establish whether the optimal number ESWL treatment that lead to disintegration of stones and its spontaneous elimination dependent on morphological structure of stones, their size and location in the urinary tract.
4. MATERIAL AND METHODS
The study was prospective, open and comparative. It was conducted at the Urology Clinic Clinical Center of Sarajevo University in the period from 2007 to 2013. The study included 404 patients with urinary tract lithiasis. All patients prior to initiation of therapy–ESWL treatments were subjected to the following diagnostic procedures: anamnesis, clinical examination of patients, laboratory tests, ultrasound examination of the urinary tract and urinary tract X-ray, from which was derived chemical qualitative analysis of morphological stone composition. Diagnostics are used in the detection of complications such as obstruction with dilatation of the renal colorectal system, reduction of the renal parenchyma and in monitoring of renal obstruction during treatment. This type of diagnosis is not suitable for stones in the ureter and can make the difference between calcified and radiolucent concrement.
ESWL treatment is performed on the machine Siemens Model Lithostar Multiline, which has a combined ultrasonographic and fluoroscopic display, large energy density in order to obtain optimum focus (without damaging surrounding tissue) and minimal pain that on rare occasions requires for mild sedation-sedation. Number of maximum shock waves used by one ESWL treatment is 4000, while the energy was dependent on stones localization. Our appliance, like most modern appliances used electromagnetic source. The shock waves are transmits to the body through the water, focused by acoustic lens system so that the released energy is reflected on the surface of the stone.
Results are expressed as mean (X) and standard error of the arithmetic mean (SEM) for the variables that had a normal distribution, as well as the median and interquartile interval (25-75 percentiles) for the variables which had normal distribution. The normality of distribution of variables was tested by the Shapiro-Wilks test. For variables that have followed a normal distribution in a comparative analysis of the independent variables we used Student's t test. For variables that are not following normal distribution in a comparative analysis of independent variables, the Mann-Whitney U test. For nominal and ordinal variables chi-square test was used. In cases when the frequency was lower than expected was used the Fisher's exact test. The degree of correlation was determined by means of the Spearman. P value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS computer software for statistical analysis (SPSS Statistical Package for the Social Sciences) version 13.0.
5. RESULTS
From a total of 404 patients included in the study there were 234 (57.92%) male and 170 (42.08%) female patients.
The most common age group in the sample was at age from 35 to 45 years and consisted of 110 respondents (27.09%). The minimum number of respondents had the age over 65 years 19 respondents (4.67%).
The most common type of stone both in female and male patients was calcium type. From a total of 262 calcium stones, 105 of them (40.07%) was present in female patients and 157 (59.92%) in male. Share of infectious type of stone in female patients was 63 (49.60%) and 64 among males (50.39%). Other stones were less abundant in both the gender groups and their total number was only 17. In women their frequency was 2 (13.33%) and 13 among males (86.67%). There was a significant difference in the frequency of different types of stones by gender (χ2 = 11.47, p = 0.009).
Due to the very low prevalence of other types of stones and inability to perform the chi-square test to a group of other stones are grouped stones which, by virtue were cystine, xanthine stones and uric acid stones. The incidence of cystine calculi was 4 (0.9%), frequency of xanthine stones 3 (0.7%) and uric acid 8 (1.9%). In the group of female respondents 74 (40.88%) had calculus size up to 10 mm, while in the group of male patients stone size up to 10 mm had 107 (59.12%). In the group of female respondents 96 of them (43.05%) had a size of stone exceeding 10 mm, while in the group of male patients stone size over 10 mm had 127 (56.95%). There was no statistically significant difference in the incidence of stones with sizes up to 10 and over 10 mm by gender (χ2 = 0.192, p = 0.661)
5.1. Results of ESWL treatment
The most common frequency of treatments in the sample was 5 treatments (24.01%), followed by 4 treatments (14.6%). From total sample 6 treatments had 13.61% of the respondents, while 7 treatments had 12.87% of the respondents, also 11.88% had 3 treatments and 2 treatments 8.17% of the respondents. In this group 16 treatments had 3.96% of the respondents, and 2.97% had 12 treatments. By 2.72% had a 1 and 9 treatments.
