

Abstract
A 36-year-old, otherwise-healthy woman with a 6-year history of progressive dysphagia underwent an esophagogram that revealed an oblique extrinsic defect with an inferior-to-superior (left-to-right) course consistent with an aberrant right subclavian artery. An aortogram confirmed the diagnosis of aberrant right subclavian artery.
She underwent surgical repair, tolerated the procedure well, and was discharged home, symptom free, on postoperative day 3. We found that the right supraclavicular approach provides good exposure and avoids the morbidity of the classically described approach via a median sternotomy or thoracotomy.
Key words: Aorta, thoracic/abnormalities; aortic arch syndromes/surgery; constriction, pathologic; deglutition disorders/etiology; esophageal stenosis/etiology; subclavian artery/abnormalities
Surgical correction is indicated for dysphagia lusoria in association with an aberrant right subclavian artery. We describe our use of the right supraclavicular approach, which avoids the possible complications of thoracotomy or sternotomy.
Case Report
A 36-year-old, otherwise-healthy woman with a 6-year history of progressive dysphagia was referred to Waterbury Hospital. Her dysphagia had progressed to the point that she could eat only small meals.
An esophagogram (Fig. 1) revealed a notching of the upper esophagus from an extrinsic compression, which was consistent with an aberrant right subclavian artery.

Fig. 1 Esophagogram: An oblique extrinsic defect courses from inferior (left) to superior (right) (arrow), consistent with an aberrant right subclavian artery at the upper thoracic level just above the aortic arch.
Subsequently, an arteriogram confirmed the aberrant origin of the right subclavian artery (Fig. 2), arising from the aorta distal to the usual left subclavian artery. The artery had a retro-esophageal course that was causing compression of the esophagus. Her blood pressure was equal in both upper extremities. Due to the persistence and worsening of her symptoms, surgical correction was recommended. Approximately a month later, the patient was taken to the operating room for resection and reconstructive bypass surgery.

Fig. 2 Arteriogram: The aberrant right subclavian artery arises from the aorta distal to the origin of the left subclavian artery (arrow).
Surgical Technique
Under general anesthesia, the patient was placed in the supine position, with a sandbag in the midline behind her shoulders, to extend her neck. Through a right supraclavicular incision, we divided the clavicular head of the sternomastoid muscle and identified and exposed the right common carotid artery. We then located the aberrant right subclavian artery and followed its retro-esophageal segment to its origin at the aortic arch, by retracting the esophagus anteriorly. Injury to the brachial plexus and the right recurrent laryngeal nerve was avoided by careful identification of these structures.
After systemic heparinization and application of a vascular clamp, we were able to divide, ligate, and oversew the proximal portion of this artery almost at its origin. The distal portion of the right subclavian artery was trimmed, with careful preservation of the right vertebral artery; then an end-to-side anastomosis was made with the right common carotid artery (Fig. 3). At the end of the operative procedure, there was no vocal cord paralysis, and good pulses were palpated in the right radial artery.
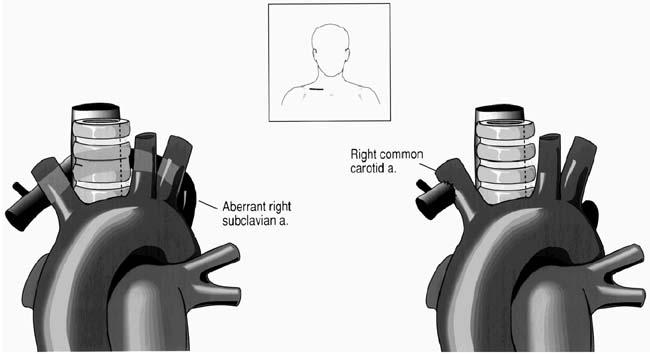
Fig. 3 Through a right supraclavicular incision (inset), the aberrant right subclavian artery was dissected and divided after application of vascular clamps. The proximal end was ligated and oversewn at the anomalous origin. The distal end was anastomosed to the right common carotid artery.
Postoperatively, the patient tolerated a regular diet without symptoms of dysphagia. The right upper extremity had a 2+ palpable radial pulse, with blood pressure equal to that of the contralateral side. She was discharged home on postoperative day 3. Four years later, she remained without symptoms of dysphagia.
