

Abstract
Background:
Opium dependence is one of the most challenging health problems in the developing countries as well as Iran. Among several health problems due to opium dependence, there are limited reports indicating the presence of lead in opium. The aim of this study is to investigate the blood lead level (BLL) in oral and inhalational opium dependents and its association with anemia.
Materials and Methods:
A cross-sectional study was done among 86 opium dependent patients who were referred to five large detoxification centers in Tehran city and 48 healthy individuals. BLL was assessed using the atomic absorption spectrometry technique. Multivariate analysis of variance and binary logistic regression analysis were performed for statistical assessment using SPSS version 18 for Windows.
Results:
The highest BLL was detected in oral opium dependent group (mean = 11.75, standard deviation (SD) = 6.06) in comparison to inhalational opium dependent group (mean = 7.07, SD = 3.61) and healthy control group (mean = 6.05, SD = 1.83). Anemia was detected in 38% of oral-opium dependent and 43% of inhalational-opium dependent group. Age (odds ratio (OR): 1.06, 95% confidence interval (CI): 1.03-1.09) and opium dependence (OR: 3.59, 95% CI: 1.69-7.59) were significant predictors of anemia in these patients (P < 0.001).
Conclusion:
The results of this study confirmed the higher BLL in opium dependents, especially with an oral form of consumption.
Keywords: Anemia, blood lead level, Iran, opium dependent
INTRODUCTION
Opium dependence is one of the most challenging health problems in the developing world as well as Iran.[1] Over many decades, opium has been the most frequently abused substance in Iran and more than 2 million people use opiates.[2] The adverse consequences of opium use were clearly described as physical, mental, and psychiatric disorders.[3]
Among several health problems due to opium dependence, there are some reports indicating unusual pathologic findings such as abdominal pain, anemia, and kidney impairment in opium addicts.[4,5,6,7] These findings suggest a non-traditional source of exposure to lead.
Lead is a prevalent heavy metal with severe toxic effects for human.[8] The major routes of exposure to lead are through ingestion and inhalation.[9] After exposure, lead will be accumulated in blood, soft-tissues and bone, and may cause several signs and symptoms such as anemia, renal failure, hearing loss, impaired immune system, and decline of neurocognitive function.[10]
The first report of the presence of lead in opium backed to 1973 due to ingestion of home-made opium.[11] In recent times, few case-report studies have reported lead poisoning as a consequence of opium addiction in Iran.[6,7] Salehi et al. studied blood lead level (BLL) in 22 orally opium addicted patients with 22 healthy controls. They concluded that addicted patients have an elevated BLL compared with healthy controls.[12] In another study, Hayatbakhsh Abbasi et al. compared BLL in 50 inhalational-opium dependent to 43 nondependents. They failed to find any significant relationship between opium consumption and serum level of lead, but the concentration of lead in dependent group was higher than controls.[13] The existence of lead was approved in 10 opium samples in Kerman province with a mean concentration of 1.88 ± 0.35 PPM.[14]
However, these studies have limited value due to the low sample size and comparing just one form of opium consumption (inhalation or ingestion) with a healthy population. The high frequency of opium dependence in Iran and potential severity of lead exposure, prompted us to examine BLL in three groups, consisting of two forms of opium dependence (ingestion and inhalation) in comparison to healthy individuals and to investigate its association with anemia.
MATERIALS AND METHODS
In this cross-sectional study, we studied 86 opium dependent patients who were referred to five large detoxification centers in Tehran city. Between January 2009 and February 2010, all referral opium-dependent patients were examined and participants who met the inclusion criteria were enrolled.
Eligibility criteria included diagnosis of opium dependence based on diagnostic and statistical manual of mental disorder-IV criteria[15] for at least 6 months, age more than 18 years and consenting to participate. Persons working in mines or manufacturing industries with lead exposure, such as battery factories, foundries, wire factories or working with batteries, solder, ammunitions, paint, car radiators, cable, wires, and ceramic with lead glazes were excluded. Using a simple random sampling by Microsoft Excel software, 46 patients were recruited in inhalational opium dependent, 40 patients in oral opium dependent group.