Number of treatment for females was 5 (4-6), while in men and it was 5 (4-7). There was no statistically significant difference in the number of treatment between male and female subjects (p = 0.557).
There was a significant positive correlation between the size stone and number of treatments in the total sample (rho = 0.491, p <0.01), respectively, as the stones were larger was needed and a higher number of treatments.
Number of stones localized at medial renal line who had 0-5 treatment was 66 (79.51%), and 17 (20.49%) had 6 or more than 6 treatments. Number stones localized in the renal pyelon, which received between 0-5 treatments was 35 (52.23%), and 32 of them (47.76%) had 6 or more than 6 treatment. There was no significant difference in the incidence of treatment towards localization (medial/pyelon) (χ2 = 12.543, p <0.001), respectively, medial localization required a smaller number of treatments.
The number of treatments for medially localized stones was 5 (3-5), while for those localized in pyelon was 5 (4-7). There was a statistically significant difference in the number of treatment among these localized calculus (p = 0.0002). Number of ESWL treatment of stones in the renal pyelon is higher than the number of treatments from stones located medially.
Sensitivity to the size of stone was 63.8%, specificity 71.4%, positive predictive value 51.9%, negative predictive of 80.2%. Overall accuracy was 68.9%. AUC for stone size was 0,701. Cut off the size of the calculus was 14.00 mm.
If the stone is larger than 14 mm and if the number of sessions is greater than 5.5, the stone is likely localized in the lower half, and below the numerical values listed in the top half. For all other localization in the kidney, ureter, and the ROC curve was negative–there was no significance.
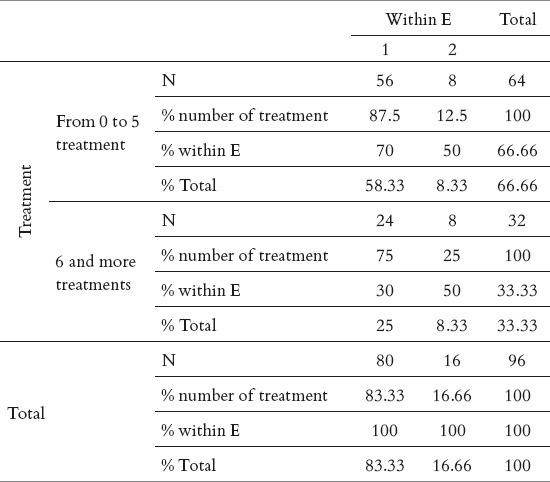
Frequency of localizing at sites of physiological stones stricture site which had a number of treatments 0-5 was 56 (70%), while the frequency of localizing at sites of physiological stones stricture site which had a number of treatment 6 or more was 24 (30%). Frequency of localizing at sites of stones physiological enlargement ureter which had a number of treatments 0-5 was 8 (50%), while the frequency of localizing at sites of stones physiological enlargement of the number of treatments had 6 or more was 8 (50%). There was no statistically significant relationships between a number of treatments and localizing of stone in relation to the physiological narrowing or widening of the ureter (p = 0.150), Table 1.
Table 1.
The relationships between a number of treatments and localization of calculus in the ureter. Ficher exact test; p=0.150
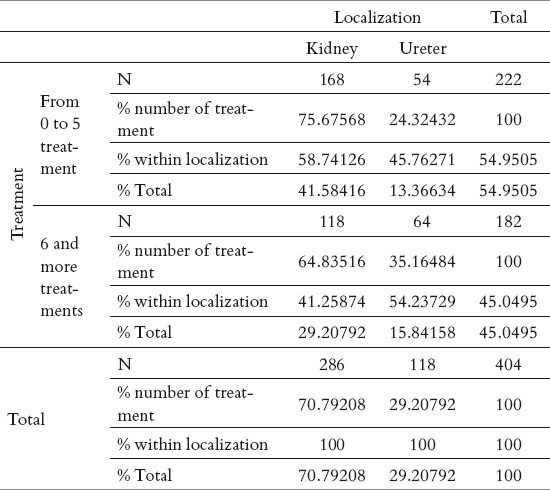
Frequency of localizing stones in the kidney that had a number of treatments 0-5 were 168 (58.74%), while the incidence of kidney stones to the number of treatments have 6 or more was 118 (41.25%). Frequency of stones in the ureter, which had a number of treatments 0-5 was 54 (45.76%), while the frequency of stones in the ureter, which had a number of treatment 6 or more was 64 (54.23%). There was a statistically significant relationships between a number of treatments and kidney stones and/or ureter (χ2 = 5.684, p = 0.017), or larger percentage of a smaller number of treatments in the kidney to the ureter and vice versa (Table 2).
