

Abstract
Lipomas are the most common type of soft tissue mesenchymal tumors. They are typically located subcutaneously and consist of mature fatty tissue. When they occur under the enclosing fascia, they are called deep-seated lipomas. Infrequently, lipomas can arise inside the muscle and are called intramuscular lipomas. Intramuscular lipomas have been commonly investigated and categorized in the same group as other deep-seated and superficial lipomatous lesions. Their clinical, histological and imaging characteristics may resemble well-differentiated liposarcomas, further adding to the difficulties in the differential diagnosis. This article summarizes the available literature and describes the typical epidemiological, pathological and clinical features of intramuscular lipomas, as well as delineating their treatment and prognosis.
Key words: lipoma, intramuscular, deep-seated
Introduction
Lipomas are benign mesenchymal tumors. They are the most common type of soft tissue tumors.1 Usually, they are localized superficially to the enclosing fascia in the subcutaneous tissues (subcutaneous lipoma). However, lipomas may be localized deep under the enclosing fascia; these are called deep-seated lipomas. Intramuscular lipomas are deep-seated lipomas which originate within the muscle. Although there are numerous papers discussing intramuscular lipomas, and some authors have tried to differentiate them from other lipomatous lesions for over a century, there is still great deal of confusion regarding their characteristic features and the use of terms when referring to them. Intramuscular lipomas have been commonly investigated and categorized in the same group as other deepseated and superficial lipomatous lesions.2,3
In 1853, Paget described a lipoma infiltrated into the trapezius muscle and in 1946, Regan et al. introduced the term infiltrating lipoma.4-7 Later, Greenberg et al. recognized that infiltrating lipomas may be either intermuscular or intramuscular using the classification of Moriconi, which differentiated between lipomas based on whether they were located between or within the muscles.8,9 Subsequently, it was also recognized that intramuscular lipomas can present as infiltrative, well-defined/non-infiltrative and mixed (with areas of infiltration and well-defined areas) variant.10,11
The authors of this article use the terms intramuscular lipoma and intermuscular lipoma, reserving the term infiltrating lipoma when there is clear radiological, surgical or microscopic evidence of infiltration of muscle or other adjacent structure. Of note is that many of the intermuscular and a small number of the intramuscular lipomas will grow by expansion and enclosure of other structures rather than infiltration. It is sometimes difficult to define the exact location of origin, especially when encountering a large lipoma arising from a small muscle with a large extramuscular component or intermuscular lipoma which secondary infiltrated the adjacent muscle. Because many clinicians are still unaware of the significance of a lipoma arising within the muscle, knowledge of this pathology can help the physician to provide appropriate care and counseling for the patient and prevent anxiety and fear from malignancy. This article reviews the characteristic epidemiological, pathological, clinical, and imaging features of intramuscular lipomas, as well as outlining their treatment and outcome after treatment.
Epidemiology
The precise epidemiological and demographic characteristics of intramuscular lipomas are not very well defined. The fact that intramuscular lipomas are relatively uncommon and have been commonly investigated and categorized in the same group as other deep-seated and superficial lipomas, contributed to the difficulties in better defining the typical epidemiological and demographic characteristics of these tumors.2,3 Another contributing factor is that many of the old studies investigating lipomatous tumors lack cytogenetic testing which may have misdiagnosed low-grade liposarcomas for intramuscular lipomas based on histology alone, further adding to the inaccuracy of the data in these studies.
Prevalence
Intramuscular lipoma is a relatively uncommon condition and accounts for just over 1.8% of all primary tumors of adipose tissue and less than 1% of all lipomas.10,12 Furthermore, Fletcher et al. found that 83% were of the infiltrative type and 17% were the well-defined type.10 Lipomas are estimated to be multiple in 5-15% of patients.1 However, most intramuscular lipomas are located within a single muscle (solitary) with only a few cases reported involving two or more muscles.8,13,14 Co-existence of intramuscular lipoma with other lipomatous and non-lipomatous tumors such as spindle cell lipoma, parosteal lipoma, well-differentiated liposarcoma and laryngeal squamous cell carcinoma in the same patient have been reported on occasion.14-18
Age distribution
Intramuscular lipomas may occur in all age groups, from childhood to old age. However, the majority of them occur between the ages of 40 and 70 years.6,10 The average age at presentation has been reported as 58.7 years,19 54 years,20 50 years,21 49 years,22 and 48 years.23 Furthermore, Fletcher et al. found that the average age for infiltrative subtype was 51.5 years and for the well-circumscribed subtype was 47.25 years.10
Gender distribution
Clear gender predilection has not been currently established. However, there is female predominance in the majority of studies where intramuscular lipomas were separately evaluated.5,10,19-25 In contrast, other large studies have shown that men were affected more often than women.3,26 For example, Ramos-Pacua et al. found that among 50 patients with intramuscular and intermuscular lipomas, 62% were men and 38% women.3 However, these studies did not calculate separately the gender distribution among different lipoma subtypes, which most likely distorted the accuracy of that demographic characteristic.
Anatomical distribution
Although it is generally believed that intramuscular lipomas primarily occur in the large muscles of the limbs and the trunk,6,27 they can occur in almost any anatomical site.28-43 The exact topographical distribution has not been calculated and has varied among different studies. Nishida et al. found that the most common location was the thigh followed by the shoulder.19 Basset et al. found that 47 % of intramuscular lipomas arose in the upper limb or chest wall.20 In addition, Fletcher et al. found that of the infiltrative subtype 38% were located in the trunk, 20% in the head and neck, 18% in the upper limb and 10% in the lower limb. In contrast, from the well-circumscribed type, 87.5 % were located in the trunk and 12.5% in the head.10 In the head and neck regions, involvement of different muscles such as the neck muscles, tongue, cheek, orbicularis muscle and temporalis muscle have been described with the tongue being one of the most commonly involved sites.6,44-69 Intramuscular lipomas of the hand and foot are rare.70-73
Etiology and pathogenesis
The exact etiology and pathogenesis of intramuscular lipomas remains unclear. Similar to other lipoma subtypes, intramuscular lipomas most likely have neoplastic pathogenesis and represent a true neoplasm directly originating from multipotent mesenchymal cells. Reactive pathogenesis have been proposed as well. Trauma, chronic irritation, obesity, developmental disorders, endocrine, dysmetabolic and genetic factors provoking the uncontrolled growth of lipomas have all been suggested to play a possible role in the development of intramuscular lipomas.3,25,47,74 Ramos-Pascua et al. suggested that body mass index may be related to the development of intramuscular lipomas as two-thirds of their cases were overweight or obese.3 Bjerreagaard et al. suspected hormonal imbalance; however, all tests for estrogen receptors in their study were negative.25 To the best of our knowledge, no familial cases of intramuscular lipomas have been reported. Further studies using molecular techniques are needed to understand the exact mechanism of the underlying benign growth or neoplastic transformation.