Control group was selected among healthy participants from five premarriage consultation centers in Tehran city near the detoxification centers. Participants who had no history of opium dependence and lead exposure with negative urine morphine test were included in the control group. Forty-seven participants consented to participate and recruited.
For the measurement of BLL, 5 ml of blood was obtained from the antecubital vein and was collected in heparinized lead-free tubes. BLL of participants was measured using graphite furnace atomic absorption spectrometry technique.[16] The results were obtained as μg/dl.
Hemoglobin and hematocrit of the participants were assessed using a coulter AcT Diff Hematology Analyzer (Beckman-Coulter, High Wycombe, UK).
Statistical analysis
All descriptive statistics are presented as means and standard deviations (SDs) for quantitative variables, and as relative frequencies and percentages for categorical variables.
Multivariate analysis of variance was used to compare the mean of BLL and other hematologic factors in three groups (oral opium dependent, inhalational opium dependent and healthy individuals). A post-hoc (LSD) analysis was then used to analyze differences between groups.
Binary logistic regression analysis was applied to assess the predictors of anemia. Anemia was defined as a definition of the World Health Organization (WHO) (hemoglobin ≤12 g/dl for women, ≤13 g/dl for men).[17] Considering the presence of anemia as the dependent variable, the independent (predictor) variables were entered in the model, starting from the age of participants and followed by the BLL and opium dependence. The level of significance was set at P < 0.05 and all tests were two-tailed. The analysis of data was performed by the predictive analytic software (PASW Statistics 18) for Windows.
Ethics
The design of the study was approved in Ethics Committee of Vice Chancellor for Research, Tehran University of Medical Sciences (Project No. 105). All participants received trial information and provided written informed consent. Furthermore, researchers managed the confidentiality of all information carefully.
RESULTS
Demographic characteristics
In all, 134 participants fulfilled the study's inclusion criteria and enrolled. The study population consisted of 46 patients who were inhalational opium dependents, 40 oral opium dependents and 47 healthy individuals. All of them were men. The mean age of all participants was 33.5 (SD = 16.51) with a range of 22-84 years. Using analysis of variance, there was no statistically significant difference between three groups regarding to age (P = 0.67).
BLL
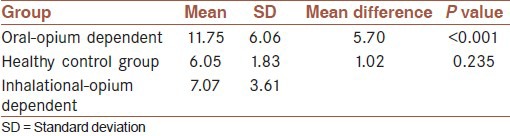
In the healthy control group, the mean of BLL was 6.05 (SD = 1.83). The BLL mean was the highest in the oral opium dependent group. There was a statistically significant difference between BLL in these three groups (P < 0.001).
The post-hoc analysis showed a statistically significant difference between oral opium dependent group with inhalational group and healthy participants (P < 0.001). However, the mean difference of BLL between healthy group and inhalational group was not significantly different (P = 0.23) [Table 1].
Table 1.
Mean of lead level in inhalational and oral opium dependents in comparison to the healthy group
Although the mean of BLL was higher in anemic group (8.98 [SD = 4.88] as compared to non-anemic group 7.79 [SD = 4.64]), this difference was not statistically significant (P = 0.216).
Predictors of anemia
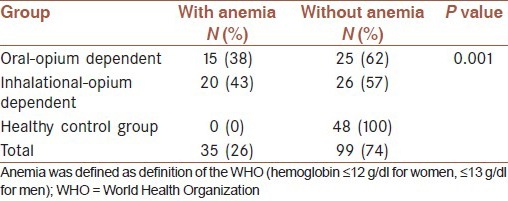
Using WHO definition, anemia was recognized in 35 (26.1%) participants. Among them, 20 participants were in inhalational group and 15 were oral opium-dependents. No one in the control group showed clinically and laboratory anemia manifestations. Chi-squared analysis showed a statistically significant difference in these groups (P < 0.001) [Table 2].
Table 2.
Frequency of anemia in in inhalational and oral opium dependents in comparison to the healthy group
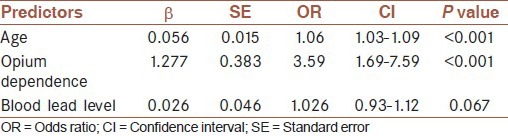
Binary logistic regression analysis showed that age and opium dependence was significant predictors of anemia. The lead level has no predictive role in the presence of anemia. The overall model was significant at the <0.001 level according to the model Chi-square statistic and explained 40% of the variation of the anemia [Table 3].