Table 2.
The frequency of the number of treatments in relation to the localization of stones in kidney and ureter. (χ2 = 5.684; df= 1; p=0.017).
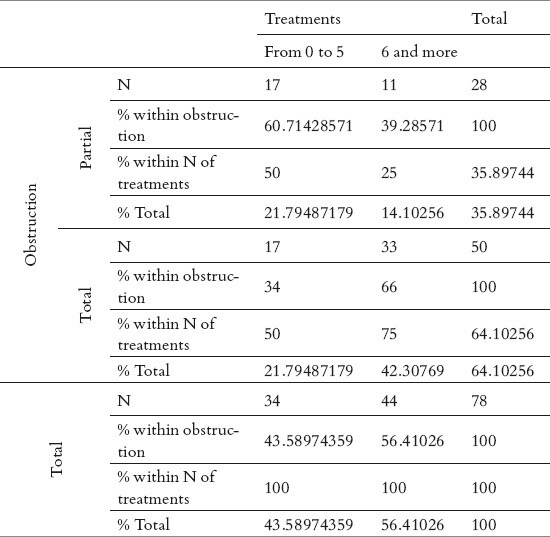
In 17 (50%) patients who had a partial obstruction the number of treatments was 5 or under 5, and 11 (25%) of respondents had 6 or more than 6 treatments. In 17 (50%) patients who had a complete obstruction the number of treatments was 5 or under 5, and 33 (75%) of respondents had 6 or more than 6 treatments. There was a significant correlation between the size of the type of obstruction and the number of treatments (χ2 = 5.209, p = 0.022) (Table 3).
Table 3.
The relationship between the type of obstruction and number of treatments. χ2=5.209; df=1; p=0.022
6. DISCUSSION
Treatment of urolithiasis involves the use of modern machines, such as ESWL. It is shown that ESWL is very easy and useful method of treatment, and as such a first method of choice in the treatment of kidney stones, less invasive than all other methods, with 80-90% treatment success (1). Once we localized place of the calculus, lithotripter breaks the same for thousands of shock waves with an emphasis on regional focal area, which leads to its decomposition into pieces. After treatment, the fragments are removed by urine during the following months (1).
Epidemiological and randomized studies have shown greater security of ESWL treatment methods in breaking stones when it starts with applying lower energy sequences of the same, with a gradual increase energy sequences, resulting in a vasoconstriction which prevents renal damage, and the difference in the fragmentation is not significant despite the fact that whether amplification is carried out or not (19).
Previous clinical and epidemiological studies have shown that as an indication of ESWL treatment urolithiasis depends on several factors, including the size, localization, consistency and other histological characteristics of the stone (20). Pregnancy and specific internship and urological diseases, with an emphasis on acute urinary infection are contraindications for ESWL (1).
Size of stone and its position are prognostic factors that determine the level of disintegration of stone after using ESWL in pediatric patients. According to the analysis of El-Nahas and colleagues (17), ESWL should be recommended for renal pyelon stones up to 24 mm for the upper or middle calix to 15 mm, and lower calix to 11 mm. Although the composition of stone is independent variable that can be useful for predicting the success of ESWL, for most stones is difficult to predict the sensitivity of breaking by the X-ray prior to ESWL. Mentioned facts further complicate decisions in the treatment of this disease, especially when it was still in the account other factors, such as size, localization and other characteristics of the formation. Although ESWL is widely applied therapeutic methods, some studies have shown high rates of recurring stones between 26% and 53% after 10 years (1). According to a number of previous studies, it was found that ESWL method is a risk factor, while in other studies not characterized in this way (2).