Similarly, the mechanisms of infiltrative growth of intramuscular lipomas are not fully understood. Aberrant high mobility group proteins have been reported to play a role during the development of lipomatous tumors.75 Furthermore, Mori et al. reported type-selective muscle fiber atrophy or degenerative changes in 70% of intramuscular lipomas examined by immunohistochemical analysis, most of which were the infiltrative type. In addition, the patterns of fiber atrophy were not confined to the areas of fatty infiltration but were also detected in the peripheral muscle fibers where tumor involvement was not prominent. In half of these tumors, they found type II (fast fiber) dominant pattern atrophy and in the other half type I (slow fiber) dominant pattern atrophy. These findings strongly suggest association with focally neurogenic or myogenic disorders in the lesion. The authors also suggested that these changes may modulate the infiltrating growth characteristic of intramuscular lipoma.75
Gross pathoanatomy and histopathology
Intramuscular lipomas present with typical gross pathological and histopathological features which can establish the diagnosis in the majority of cases. In histologically questionable cases, cytogenetic testing may be very useful in establishing the correct diagnosis and differentiate them from other lipomatous lesions.
Gross pathological features
On gross examination, the majority of intramuscular lipomas are seemingly circumscribed, masses of uniform, yellowish adipose tissue with mottled tan areas and a soft consistency. Often the mass has lobulated surface. Some of them are attached to obvious skeletal muscle. Their shape is typically round or fusiform. They can vary in size from 1 cm to 25 cm.10,20Usually they are non-capsulated although small number of masses may be capsulated. Nishida et al. found that a capsule separating the lesion from the surrounding muscles was recorded in only 12.5 % of the cases.19 The intramuscular lipoma with extramuscular component may have a capsule at the extramuscular margin (the outer margin) and not on the margin in the muscle. On cross section, the cut surface can vary from yellow to dark tan. Some tumors may have a grayish, firm surface. In the infiltrative type, bundles of muscle fibers can be noticed passing through the tumor.19 Interestingly, Fletcher et al. did not notice obvious muscular tissue macroscopically within the fat in any of their tumors.10 Entrapped muscle fibers are typically not observed in the well-encapsulated intramuscular lipomas. Occasionally, focal calcification can be observed.10,76 Usually, no macroscopic evidence of necrosis or hemorrhage is noted.10
Histological and cytological features (microscopic pathological features)
Histologically, intramuscular lipomas can be divided into the infiltrative type, well- circumscribed type, and mixed type (with areas of infiltrative margins and well-circumscribed or encapsulated areas). The histological features of infiltrative intramuscular lipomas are distinctive. They have relatively uniform appearance characterized by mature uni-vaculoated adipocytes of fairly uniform size and shape which irregularly infiltrate between muscle fibers and, in many places, completely replacing the muscle bundles. Rarely, intramuscular lipomas may infiltrate not only the muscle but also the fascia and tendon.26 When cut in cross section there is a checkerboard-like appearance and, in longitudinal section, a striped appearance (Figure 1). Adipocytes’ nuclei are small, flattened and peripherally situated. They do not display nuclear atypia and there is no increased mitosis, hyperchromasia, pleomorphysim or multinucleation of fat cells. Lipoblasts are not identified. Individual muscle fibers are normal or often atrophic, but do not show the striking reactive changes, such as increased nuclear/cytoplasmic ratio and multinucleation, often seen at the advancing edge of desmoid fibromatoses or many sarcomas. Muscle fibers may be widely separated.13 A delicate connective tissue stroma may be focally present. The tumor vasculature is very scanty and consistent of occasional thin-walled capillaries. Larger vessels, which are always solitary, are exceedingly rare. In some tumors, histology may reveal areas of fat necrosis, hemorrhage and cyst formation.10,25 The areas of fat necrosis are associated with lipid-laden macrophages and chronic inflammatory cell infiltrate, composed entirely of lymphocytes. These foci are often associated with adjacent fibrosis, but irregular fibrous septa or significant paramuscular fibrosis is never seen in the absence of degenerative, inflammatory features.10 The well-circumscribed intramuscular lipomas are composed solely of a discrete mass of uniform, mature adipocytes, which are clearly delineated from the surrounding muscle. No fatty infiltration of adjacent muscle fibers and entrapped muscle is typically evident within the tumor itself. In these cases, fibrous stroma condenses toward the borders of the tumor forming a capsule.26 Similar to the infiltrative type, there is no adipocytic atypia and lipoblasts are never seen. Blood vessels are scarce and uniformly small. Chondroid or osseous metaplasia is occasionally encountered within intramuscular lipomas, particularly if they are long-standing.27,77 Ossification presents as haphazardly distributed and interlacing thin lamellar bone structures which can be disseminated throughout the tumor or concentrated at the periphery of the mass.13,76,77 Thin trabeculae of mature bone can be also found in the fibrous septae as well.77 Frequently, there are peripheral osteoblasts surrounding the mature bone.
Figure 1.
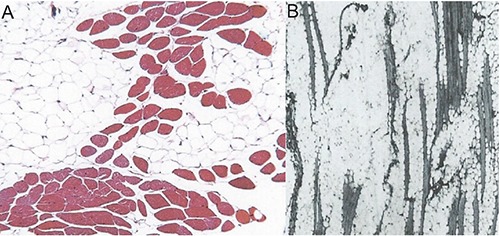
A) Histological appearance of the infiltrative intramuscular lipoma. Mass of mature uni-vacuolated adipocytes of fairly uniform size, which irregularly infiltrate between muscle fibers. Transverse section showing chequerboard-like appearance. Reproduced with permission (D’Alfonso™, 2011; Copyright 2011 College of American Pathologists).37 B) Histological appearance of the infiltrative intramuscular lipoma. Mass of mature uni-vacuolated adipocytes of fairly uniform size, which irregularly infiltrate between muscle fibers. Longitudinal section showing the striated appearance of the muscle fibers caused by the proliferation of fat cells. Reproduced with permission (Kindblom LG, 1974; Copyright 1974 American Cancer Society).27
Normally, there is no nuclear atypia or increased rate of mitosis.77 A single case of isolated (localized) idiopathic granulomatous vasculitis characterized by transmural inflammatory cell infiltrate composed of epitheloid histiocytes, multinucleated giant cells and lymphocytes isolated to the intramuscular lipoma has been reported as well.78
Histological and cytological differential diagnosis of intramuscular lipoma is mainly versus well-differentiated liposarcoma. Well-differentiated liposarcomas are distinguished from intramuscular lipomas by the presence of atypical cells or vacuolated lipoblasts admixed with fibroblasts-like spindle cells, frequently located in the septa. Compared to intramuscular lipomas, well-differentiated liposarcomas have more and thicker fibrous septae with some large and small blood vessels.24,79 Inflammatory cell and myxoid areas are frequently observed near the septa.80 The other lesion with which intramuscular lipomas may be confused histologically is intramuscular hemangioma. Intramuscular hemangiomas often show a prominent adipose tissue component replacing adjacent muscle. However, the extensive vascular component will render the diagnosis simple.10 Primary muscular diseases that may result in fatty degeneration and fatty replacement of the muscle are excluded by the clinical presentation and dystrophic changes characterized by fiber size variability, fiber necrosis, regeneration, inflammation and connective tissues deposition. A single case of spindle-cell lipoma inside an intramuscular lipoma has been reported, presenting as a single heterogeneous mass. In this case, a second well-circumscribed tumor consistent of mixture of mature fat cells and uniform, small spindle cells with scant, elongated cytoplasm was described.15 Careful examination of the entire mass with sufficient numbers of histological samples will provide the correct pathological diagnosis and prevent mislabeling other fat containing lesions, which may require a different treatment approach.