Discussion
The most common embryologic abnormality of the aortic arch is an aberrant right subclavian artery, which occurs in 0.5% to 1.8% of the population.1,2
As hypothesized by Edwards, this abnormal origin of the right subclavian artery can be explained by the involution of the 4th vascular arch with the right dorsal aorta.3 The 7th intersegmental artery remains attached to the descending aorta, and this persistent intersegmental artery becomes the right subclavian artery. This leads to the aberrant artery, which often follows a retro-esophageal course (Fig. 4).
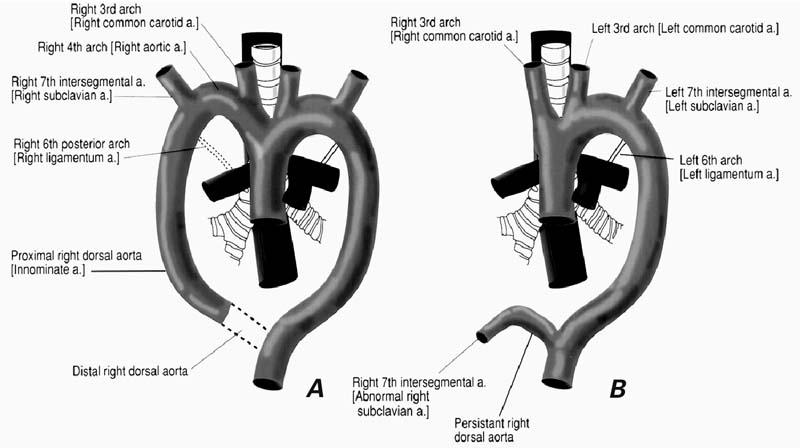
Fig. 4 A) The normal embryologic development of the aortic arches: Dotted lines represent normal vessel involution of the right dorsal aorta and the right 6th posterior arch. The persistence of the proximal right dorsal aorta becomes the innominate artery. B) Abnormal embryologic development of the aortic arch: The involution of the right 4th vascular arch and proximal right dorsal aorta leaves the right 7th intersegmental artery attached to the abnormally persistent right dorsal aorta. After rotation of the dorsal aorta, the right 7th intersegmental artery becomes the aberrant right subclavian artery.
Although most cases of this anomaly are asymptomatic, symptoms may appear when a “ring” completely encircles the trachea or the esophagus. Extrinsic compression of the esophagus may lead to dysphagia. This phenomenon, first reported in 1794 by London physician David Bayford, was originally described as “dysphagia by freak of nature,” and is commonly referred to as dysphagia lusoria.4
In 1936, Kommerell described the radiologic findings of this persistent route of the aortic arch as an aortic diverticulum (Kommerell's diverticulum).5 The 1st successful repair of this anomaly was reported by Robert Gross in 1946.6 Early reports revealed that simple division without restoration of flow leads to weakness and ischemia of the right arm, which can cause a reversal of blood flow from the right vertebral artery to the right subclavian artery. This phenomenon, first described by Contorni in 1960,7 was named subclavian steal by Reivich and colleagues in 1961.8 In 1964, Hallman and Cooley recommended an arteriogram prior to surgical repair of the congenital aortic vascular ring in adults.9
Reconstitution of flow to a divided aberrant right subclavian artery was first performed by Bailey and associates in 1965.10 They attached the distal end of the ligated artery to the ascending aorta proximal to the right common carotid artery. Numerous alternatives have been described. Cooley was the first to attach the distal subclavian artery to the right common carotid artery.11 In this case, the right supraclavicular approach was found to provide excellent exposure for proximal ligation and distal anastomosis of the aberrant right subclavian artery to the right common carotid artery.
This technique, elegantly described by Valentine and colleagues in 1987,12 is a simplified version of the low cervical approach originally described by Orvald and co-authors in 1972,13 which required extensive dissection on both sides of the esophagus before ligation of the aberrant subclavian artery.
In our opinion, the supraclavicular approach provides good exposure, rapid recovery, and avoids the morbidity associated with the classically described median sternotomy or thoracotomy.
Footnotes
Address for reprints: Massoud A. Marjani, MD, Department of Surgery, Waterbury Health Center, Waterbury, CT 06708
E-mail: massoudmarjani@earthlink.net
Dr. Carrizo is now at North Shore–Long Island Jewish Health System, Manhasset, New York.