Previous studies have shown that the size of stone correlates with the number of ESWL treatments when applied. Besides the size of the stone, even more important feature of the same composition and consistency, because the stones that are chemically softer required significantly fewer applications of ESWL, regardless of its size (1).
Interesting results are presented by Tarawneh and colleagues (18), who proved an inverse correlation between the performance of ESWL and size of the stone. As part of their study, the authors demonstrated that the stones of high density, large size and lower localization in the kidney can better administered in a method PCNL (Percutaneous nephrolytopaxy). Comparing therapeutic procedures for urolithiasis caused by moderately large kidney stones, Resorlu and colleagues (21) showed that PCNL as a therapeutic method has a much higher success rate and a lower rate of recurrence of disease compared with ESWL. However, the authors point out the absence of PCNL, and this is its invasiveness accompanied by blood loss, exposure to radiation, a longer hospital stay.
The results of our study showed a statistically significant positive correlation between the size of stone and number of treatments in the total sample (rho = 0.491, p <0.01), meaning that for the larger size of stone it is necessary to apply a larger number of ESWL treatments. Similar results were from studies by Tarawneh and associates (1), who have proven statistically significant positive correlation between the size stone and number when applied treatment with ESWL. The authors also showed that a higher success rate recorded for stones smaller diameter and percentage of 92% for the lowest diameters, 74% for medium-sized stones, and 50% for larger stones. By Chi square test the authors have shown that the success of the treatment and the size of the stone significantly dependent. When stones over 2 cm in size, the probability of success with ESWL included reducing the need for other methods of treatment increases. The benefit of ESWL's been proven in the treatment of non obstructive kidney stones. In patients with large stones before ESWL-and stenting can provide drainage of urine and prevent obstructive sepsis.
Recent studies and experience have shown that the composition of stone certainly affects the effectiveness of ESWL. Stones made of calcium oxalate dihydrate are easier to crush and infectious stones even easier. Stones made of uric acid are difficult to break, but using more energy they can be broken down into small pieces. Cystine stones are very resistant to breaking. Even if you manage to break, resulting fragments are quite large and difficult to eliminate.
It is shown that not all stones are equally sensitive to treatment. The composition of the stone, which determines its strength, also has an impact on its dissolution, breaking with ESWL and elimination after the treatment. Results of the study showed that the number of treatments is a good indicator of the stone hardness. Sensitivity to the number of treatments was 67.2%, specificity 51.1%, with positive predictive value 73.9%. Cut off the treatments needed to differentiate between hard and soft stones was 4.5. Also, analysis of ROC curve in our results showed that the size of stone is a good indicator of the hardness of stone with a sensitivity of 63.3% and specificity 73.3%. Size stone of 14.5 mm and more proved to be a significant indicator of the hardness of stone regardless of stone location.
By analyzing the effects of ESWL Popov et al (22) showed that low density stones, which are composed by the softer, after one or two sessions with ESWL had effective therapeutic effects in 64.4% of patients. Patients who have had stones greater density, which are at the very composition also firmer, with the same number of sessions were effective therapeutic effects in a small percentage of patients. The same authors have also demonstrated that the stones size over 10 mm require the application of a number of sessions a treatment success.
Phipps et al (23) have shown that the average size of the stones are 7-8 mm in the distal parts ureter after only one treatment over ESWL transgluteal by increasing the success of treatment in relation to the application with the treatment success.
From the analysis of the obtained results, we found that the size stone and number of ESWL sessions are good indicators for differentiation of calculus localization toward the poles. The analysis of the results showed that the stone is localized in the lower half if the stones larger than 14 mm and if the number of treatments is greater than 5.5, and below the specified numerical values on the upper half. For all other localization in the kidney, ureter, and the ROC curve was negative (non-significant).