Cytogenetic profile
The advancement and development of better cytogenetic methods in the last few decades resulted in the cytogenetic characterization of a number of soft tissue tumors including lipomatous tumors. Cytogenetic abnormalities have been found to be common in lipomatous tumors and to correlate reliably with morphological subtypes.81 Specific chromosomal abnormalities have been described in intramuscular lipomas. Fletcher et al. reviewed the karyotype of 178 lipomatous tumors.81 Six cases were classified as intramuscular lipomas of ordinary type. All cases arose in the extremities. Karyotypically, two cases each have shown aberrations affecting 8q and 12q; one of the latter was combined with 13q abnormality. The remaining two lesions showed aberrations affecting other chromosomes. None had normal karyotype. They also concluded that there are no consistent cytogenetic differences between subcutaneous, subfascial and intramuscular lipomas of ordinary type. Sreekantaiah et al. reported that in their series of lipomas, all patients with intramuscular lipomas had abnormal karyotypes.82 Furthermore, they reported that the depth of the lipoma was significantly related to the finding of complex abnormality as four of the 9 patients with complex changes in their series of 109 lipomas had intramuscularly-situated lipomas.82 In a study of 106 lesions (55 classified as intramuscular lipomas and 51 classified as atypical lipomatous tumors) Bassett et al. found that the cytogenetic studies of intramuscular lipomas revealed simple translocations or loss of chromosomal material involving the q14-15 region on chromosome 12, paracentric or pericentric inversions of chromosome 12q14-15, aberrations involving 6p21-22, or loss of material from the q12-14 or q22 region of chromosome 13.20 The rearrangements involving 12q14-15 and 6p21-22 lead to overexpression of HMGIC and HMGIY, respectively. The proteins encoded by these genes are high mobility group proteins that are involved in determining chromosomal structure and are known to affect gene expression globally.20
Pierron et al. studied a single case of a 5-year-old boy with intramuscular lipoma of the buttock and found a translocation involving the short arm of chromosome 9 and the long arm of chromosome 12 [karyotype 46, XY,t(9;12)(p22;q14)].83 Furthermore, they found rearrangement of both HMGA2 and NFIB genes with HMGA2-NFIB fusion. Bao et al. reported a case of a three-way translocation t(1;4;12)(q25;q27;q15) as the sole chromosomal abnormality in an 8-year-old girl with an intramuscular lipoma.84
Although further knowledge is needed to better understand the spectrum of cytogenetic characteristics of lipomatous tumors generally and intramuscular lipomas in particular, it is clear that cytogenetic analysis can be of diagnostic value in hystologically borderline or difficult cases. Because it appears that based on histology alone, it is possible to misdiagnose intramuscular lipoma with well-differentiated liposarcoma, cytogenetic testing may be very useful in these cases. In contrast to intramuscular lipomas, well-differentiated liposarcomas are typically associated with supernumerary ring or giant marker chromosomes.81,85,86 While histological diagnosis is the gold standard for diagnosis in lipomatous tumors, cytogenetic analysis is quickly becoming an integral part of the diagnostic work up. Additionally, cytogenetic analysis may potentially be useful in predicting the disease course. In general, tumors with complicated chromosome aberrations are associated with a poor disease course.84
Clinical presentation
Clinically, intramuscular lipomas most often present as a slowly growing asymptomatic mass or swelling with no palpable mass. Pain is a late and uncommon symptom, usually in deep and very large lipomas and is most likely due to compression or expansion of the adjacent soft tissues or compression of the adjacent peripheral nerve.13,33,34,39,43 Paresthesias and nerve distribution neurological deficit due to nerve impingement can be encountered as well.22,26,46 A small number of patients may complain of occasional cramping. Dysfunction of the engaged muscle due to extensive infiltration has been reported.26,46 When the mass increases in size, decreased range of motion or functional limitation due to mechanical restriction may be an associated complaint. Duration of symptoms before diagnosis may vary from a few months to years.
Physical examination shows a palpable mass or soft tissue swelling of fairly soft consistency. However, consistency can vary with the density of the fibrous tissue stroma. In some cases the tumor changes its consistency and form when the engaged muscle is contracted. In this case, the tumor may become more readily palpable, firmer and more spherical. However, in some cases the tumor can be firm even with the muscle relaxed.33 The tumor is usually not tender to palpation, but may be tender in some cases. The mass is freely movable and not fixed to the bone or overlying skin. Some intramuscular lipomas may exhibit diminished mobility due to their infiltration to the muscle. The skin and vessels overlying the mass show no changes even in the presence of a fairly large mass.28 However, superficial venous congestion caused by peripheral vascular compression has been reported in a large deltoid intramuscular lipoma.33 Nonetheless, this is not typical and is usually a sign of malignancy. No associated lymphadenopathy is usually detected.
Other specific symptoms and clinical presentation depend on the location and the volume of the tumor. They can mimic other more common pathologies in that specific region and can be misdiagnosed initially. When encountered in the supraspinatus muscle, intramuscular lipoma may cause impingement syndrome.35,36 When encountered in the pectoralis muscle, it may mimic breast cancer.29,37,38 When encountered in the chest wall, it may imitate a pulmonary nodule.12 When encountered in the muscles of the retropharyngeal space, the patient may present with dysphagia and dysphonia due to compression of the recurrent laryngeal nerve or mass effect.47,55,60 When reported in the tongue, it can cause difficulties with deglutition, mastication and speech.46,62-64 Proptosis and diplopia have been reported with intramuscular lipoma of the superior oblique muscle.6 Headache has been reported with intramuscular lipoma of the temporalis muscle.51 Clinically, intramuscular lipomas are difficult to differentiate from other benign (neoplastic and non-neoplastic) and malignant masses occurring in the soft tissues. Differential diagnosis should include hematoma, muscle herniation, ganglion cyst, heterotopic ossification, angiolipoma, haemangioma, fibrous myositis, primary muscular disease with fatty infiltration, liposarcoma, fibrosarcoma and other soft tissue masses. Large intramuscular lipomas also need to be differentiated from lipomatosis, a process of diffuse overgrowth of mature adipocytes, which presents with extensive infiltration of muscle and subcutaneous tissue. Patient with lipomatosis are affected at a much younger age and typically the entire body region is involved.