References
- 1.Richardson JV, Doty DB, Rossi NP, Ehrenhaft JL. Operation for aortic arch anomalies. Ann Thorac Surg 1981;31: 426–32. [DOI] [PubMed]
- 2.Stewart JR, Kincaid OW, Edwards JE. An atlas of vascular rings and related malformations of the aortic arch system. Springfield (IL): Charles C. Thomas; 1964. p. 53.
- 3.Edwards JE. Congenital malformations of the heart and great vessels. Section H. Malformations of the thoracic aorta. In: Gould SE, editor. Pathology of the heart. 2nd ed. Springfield (IL): Charles C. Thomas 1960. p. 391–462.
- 4.Bayford D. An account of a singular case of obstructed deglutition. Memoirs Med Soc London 1794;2:275–86.
- 5.Kommerell B. Verlagerung des osophagus durch eine abnorm verlaufende arteria subclavia dextra (arteria lusoria). Fortschr Geb Rontgenstr Nuklearmed 1936;54:590–5.
- 6.Gross RE. Surgical treatment for dysphagia lusoria. Ann Surg 1946;124:532–4. [PubMed]
- 7.Contorni L. The vertebro-vertebral collateral circulation in obliteration of the subclavian artery at its origin [in Italian]. Minerva Chir 1960;15:268–71. [PubMed]
- 8.Reivich M, Holling HE, Roberts B. Reversal of blood flow through the vertebral artery and its effect on cerebral circulation. N Engl J Med 1961;265:878–85. [DOI] [PubMed]
- 9.Hallman GL, Cooley DA. Congenital aortic vascular ring. Surgical considerations. Arch Surg 1964;88:666–75. [DOI] [PubMed]
- 10.Bailey CP, Hirose T, Alba J. Re-establishment of the continuity of the anomalous right subclavian artery after operation for dysphagia lusoria. Angiology 1965;16:509–13. [DOI] [PubMed]
- 11.Cooley DA. Surgical treatment of aortic aneurysms. Philadelphia: WB Saunders; 1986. p. 175–84.
- 12.Valentine RJ, Carter DJ, Clagget GP. A modified extrathoracic approach to the treatment of dysphagia lusoria. J Vasc Surg 1987;5:498–500. [PubMed]
- 13.Orvald TO, Scheerer R, Jude JR. A single cervical approach to aberrant right subclavian artery. Surgery 1972;71:227–30. [PubMed]
For Further Reading
- 1.Brown DL, Chapman WC, Edwards WH, Coltharp WH, Stoney WS. Dysphagia lusoria: aberrant right subclavian artery with a Kommerell's diverticulum. Am Surg 1993;59: 582–6. [PubMed]
- 2.Janssen M, Baggen MG, Veen HF, Smout AJ, Bekkers JA, Jonkman JG, Ouwendijk RJ. Dysphagia lusoria: clinical aspects, manometric findings, diagnosis, and therapy. Am J Gastroenterol 2000;95:1411–6. [DOI] [PubMed]
- 3.Taylor M, Harris KA, Casson AG, DeRose G, Jamieson WG. Dysphagia lusoria: extrathoracic surgical management. Can J Surg 1996;39:48–52. [PMC free article] [PubMed]
- 4.Karlson KJ, Heiss FW, Ellis FH Jr. Adult dysphagia lusoria. Treatment by arterial division and reestablishment of vascular continuity. Chest 1985;87:684–6. [DOI] [PubMed]
- 5.Bogliolo G, Ferrara M, Masoni L, Pietrapaolo V, Pizzicannella G, Miscusi G. Dysphagia lusoria: proposal of a new treatment. Surg Endosc 1987;1;225–7. [DOI] [PubMed]
- 6.Chaffin JS, Munnell ER, Grantham RN. Dyphagia lusoria: current surgical approach. J Cardiovasc Surg (Torino) 1978; 19:311–3. [PubMed]
- 7.Freed K, Low VH. The aberrant subclavian artery. Am J Radiol 1997;168:481–4. [DOI] [PubMed]
- 8.Kent PD, Poterucha TH. Images in clinical medicine. Aberrant right subclavian artery and dysphagia lusoria. N Engl J Med 2002;346:1637. [DOI] [PubMed]