Frequency of medial localization in stones whose size was less than 10 mm was 39.75%, and the frequency of 60.25% for stones ranging in size over 10 mm. Frequency of pyelon localization in stones smaller than 10 mm was 7.46%, and the frequency of 92.53% for stones ranging in size over 10 mm. There was a significant correlation between the size of the stone and localizing stones (medial / pyelon) (χ2 = 20.443, p <0.001), i.e. Stones up to 10 mm more frequently occurring mediorenal, and more than 10 mm were slightly more common in the pyelon. With a statistically significant correlation between the size of the stone and localizing calculus (medial / pyelon), our results showed a significant difference in the incidence of treatment towards localization (medial / pyelon) (p <0.001) and a significant correlation between the hardness stone and its localizing (p = 0.012) or soft stones occur more frequently in medial localization, and hard stones are somewhat more common in the pyelon.
Previous studies have shown that the localization of kidney stones compared to the lower party, such as the ureter, has a more favorable therapeutic results (1), with the suggestion that prior decisions of ESWL of, besides localization, it is necessary to carefully consider the size and density of the stone, which can greatly affect the outcome of treatment (18). There are also views that the stones were localized in the distal parts of the ureter with ESWL infection removed only when they are placed in the mouth of the urethral. In addition, stones which are located in the ureter, in relation to the renal localization, tend to break up into fragments due to the lack of available space. Common obstructions that accompany localized stones in the ureter hampered conditions for the application of ESWL (1). When it comes to localize the ureter, there was no statistically significant correlation between the size of the stone and localizing the ureter (p = 0.688). Also, our results showed no statistically significant relationships between a number of treatments and localize the calculus in the ureter. According to our results, Pirincci and associates (24) are also observed a significant correlation between the number of treatment and localize the calculus in the ureter.
Comparing the effectiveness of ESWL to localize calculus, Badawy et al (24) showed that the overall success rate for renal and urethral stones in child population was 83.4%. The authors also noted that the re-treatment was necessary in 4% of patients in the group of kidney stones, and in 28% of patients with uretheric stones, with the localization of the urethral calculus had a big impact on treatment outcome. The authors suggest that ESWL treatment in childhood and for renal and urethral stones in a very efficient and cost effective, although children with major dimensions of stone or previously undergoing surgery have a low rate of success.
Factors that determine the effectiveness of ESWL for ureterolites are the following: size, localization, composition, persistence in the ureter, and the degree of dilation of the urinary tract. If the stone is large size, long persisted in the ureter, and the higher hardness, certainly need a larger number of ESWL (1). Perks and colleagues (26) suggest that the density stone below 900 HFU and the distance between the skin and stone of less than 9 cm important factors for predicting treatment success with ESWL methodology. Our findings show that there is a statistically significant correlation between the number of treatment and localize the kidney stones and / or in the ureter. Frequency of localizing stones in the kidney that had a number of treatments 0-5 was 58.74%, while the incidence of kidney stones localizing which had a number of treatments 6 and more was 41.25%. Frequency of localizing stones in the ureter, which had a number of treatments 0-5 was 45.76%, while the incidence of stones located in the ureter, which had a number of treatment 6 or more was 54.23%, i.e. Greater proportion of a small number of treatments kidney and vice versa in the case of localizing stones in the ureter.