Imaging characteristics
Imaging is important to establish a diagnosis, define the size, location and relationship with adjacent anatomical structures as well as to determine an operative plan. Different studies have tried to identify the imaging characteristics of lipomas and differentiate them from other fat containing tumors.80,87-90 However, very few of them have tried to investigate the spectrum of imaging characteristics of intramuscular lipomas independently from other lipoma subtypes.19,23
Roentgenographic imaging characteristics
The plain radiographs may either be unremarkable or may demonstrate a radiolucent soft-tissue mass of fat opacity. Most cases are sharply outlined and in some cases the enclosing fascia can be identified as a thin layer of higher density.26 Relatively opaque streaks caused by muscle bundles can be seen within the tumor area.26 In some cases, the bundles may dominate to such an extent that the true nature of the lesion may be misjudged. Soft tissue calcifications can occasionally be noticed.12,76,77 On angiography, increased vascularity, abnormal vessel formation and early venous filling are not usually apparent.5,34 In cases of masses located in the breast area where mammography is performed, radiolucent mass of fat density can be noticed in the pectoralis muscle.29
Ultrasonographic imaging characteristics
Ultrasongraphy has played a major role in the study of lipomatous tumors.91 In contrast, the ultrasound features of intramuscular lipomas have been noted in occasional case reports or grouped together with superficial lipomas (Figure 2A).29,37,71,92,93 Similar to superficial lipomas, they have presented with a spectrum of ultrasound characteristics. There are no large studies evaluating the ultrasound characteristics of intramuscular lipomas independently. However, Paunipager et al. investigated the ultrasound features of 64 deep-seated lipomas: the majority of them (56%) were intramuscular.93 In their study, they found that shape varied and was roundish, ovoid, oblonged and geographical. The majority of lipomas had well-defined margins but a small percentage had ill-defined margins. On ultrasound, the overall echogenicity was hyperechoic compared to muscle in the majority of cases, but it was also hypoechoic and isoechoic in a small fraction of the sample. Acoustic transmission compared to adjacent muscle was increased in the majority of cases but was found to be equal and decreased in some cases. Most of the lipomas presented with fine internal echoes oriented parallel to the long axis of the tumor. The majority of lipomas had no internal vascularity on ultrasound although some of them expressed mild and minimal vascularity. Tumors with entrapped muscle fibers may appear heterogeneous and will have internal striations on ultrasound imaging. Zamora et al. reported a case of infiltrative intramuscular lipoma with irregular margins and interdigitations within skeletal muscle that created a typical striated appearance (Figure 2B).92
Figure 2.
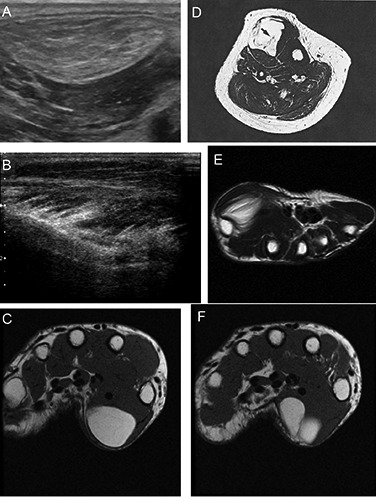
A) Ultrasound imaging of intramuscular lipoma showing hyperechoic (compared to adjacent muscle), relatively well-defined mass with fine internal echoes. Reproduced under the Creative Commons Attribution License from Chernev I, 2013.71 B) Ultrasound imaging showing heterogeneous thenar intramuscular lipoma with irregular margins and interdigitations within skeletal muscle that create the typical striated appearance. Reproduced with permission of the American Institute of Ultrasound in Medicine (Zamora MA, 2005; Permission conveyed through Copyright Clearance Center, Inc).92 C) MRI of intramuscular lipoma of the thenar eminence. Note the fat signal intensity and homogeneous appearance of the mass. Reproduced under the Creative Commons Attribution License from Chernev I, 2013.71 D) MRI intramuscular lipoma of the tibialis anterior muscle. Note the heterogeneous appearance of the mass with streaky intralesional structures. Reproduced with permission (Nishida J, 2007; pending permission from Springer Science and Business Media).17 E) MRI showing a mass with increased signal intensity infiltrating the thenar muscles. The lesion appears isointense relative to subcutaneous fat and is compatible with a deep infiltrating intramuscular lipoma. Reproduced with permission of the American Institute of Ultrasound in Medicine (Zamora MA, 2005; Permission conveyed through Copyright Clearance Center, Inc).92 F) MRI of intramuscular lipoma of the thenar eminence. Note the bilobular appearance of the tumor. Reproduced under the Creative Commons Attribution License from Chernev I, 2013.71
Although ultrasonography is a good initial diagnostic modality and may suggest the fatty nature of the mass, computed tomography (CT) scan and magnetic resonance imaging (MRI) are significantly superior for the confident identification of adipose tissues in lipomas. Furthermore, complete anatomical relationship of the lipoma with the adjacent structures is more difficult to assess with ultrasonography compared to CT scan and MRI.
Computed tomography imaging characteristics
CT scan is very suitable for the diagnosis of lipoma. The CT scan appearance of intramuscular lipomas reveals a hypodense mass situated within the muscle with Hounsfield values in the negative range.29 Attenuation is similar to that of fat tissue. The shape of the mass may vary but is usually ovoid or fusiform. The mass may be well-circumscribed or have poorly defined margins.46 Thick and thin soft tissue density streaks are commonly found inside the lesion. The thickness of the streaks varies and they are interrupted occasionally.19 These streaky structures are more distinctive on CT scan than on MRI.19 If ossification is present, CT scan can better delineate it. Some lesions may present as an area of radiolucency surrounded by a radiodense zone, consistent with ossification, separate from the adjacent bone.77 In these cases, differential diagnosis includes myositis ossificans or other calcified tumors. In contrast to intramuscular lipomas, the shape of well-differentiated liposarcomas is more often oblong or dumbbell-shaped. The CT scan typically reveals a fat density mass with areas of hazy amorhous density, usually accompanied by both thick and thin streaky soft tissue densities.19 The streaky lesions are occasionally interrupted.
Magnetic resonance imaging characteristics
MRI is very useful in distinguishing fat-containing tumors from other soft tissue tumors. MRI is also an excellent imaging modality to distinguish among lipomatous masses. On MRI, intramuscular lipomas may present with a spectrum of imaging characteristics. The shape of the mass may vary from round, ovoid and fusiform to irregularly polygonal.19,23 Very occasional dumbbell-shaped masses can be present.19 The fatty tissue in the intramuscular lipomas demonstrates high signal intensity on both T1- and T2- weighted images. Fat-suppressed sequences demonstrate signal suppression similar to normal fat. Intramuscular lipomas can be homogeneous with intensity similar to subcutaneous fat or heterogeneous with intermingled muscle fibers and other types of tumor tissue (Figure 2C,D). The intermingled muscle fibers are isointense to normal muscle on both T1- and T2-weighted images. Interdigitations with skeletal muscle showing the characteristic striated appearance is pathognomonic for intramuscular lipoma and has not been described with other lipomatous tumors (Figure 2E).1 The MRI findings of intermingled fat and muscle fibers do not correspond completely to the infiltrative type determined by histological findings.23 Some tumors may only show microscopic infiltration at the edges which is difficult to pick up on imaging. Tumor margins can be well-defined when the lesion is sharply demarcated and infiltrative (irregular) when the neoplastic fatty tissue infiltrates the surrounding muscle tissue. Capsule may be occasionally encountered and it may be found only on the outside part of the intramuscular lipoma and not on the side of the muscle. In addition, capsule may not be distinguished from the surrounding muscle even if present.1 Encapsulated intramuscular lipomas do not usually have muscle fibers incorporated in the main mass. The majority of intramuscular lipomas present as a single nodule (uninodular) although occasionally binodular masses are encountered (Figure 2F).23,71 Both thick and thin linear structures can be observed in intramuscular lipomas. They can be present within the nodes or between the nodules.