7. CONCLUSION
There was a significant positive correlation between the stone size and number of treatments in the total sample. The most common number of treatments in the sample was 5 treatments (24%). ROC curve analysis, as part of the test sensitivity and specificity of stones size in the differentiation of hardness revealed that for stones larger than 14.5 mm, and with the need to apply more than 4.5 ESWL disintegration of stone for the stones that fall the group of hard stones. It was found that the size stone of 14.5 mm and a specificity of 73.3% and a sensitivity of 63.8% in the differentiation of hard stones, until the required number of ESWL of 4.5 or higher has a positive prediction for hardness stone of 73.9%. There was a significant difference in the incidence of treatment localization medial localization and localization in the renal pyelon. Number of ESWL for renal pyelon is higher than in the same with medial localization in the kidney. There was no statistically significant correlation between the number of treatments and localization of stones in the ureter, as well as a statistically significant correlation between the size of the stone and the localization of calculus in the ureter.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Kovačević-Prstojević J. Magistarski rad. Sarajevo: Medicinski fakultet Univerziteta u Sarajevu; 2014. Broj vantjelesnih razbijanja kamenaca u odnosu na veličinu kamenca, njegovu lokalizaciju u urinarnom traktu, te morfološku strukturu kamenca. [Google Scholar]
- 2.Kovacevic-Prstojevic J, Junuzovic Dz, Hasanbegovic M, Lepara Z, Selimovic M, Zunic L. Characteristics of Calculi in the Urinary Tract. Mater Sociomed. 2014 Oct;26(5):297–302. doi: 10.5455/msm.2014.26.297-302. doi: 10.5455/msm.2014.26.297-302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim YJ, Kim CH, Sung EJ, Kim SR, Shin HC, Jung WJ. Association of nephrolithiasis with metabolic syndrome and its components. Metabolism. 2013 Jun;62(6):808–813. doi: 10.1016/j.metabol.2012.12.010. [DOI] [PubMed] [Google Scholar]
- 4.Hesse A, Brande E, Wilbert D, Kohrmann KU, Alken D. Study on the prevalence and incidence of urolithiasis in Germany comparing the years 1977 vs. 2000. Eur Urol. 2003 Dec;44(6):709–713. doi: 10.1016/s0302-2838(03)00415-9. [DOI] [PubMed] [Google Scholar]
- 5.Babenko AI, Murakhovsky AG, Tomtchuk AL, Bravve YI. About the formation of patients’ flow in multi-type hospital. Probl Sotsialnoi Gig Zdravookhranenniiai Istor Med. 2012 Nov-Dec;6:35–38. [PubMed] [Google Scholar]
- 6.Marković V, Urologija I. Beograd: ovinsko izdavačka ustanova Službeni list SRJ; 1997. Hirurgija mokraćnih organa. [Google Scholar]
- 7.Li LP, Fan YZ, Zhang Q, Zhang SL. Clinical analysis of 41 children's urinary calculus and acute renal failure. Zhonghua Er Ke Za Zhi. 2013 Apr;51(4):295–297. [PubMed] [Google Scholar]
- 8.Lulich JP, Osborne CA. Urolithiasis: past, present and future. J Small Anim Pract. 2012 Nov;53(11):621–622. doi: 10.1111/j.1748-5827.2012.01300.x. [DOI] [PubMed] [Google Scholar]
- 9.Teichman JMH. Acute Renall Colic from Ureteal Calculus. N Engl J Med. 2004;350(7):684–693. doi: 10.1056/NEJMcp030813. [DOI] [PubMed] [Google Scholar]
- 10.Galić J, Perković J. Pristup liječenju urolitijaze. MEDIX. 2010;16(91):180–184. [Google Scholar]
- 11.Marshall LS, Tanagho EA, McAninch JW. Urinary Stone Disease. In: Tanagho EA, editor. Smith's General Urology. 16th edition. San Francisko: Lange Medical Book; 2004. [Google Scholar]
- 12.Mennon M, Resnick M, Retik AB, et al. Urinary Lithiasis: Ethiology, Diagnosis and Medical Management. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ, et al., editors. Cambell's Urology. 8ht ed. Philadelphia, PA: Saunders Elsevir; 2002. pp. 3287–3289. [Google Scholar]