Although other masses may present with lipomatous components, they are easily recognized on MRI studies. Similar to histological differential diagnosis, the main differential diagnosis, when imaging, is versus well-differentiated liposarcoma, which sometimes can be difficult to differentiate from intramuscular lipoma. On MRI, liposarcomas tend to be larger than intramuscular lipomas, however size alone is not a good predictive factor for malignancy.87 In contrast to intramuscular lipomas, liposarcomas are usually multilobular and have more and thicker septae with nodules. They may also contain globular areas of other tumor tissue different from muscle and that can be easily distinguished on MRI.23,94 Some authors have suggested surgical biopsy or fine-needle aspiration cytology of heterogeneous deep lipomatous masses directed at nonadipose nodular or globular components to diagnose well-differentiated liposarcoma.24,95 Controversy exists regarding entrapped muscle fibers in lipomatous tumors as a sign of malignancy or benignancy. Hosono et al. reported that the septum-like structures contained entrapped muscle fibers pathologically.96 Donoto et al. also reported intermingled muscle fibers in two cases of liposarcoma.97 However, both of their cases were recurrences. In contrast, Matsumoto et al. did not find any muscle tissue in the septum-like structures in his cases.94 Regardless of this controversy, the typical infiltrative striated MRI appearance of some intramuscular lipomas is so characteristic and combined with other MRI characteristic may be pathognomonic in the majority of cases. Occasionally, intramuscular lipomas have to be differentiated from lipomatosis, which also has infiltrative characteristics. On MRI, lipomatosis shows the characteristics of lipomatous lesion which is poorly circumscribed and affects both the subcutis and deep soft tissues.98
Nuclear medicine imaging characteristics
Although malignant tumors typically demonstrate intense uptake, whereas benign lesions show less uptake, nuclear medicine imaging has not been used extensively in the diagnosis of intramuscular lipomas. Otsuka et al. studied 91 patients with soft tissue tumors with Thallium-201 chloride scintigraphy; among them 16 lipomas (14 pathologically proven and 2 not proven) with none of them showing high uptake in any phase.99 Unfortunately, they did not report how many of these were intramuscular vs. other lipoma subtypes. Ramos Pascua et al. reported on a single deltoid intramuscular lipoma, where the Tc 99 scan was normal.33 At this time, the role of nuclear medicine imaging for the diagnosis of intramuscular lipomas is limited and not very well established.
Treatment, recurrence and prognosis
Treatment of intramuscular lipomas depends on the tumor location, size and clinical symptoms referable to the lesion. Conservative treatment has a limited role in the treatment of symptomatic intramuscular lipomas. If the lipoma is small and does not cause functional limitations, simple observation and reassurance of the benign nature are sufficient. Although there are some reports of successful treatment of lipomas with intralesional injection of products such as steroid in animal studies, the role of that type of treatment in humans is not very clearly defined.100 Surgical excision is the treatment of choice when the patient is symptomatic and also for cosmetic purposes. Marginal excision of the well-circumscribed area and wide excision with free margin in the infiltrative areas, whenever possible, will help preventing recurrences.21 Debulking is also an acceptable option if in an unsuitable area for complete excision or if complete resection will lead to a significant functional impairment. Chemotherapy and radiotherapy are not generally recommended for the treatment of intramuscular lipoma due to the benign character of this tumor.
Currently, the disease recurrence rate of intramuscular lipoma is believed to be very low.3,20,21 However, the recurrence rate after treatment has been historically reported in the literature between 3 and 62.5% depending on the investigators.13,20,62,65 Recurrence can occur and is thought to be due to incomplete removal of lipoma during surgery. This is most likely due to the proximity of the tumor to important anatomical structures or fear of disabling functional limitations with complete resection of the involved muscle. Su et al. treated surgically 8 patients with intramuscular lipomas at different locations and no local recurrence was noticed in an average follow up period of 40 months. They performed marginal excision around the well-encapsulated border area and wide excision in the infiltrating areas. The infiltrating areas were identified by preoperative MRI. Subsequently, frozen sections examinations were performed intraoperatively.21 Ramos-Pascua et al. did not have any recurrences in their patients, although two of the patients who presented initially to their center for recurrences had small tumor remnants detected on MRI at six months postoperatively.3 Bjerregaard et al. treated 12 patients surgically by wide resection. During follow up averaging seven years, the tumor recurred in five patients.25 Basset et al. investigated 55 patients with intramuscular lipoma and only two (4%) had disease recurrence.20
Studies that reported a high rate of local disease recurrence were performed at a time when lipoblasts were required for the diagnosis of well-differentiated liposarcoma. Therefore, these studies likely misclassified many patients with well-differentiated liposarcoma as having intramuscular lipoma.20 It is possible that the true disease recurrence rate of intramuscular lipomas is much lower than previously reported; however this needs further investigation. Recurrence can occur many years after excision.10,21 Fletcher found a range from 14 months to 19 years.10 The median time between primary excision and first recurrence was 6 years.10 Studies which reported short term recurrence rates, most likely did not represent the true recurrence rate of intramuscular lipomas. Of note is that none of the well-circumscribed tumors recurred locally in the study by Fletcher.10 Furthermore, the median size of the infiltrative lesions which recurred locally was not significantly different from the rest of the group.
Despite their infiltrative nature and their tendency to recur locally, intramuscular lipomas are benign lesions, which do not have malignant potential and do not metastasize. However, malignant transformation of intramuscular lipoma has been suggested even though no definite evidence is available. Matsumoto et al. reported a case of a liposarcoma coexisting with multiple intramuscular lipomas, and suggested that the former may have resulted by malignant transformation from one of these benign lesions.14 Nevertheless, Murphy et al. believe that malignant transformation of lipomas is nonexistent and the rare reported cases likely represented sampling errors or misdiagnosis at initial investigation.1 Primary spreading to adjacent muscle is unusual and it is not clear if these cases represent intramuscular lipomas or diffuse intramuscular lipomatosis sparing the subcutaneous tissues.8,13
Conclusions
Intramuscular lipomas are relatively uncommon lipoma subtype. Due to the unfamiliarity with that pathology, they have been commonly misclassified and misdiagnosed with other benign and malignant lesions. Careful clinical, histological, imaging and cytogenetic examination can reveal the typical characteristics of intramuscular lipomas and be pathognomonic in the majority of cases. This can further allow appropriate treatment and prognosis.
References
- 1.Murphey MD, Carroll JF, Flemming DJ, et al. From the archives of the AFIP: benign musculoskeletal lipomatous lesions. Radiographics 2004;24:1433-66. [DOI] [PubMed] [Google Scholar]
- 2.Billing V, Mertens F, Domanski HA, Rydholm A. Deep-seated ordinary and atypical lipomas: histopathology, cytogenetics, clinical features, and outcome in 215 tumours of the extremity and trunk wall. J Bone Joint Surg Br 2008;90:929-33. [DOI] [PubMed] [Google Scholar]
- 3.Ramos-Pascua LR, Guerra-Álvarez OA, Sánchez-Herráez S, et al. Intramuscular lipomas: Large and deep benign lumps not to be underestimated. Review of a series of 51 cases. Rev Esp Cir Ortop Traumatol 2013;57:391-7. [DOI] [PubMed] [Google Scholar]
- 4.Regan JM, Bickel WH, Broders AC. Infiltrating benign lipomas of the extremities. West J Surg 1946;54:87-93. [PubMed] [Google Scholar]
- 5.Austin RM, Mack GR, Townsend CM, Lack EE. Infiltrating (intramuscular) lipomas and angiolipomas: a clinicopathologic study of six cases. Arch Surg 1980;115:281-4. [DOI] [PubMed] [Google Scholar]
- 6.Dutton J, Wright J. Intramuscular lipoma of the superior oblique muscle. Orbit 2006;25:227-33. [DOI] [PubMed] [Google Scholar]
- 7.Dionne GP, Seemayer TA. Infiltrating lipomas and angiolipomas revisited. Cancer 1974;33:732-8. [DOI] [PubMed] [Google Scholar]
- 8.Greenberg SD, Isensee C, Gonzalez-Angulo A, Wallace SA. Infiltrating lipomas of the thigh. Am J Clin Pathol 1963;39:66-72. [DOI] [PubMed] [Google Scholar]
- 9.Wurlitzer F, Bedrossian C, Ayaia A, et al. Problems of diagnosing and treating infiltrating lipomas. Am Surg 1973;39:240-3. [PubMed] [Google Scholar]
- 10.Fletcher CD, Martin-Bates E. Intramuscular and intermuscular lipoma: neglected diagnoses. Histopathology 1988;12:275-87. [DOI] [PubMed] [Google Scholar]
- 11.Chernev I. Intramuscular lipoma: infiltrating vs. well-circumscribed variant. Pan Afr Med J 2014;17:170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee JH, Do HD, Lee JC. Well-circumscribed type of intramuscular lipoma in the chest wall. J Cardiothorac Surg 2013;8:181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Morris AD, Jane MJ, Ritchie D, Helliwell T. Diffuse intramuscular lipomatosis of a lower limb. Sarcoma 1998;2:53-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Matsumoto K, Hukuda S, Ishizawa M, et al. Liposarcoma associated with multiple intramuscular lipomas. A case report. Clin Orthop Relat Res 2000;373:202-7. [DOI] [PubMed] [Google Scholar]
- 15.Usta U, Türkmen E, Mizrak B, et al. Spindle cell lipoma in an intramuscular lipoma. Pathol Int 2004;54:734-9. [DOI] [PubMed] [Google Scholar]
- 16.Goldman AB, DiCarlo EF, Marcove RC. Case report 774. Coincidental parosteal lipoma with osseous excrescence and intramuscular lipoma. Skeletal Radiol 1993;22:138-45. [DOI] [PubMed] [Google Scholar]
- 17.Laliotis A, Bree E, Vasilaki S, et al. Co-existence of intramuscular spindle cell lipoma with an intramuscular ordinary lipoma: report of a case. Pol J Pathol 2013;64:224-7. [DOI] [PubMed] [Google Scholar]
- 18.Momin TA, Deyrup AT, Grist WJ, et al. Laryngeal squamous cell carcinoma metastatic to a flank intramuscular lipoma. Am Surg 2008;74:447-8. [PubMed] [Google Scholar]
- 19.Nishida J, Morita T, Ogose A, et al. Imaging characteristics of deep-seated lipomatous tumors: intramuscular lipoma, intermuscular lipoma, and lipoma-like liposarcoma. J Orthop Sci 2007;12:533-41. [DOI] [PubMed] [Google Scholar]
- 20.Bassett MD, Schuetze SM, Disteche C, et al. Deep-seated, well differentiated lipomatous tumors of the chest wall and extremities. The role of cytogenetics in classification and prognostication. Cancer 2005;103:409-16. [DOI] [PubMed] [Google Scholar]
- 21.Su CH, Hung JK, Chang IL. Surgical treatment of intramuscular, infiltrating lipoma. Int Surg 2011;96:56-9. [DOI] [PubMed] [Google Scholar]
- 22.Lee Y, Jung J, Baek G, Chung M. Intramuscular Lipoma in the Thenar or Hypothenar Muscles. Hand Surgery 2004;9:49-54. [DOI] [PubMed] [Google Scholar]
- 23.Matsumoto K, Hukuda S, Ishizawa M, Chano T, Okabe H. MRI findings in intramuscular lipomas. Skeletal Radiol 1999;28:145-52. [DOI] [PubMed] [Google Scholar]
- 24.Elbardouni A, Kharmaz M, Salah Berrada MS, et al. Well-circumscribed deep-seated lipomas of the upper extremity. A reports of 13 cases. Othop Traumatol Surg Res 2011;97:152-8. [DOI] [PubMed] [Google Scholar]
- 25.Bjerreagaard P, Hagen K, Daugaard S, Kofoed H. Intramuscular lipoma of the lower limb. Long-term follow-up after local resection. J Bone Joint Surg Br 1989;71:812-5. [DOI] [PubMed] [Google Scholar]
- 26.Kindblom LG, Angervall L, Stener B, et al. Intermuscular and intramuscular lipomas and hibernomas: a clinical, roentgenologic, histologic, and prognostic study of 46 cases. Cancer 1974;33:754-62. [DOI] [PubMed] [Google Scholar]
- 27.Kransdorf MJ, Moser RP, Jr, Meis JM, Meyer CA. Fat-containing soft-tissue masses of the extremities. Radiographics 1991;11:81-106. [DOI] [PubMed] [Google Scholar]
- 28.Lahrach K, Kadi K, Mezzani A, et al. An unusual case of an intramuscular lipoma of the biceps brachii. Pan African Med J 2013;15:40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pant R, Poh ACC, Hwang SG. An unusual case of an intramuscular breast mass. Ann Acad Med Singapore 2005;34:275-6. [PubMed] [Google Scholar]
- 30.Balabram D, Cabral CCdSR, Filho OdPR, Barros CPd. Intramuscular lipoma of the subscapularis muscle. Sao Paulo Med J 2014;132:65-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Oyama N, Oyama N, Hiroshi K, et al. Left ventricular asynchrony caused by an intramuscular lipoma: computed tomographic and magnetic resonance detection. Circulation 2003;107:e200-1. [DOI] [PubMed] [Google Scholar]
- 32.Takamori S., Miwa K., Hayashi A, Shirouzu K. Intramuscular lipoma in the chest wall. Eur J Cardiothorac Surg 2004;26:1038. [DOI] [PubMed] [Google Scholar]
- 33.Ramos Pascua L, Alonso León A, Santos Sánchez JA, Ferrández Portal L. Intramuscular lipoma of the deltoid mimicking a sarcoma. A case report. Chir Organi Mov 2001;86:153-7. [PubMed] [Google Scholar]