- 13.Bartuś K, Sadowski J, Kapelak B, Zajdel W, Godlewski J, Bartuś S, et al. Denervation (ablation) of nerve terminalis in renal arteries: early results of interventional treatment of arterial hypertension in Poland. Kardiol Pol. 2013;71(2):152–158. doi: 10.5603/KP.2013.0008. [DOI] [PubMed] [Google Scholar]
- 14.Kotur-Stevuljevic J, Simic-Ogrizovic S, Dopsaj V, Stefanovic A, Vujovic A, Ivanic-Corlomanovic T, et al. A hazardous link between malnutrition, inflammation and oxidative stress in renal patients. Clin Biohem. 2012 Oct;45(15):1202–1205. doi: 10.1016/j.clinbiochem.2012.04.021. [DOI] [PubMed] [Google Scholar]
- 15.Ležaić V, Ristić S, Dopsaj V, Marinković J. Is morning urinary protein-to-creatinine ratio a reliable estimator of 24-hour proteinuria in patient with kidney disease? Srp Arh Celok Lek. 2010 Nov-Dec;138(11-12):726–731. doi: 10.2298/sarh1012726l. [DOI] [PubMed] [Google Scholar]
- 16.Grasso M, Beaghler M, Loisides P. The case for primary endoscopic management of upper urinary tract calculi: II. Cost and outcome assessment of 112 primary ureteral calculi. Urology. 1995 Mar;45(3):372–376. doi: 10.1016/S0090-4295(99)80003-X. [DOI] [PubMed] [Google Scholar]
- 17.El-Nahas AR, El-Assmy AM, Awad BA, Elhalwagy SM, Elshal AM, Sheir KZ. Extracorporeal shockwave lithotripsy for renal stones in pediatric patients: A multivariate analysis model for estimating the stone-free probability. Int J Urol. 2013 Feb; doi: 10.1111/iju.12132. doi: 10.1111/iju.12132. [DOI] [PubMed] [Google Scholar]
- 18.Tarawneh E, Awad Z, Hani A, Haroun AA, Hadidy A, Mahafza W, et al. Factors affecting urinary calculi treatment by extracorporeal shock wave lithotripsy. Saudi J Kidney Dis Transpl. 2010 Jul;21(4):660–665. [PubMed] [Google Scholar]
- 19.European Association of Urology. Guidelines 2012 edition. [Accessed: January 2014]. Available on: http://www.uroweb.org/fileadmin/guidelines/2012_Guidelines_large_text_print_total_file.pdf .
- 20.Pu YR, Manousakas I, Liang SM, Chang CC. Design of the dual stone locating system on an extracorporeal shock wave lithotriptor. Sensors (Basel) 2013 Jan;13(1):1319–1328. doi: 10.3390/s130101319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Resorlu B, Unsal A, Ziypak T, Diri A, Atis G, Guven S, et al. Comparison of retrograde intrarenal surgery, shockwave lithotripsy, and percutaneous nephrolithotomy for treatment of medium-sized radiolucent renal stones. World J Urol. 2012 Nov 22; doi: 10.1007/s00345-012-0991-1. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 22.Popov E, Donkov I, Slavov C, Georgiev M. Correlation of CT stone density and skin-to-surface distance with ESWL efficacy on lower pole kidney stones. AFJU. 2012;18(Suppl):53–54. [Google Scholar]
- 23.Phipps S, Stephenson C, Tolley D. Extracorporeal shockwave lithotripsy to distal ureteric stones: the transgluteal approach significantly increases stone-free rates. BJU Int. 2013 Jul;112(2):E129–33. doi: 10.1111/j.1464-410X.2012.11738.x. [DOI] [PubMed] [Google Scholar]
- 24.Pirincci N, Gecit I, Bilici S, Taken K, Tanik S, Ceylan K. The effectiveness of extracorporeal shock wave lithotripsy in the treatment of ureteral stones in children. Eur Rev Med Pharmacol Sci. 2012 Oct;16(10):1404–1408. [PubMed] [Google Scholar]
- 25.Badawy AA, Saleem MD, Abolyosr A, Aldahshoury M, Elbadry MS, Abdalla MA, et al. Extracorporeal shock wave lithotripsy as first line treatment for urinary tract stones in children: outcome of 500 cases. Int Urol Nephrol. 2012 Jun;44(3):661–666. doi: 10.1007/s11255-012-0133-0. [DOI] [PubMed] [Google Scholar]
- 26.Perks AE, Schuler TD, Lee J, Ghiculete D, Chung DG, D’A Honey RJ, et al. Stone attenuation and skin-to-stone distance on computed tomography predicts for stone fragmentation by shock wave lithotripsy. Urology. 2008 Oct;72(4):765–769. doi: 10.1016/j.urology.2008.05.046. [DOI] [PubMed] [Google Scholar]