- 34.Warner JJ, Madsen N, Gerber C. Intramuscular lipoma of the deltoid causing shoulder pain: report of two cases. Clin Orthop 1990;253:110-2. [PubMed] [Google Scholar]
- 35.Egea Martinez JM, Mena JF. Lipoma of the supraspinatus muscle causing impingement syndrome a case report. J Shoulder Elbow Surg 2009;18:3-5. [DOI] [PubMed] [Google Scholar]
- 36.Ferrari L, Haynes P, Mack J, DiFelice GS. Intramuscular lipoma of the supraspinatus causing impingement syndrome. Orthopedics 2009;32:601. [DOI] [PubMed] [Google Scholar]
- 37.D’Alfonso TM, Shin SJ. Intramuscular lipoma arising within the pectoralis major muscle presenting as a radiographically detected breast mass. Arch Pathol Lab Med 2011;135:1061-3. [DOI] [PubMed] [Google Scholar]
- 38.Gopal U, Patel MH, Wadhwa MK. Intramuscular lipoma of the pectoralis major muscle. J Postgraduate Med 2002;48:330. [PubMed] [Google Scholar]
- 39.Gutknecht DR. Painful intramuscular lipoma of the thigh. South Med J 2004;97:1121-2. [DOI] [PubMed] [Google Scholar]
- 40.Harrington AC, Adnot J, Chesser RS. Infiltrating lipomas of the upper extremities. J Dermatol Surg Oncol 1990;16:834-7. [DOI] [PubMed] [Google Scholar]
- 41.Ezirmik N, Yildiz K. Deep intramuscular lipoma in thigh. Med J Bakirkoy 2011;7:167-9. [Google Scholar]
- 42.Allen B, Rader C, Babigian A. Giant lipomas of the upper extremity. Can J Plast Surg 2007;15:141-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kapetanakis S, Papathanasiou J, Dermon A, et al. Unusual intramuscular lipoma of the deltoid muscle. Folia Medica 2010;52:68-71. [DOI] [PubMed] [Google Scholar]
- 44.Collela G, Lanza A, Rossiello L, Rossiello R. Infiltrating lipoma of the tongue. Oral Oncology Extra 2004;40:33-5. [Google Scholar]
- 45.Garavaglia J, Gnepp D. Intramuscular (infiltrating) lipoma of the tongue. Oral Surg Oral Med Oral Pathol 1987;63:348-50. [DOI] [PubMed] [Google Scholar]
- 46.Colella G, Biondi P, Caltabiano R, et al. Giant intramuscular lipoma of the tongue: a case report and literature review. Cases J 2009;2:7906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Pichierri A, Marotta N, Raco A, Delfini R. Intramuscular infiltrating lipoma of the longus colli muscle: a very rare cause of neck structures compression. Cent Eur Neurosurg 2010;71:157-9. [DOI] [PubMed] [Google Scholar]
- 48.Charles NC, Palu RN. Intramuscular lipoma of the eyelid. Ophthalmic Surg Lasers 2000;31:340-1. [PubMed] [Google Scholar]
- 49.Akbulut M, Aksoy A, Bir F. Intramuscular lipoma of the tongue: a case report and review of the literature. Aegean Pathol 2005;2:146-9. [Google Scholar]
- 50.Keskin G, Ustundag E, Ercin C. Multiple infiltrating lipomas of the tongue. J Laryngol Otol 2002;116:395-7. [DOI] [PubMed] [Google Scholar]
- 51.Ban M, Kitajima Y. Intramuscular lipoma within the temporal muscle. Int J Dermatol 2002;41:689-90. [DOI] [PubMed] [Google Scholar]
- 52.Salvatore C, Antonio B, Vecchio W, et al. Giant infiltrating lipoma of the face: CT and MR imaging findings. Am J Neuroradiol 2003;24:283-6. [PMC free article] [PubMed] [Google Scholar]
- 53.Ozcan C, Gorur K, Talas D, Aydin O. Intramuscular benign lipoma of the sternocleidomastoid muscle: a rare cause of neck mass. Eur Arch Otorhinolaryngol 2005;262:148-50. [DOI] [PubMed] [Google Scholar]
- 54.Dattilo DJ, Ige JT, Nwana EJ. Intraoral lipoma of the tongue and submandibular space: report of a case. J Oral Maxillofac Surg 1996;54:915-7. [DOI] [PubMed] [Google Scholar]
- 55.Eisele D, Landis G. Retropharyngeal infiltrating lipoma-a case report. Head Neck 1988;10:416-21. [DOI] [PubMed] [Google Scholar]
- 56.Shiraki K, Kamo M, Sai T, Kamo R. Rare site for an intramuscular lipoma. Lancet 2002;359:2077. [DOI] [PubMed] [Google Scholar]
- 57.Mattel SF, Persky MS. Infiltrating lipoma of the sternocleidomastoid muscle. Laryngoscope 1983;93:205-7. [DOI] [PubMed] [Google Scholar]
- 58.Lerosey Y, Choussy O, Gruyer X, et al. Infiltrating lipoma of the head and neck: a report of one pediatric case. Int J Pediatr Otorhinolaryngol 1999;47:91-5. [DOI] [PubMed] [Google Scholar]
- 59.Del Castillo-Pardo de Vera JL, Cebrian Carretero JL, Gomez-Garcia E. Chronic lingual ulceration caused by lipoma of the oral cavity. Med Oral 2004;9:163-7. [PubMed] [Google Scholar]
- 60.Senchenkov A, Werning J, Staren E. Radiographic assessment of the infiltrating retropharyngeal lipoma. Otolaryngol Head Neck Surg 2001;125:658-60. [DOI] [PubMed] [Google Scholar]
- 61.Bennhoff DF, Wood JW. Infiltrating lipomata of the head and neck. Laryngoscope 1978;88:839-48. [DOI] [PubMed] [Google Scholar]
- 62.Garg M, Aggarwal R, Rajeev S. Intramuscular lipoma of tongue. J Cutan Aesthet Surg 2011;4:152-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Bandeca MC, De Padua JM, Nadalin MR, et al. Oral soft tissue lipomas: a case series. J Canad Dental Assoc 2007;73:431-4. [PubMed] [Google Scholar]
- 64.Amirzedeh A, Klaustermeyer W. Intramuscular lipoma of the tongue masquerading as angioedema. Ear, Nose Throat J 2013;92:1-3. [DOI] [PubMed] [Google Scholar]
- 65.Sohn W, Kim JH, Jung SN, et al. Intramuscular lipoma of the sternocleidomastoid muscle. J Craniofacial Surg 2010;21:1976-8. [DOI] [PubMed] [Google Scholar]
- 66.Dattolo RA, Nesbit GM, Kelly KE, Cupp CL. Infiltrating intramuscular lipoma of the paraspinal muscles. Ann Otol Rhinol Laryngol 1995;104:582-4. [DOI] [PubMed] [Google Scholar]
- 67.Chung JC, Ng RW. A huge tongue lipoma. Otolaryngol Head Neck Surg 2007;137:830-1. [DOI] [PubMed] [Google Scholar]
- 68.Piattelli A, Fioroni M, Iezzi G, Rubini C. Osteolipoma of the tongue. Oral Oncol 2001;37:468-70. [DOI] [PubMed] [Google Scholar]
- 69.Piattelli A, Fioroni M, Rubini C. Intramuscular lipoma of the cheek: a case report. J Oral Maxillofac Surg 2000;58:817-9. [DOI] [PubMed] [Google Scholar]
- 70.Mohan L, Semoes J. Thenar intramuscular lipoma: an unusual case. Internet J Surg 2008;17:22. [Google Scholar]
- 71.Chernev I, Tingey S. Thenar intramuscular lipoma: A case report. J Med Cases 2013;4:676-8. [Google Scholar]
- 72.Aldredge WM, Halpert B. Lipoma of the thenar. Surgery 1948;24:853. [PubMed] [Google Scholar]
- 73.Lui TH. Intramuscular lipoma of abductor digiti minimi mimicking intramuscular haemangioma. BMJ Case Rep 2013;2013:bcr2013200897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Copcu E. Can intramuscular lipoma have a post-traumatic origin? Br J Dermatol 2003;149:1084-5. [DOI] [PubMed] [Google Scholar]
- 75.Mori K, Chano T, Matsumoto K, et al. Type-selective muscular degeneration promotes infiltrative growth of intramuscular lipoma. BMC Musculoskelet Disord. 2004;5:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Demiralp B, Alderete JF, Kose O, et al. Osteolipoma independent of bone tissue: a case report. Cases J 2009;2:8711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Heffernan EJ, Lefaivre K, Munk PL, Nielsen TO, Masri BA. Ossifying lipoma of the thigh. Br J Radiol 2008;81:207-10. [DOI] [PubMed] [Google Scholar]
- 78.Fernando Val-Bernal J, Val D, Calvo I, Francisca Garijo M. Isolated (localized) idiopathic granulomatous (giant cell) vasculitis in an intramuscular lipoma. Pathol Res Pract 2006;202:171-6. [DOI] [PubMed] [Google Scholar]
- 79.Evans HL, Soule EH, Winkelmann RK. Atypical lipoma, atypical intramuscular lipoma, and well differentiated retroperitoneal liposarcoma: a reappraisal of 30 cases formerly classified as well differentiated liposarcoma. Cancer 1979;43:574-84. [DOI] [PubMed] [Google Scholar]
- 80.Ohguri T, Aoki T, Hisaoka M, et al. Differential diagnosis of benign peripheral lipoma from well-differentiated liposarcoma on MR imaging: is comparison of margins and internal characteristics useful? Am J Roentgenol 2003;180:1689-94. [DOI] [PubMed] [Google Scholar]
- 81.Fletcher CDM, Akerman M, Dal Cin P, et al. Correlation between clinicopathological features and karyotype in lipomatous tumors. A report of 178 cases from the Chromosomes and Morphology (CHAML) Collaborative Study Group. Am J Pathol 1996;148:623-30. [PMC free article] [PubMed] [Google Scholar]
- 82.Sreekantaiah C, Leong SP, Karakousis CP, et al. Cytogenetic profile of 109 lipomas. Cancer Res 1991;51:422-33. [PubMed] [Google Scholar]
- 83.Pierron A, Fernandez C, Saada E, et al. HMGA2-NFIB fusion in a pediatric intramuscular lipoma: a novel case of NFIB alteration in a large deep-seated adipocytic tumor. Cancer Genet Cytogenet 2009;195:66-70. [DOI] [PubMed] [Google Scholar]
- 84.Bao L, Miles L. Translocation (1;4;12)(q25;q27;q15) in a childhood intramuscular lipoma. Cancer Genet Cytogenet 2005;158:95-7. [DOI] [PubMed] [Google Scholar]
- 85.Shimada S, Ishizawa T, Ishizawa K, et al. The value of MDM2 and CDK4 amplification levels using real-time polymerase chain reaction for the differential diagnosis of liposarcomas and their histologic mimickers. Hum Pathol 2006;37:1123-9. [DOI] [PubMed] [Google Scholar]
- 86.Bartuma H, Hallor K, Panagopoulos I, et al. Assessment of the clinical and molecular impact of different cytogenetic subgroups in a series of 272 lipomas with abnormal karyotype. Genes Chromosomes Cancer 2007;46:594-606. [DOI] [PubMed] [Google Scholar]
- 87.Rougraff BT, Durbin M, Lawerence J, Buckwalter K. Histologic correlation with magnetic resonance imaging for benign and malignant lipomatous masses. Sarcoma 1997;1:175-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Kransdorf MJ, Bancroft LW, Peterson JJ, et al. Imaging of fatty tumors: distinction of lipoma and well-differentiated liposarcoma. Radiology 2002;224:99-104. [DOI] [PubMed] [Google Scholar]
- 89.Jaovisidha S, Suvikapakornkul Y, Woratanarat P, et al. MR imaging of fat-containing tumours: the distinction between lipoma and liposarcoma. Singapore Med J 2010;51:418-23. [PubMed] [Google Scholar]
- 90.Gaskin CM, Helms CA. Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): results of MRI evaluations of 126 consecutive fatty masses. AJR Am J Roentgenol 2004;182:733-9. [DOI] [PubMed] [Google Scholar]
- 91.Inampudi P, Jacobson JA, Fessell DP, et al. Soft-tissue lipomas: accuracy of sonography in diagnosis with pathologic correlation. Radiology 2004;233:763-7. [DOI] [PubMed] [Google Scholar]
- 92.Zamora MA, Zamora CA, Samayoa EA, et al. High-resolution ultrasonography in an aggressive thenar intramuscular lipoma. J Ultrasound Med 2005;24:1151-5. [DOI] [PubMed] [Google Scholar]
- 93.Paunipagar B, Griffith J, Rasalkar D, et al. Ultrasound features of deep-seated lipomas. Insights Imaging 2010;1:149-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Matsumoto K, Takada M, Okabe H, Ishizawa M. Foci of signal intensities different from fat in well-differentiated liposarcoma and lipoma: correlation between MR and histological findings. Clin Imaging 2000;24:38-43. [DOI] [PubMed] [Google Scholar]
- 95.Murphey MD, Arcara LK, Fanburg-Smith J. From the archives of the AFIP: imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation. Radiographics 2005;25:1371-95. [DOI] [PubMed] [Google Scholar]
- 96.Hosono M, Kobayashi H, Fujimoto R, et al. Septum-like structures in lipoma and liposarcoma: MR imaging and pathologic correlation. Skeletal Radiol 1997;26:150-4. [DOI] [PubMed] [Google Scholar]
- 97.Donato M, Vanel D, Alberghini M, Mercuri M. Muscle fibers inside a fat tumor: a nonspecific imaging finding of benignancy. Eur J Radiol 2009;72:27-9. [DOI] [PubMed] [Google Scholar]
- 98.Drevelegas A, Pilavaki M, Chourmouzi D. Lipomatous tumors of soft tissue: MR appearance with histological correlation. Eur J Radiol 2004;50:257-67. [DOI] [PubMed] [Google Scholar]
- 99.Otsuka H, Terazawa K, Morita N, et al. Thallium-201 chloride scintigraphy in soft tissue tumors. J Med Invest 2009;56:136-41. [DOI] [PubMed] [Google Scholar]
- 100.Lamagna B, Greco A, Guardascione A, et al. Canine lipomas treated with steroid injections: clinical findings. PLoS One 2012;7:e50234. [DOI] [PMC free article] [PubMed] [Google Scholar]