Table 3.
Logistic regression analysis for variables predicting anemia
DISCUSSION
The aim of this study was to compare the BLL in two groups of opium dependents in comparison to healthy control group and its association with anemia.
The results of our study showed that the BLL was higher in opium dependent participants in comparison to the healthy group. Oral-opium dependent group showed the highest BLL. This is in line with the results of Salehi et al.[12] and Amiri et al.[18] who reported a higher level of BLL in opium dependent group.
The higher level of lead in opium dependents may have several explanations. Some authors suggest it is due to contamination of opium with lead during its processing.[19] On the other hand, Iran is one of the key neighbors of Afghanistan-the major producer of opium in the world-and Iran is one of the main routes of world-wide opium transit. This make opportunity for drug producers and sellers to add some other substances such as lead to increase its weight for more profit.[14,20] Although these explanations make a sense about the source of lead in opium, but the exact source of lead in opium is still unknown.
In our study, the BLL in inhalational group was higher, but not statistically significant different from healthy control group. Previous studies show that the heat of smoking opium can affect the amount of lead absorbed in the blood.[13] In oral form of opioid consumption, the lead is not much affected and the blood absorption of lead can be higher in this method.
Among adults, greater absorption of lead can be achieved via lead ingestion during a period of fasting.[21] Rabinowitz et al.[22] have reported that 35% of lead will be absorbed in fasting period, in comparison to lower amounts (8.2%) if ingested with food.[22] In another study, Maddaloni et al. found a great difference in lead absorption between fasting (26.1%) and after eating (2.5%).[23] In Iran, most oral opium addicted patients consume opium in fasting with the highest lead bioavailability.
Lead is easily absorbed by the gastrointestinal tract and respiratory system and into the blood, bone and soft-tissues.[24] Higher level of BLL is associated with several clinical manifestations such as nausea, vomiting, constipation, abdominal pain, extremity pains, headache, paraesthesia, muscle weakness as well as anemia. In our study, anemia was present in 35 opium dependent patients (20 participants in inhalational group and 15 in oral opium dependent group). No one in the control group had anemia. Among several factors, age and group of participation were significant predictors of anemia. The results of this study are in line with previous ones that showed a particularly noticeable increase in prevalence of anemia in the oldest subjects.[25]
However, the pathogenesis of anemia in these patients is not completely understood. Some authors suggest that improper feeding, lack of self-care, inadequate diet would cause anemia in opium dependent group.[26] Lead absorption from the gastrointestinal tract is also increased in malnutrition and iron deficiency states.[27] Lead will produce anemia by two mechanisms: Impairment in heme biosynthesis, and increased rate of red blood cell destruction. A recent study proposed that low level of lead can induce phosphatidylserine exposure and erythrophagocytosis that may act as a mechanism underlying lead-associated anemia.[28] However, in our study, BLL was not a significant predictor of anemia. This may be due to the low frequency of anemia in our sample that reduced the power of study to investigate the role of lead in producing anemia. More research, particularly with large sample size, is warranted to direct the causation between BLL and anemia.
CONCLUSION
The results of this cross-sectional study confirmed the higher level of BLL in opium dependents, especially in oral form of consumption. Opium addiction is one of the most prevalent forms of addiction in Iran and there is a large population of opioid users who are potentially at risk of lead toxicity. The higher level of BLL in opium dependents is a warning to policy makers and health care workers about the possibility of lead poisoning in these patients. This needs a systematic effort to combat the opium smuggling-illegal opium importation and sale-to mitigate health risks by ensuring product quality; and reduce opium use by expanding rehabilitation centers.
AUTHOR'S CONTRIBUTION
BHD contributed in the conception of the work, conducting the study, data collection, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. NT contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. NJ contributed in the conception of the work, data analysis, drafting and revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
ACKNOWLEDGMENT
This manuscript is the first report of the dissertation project numbered 105 founded by the Vice Chancellor for Research, Tehran University of Medical Sciences. We are grateful to the time and the dedication of all the research coordinators and research assistants and for the generous donation of our participants.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Board INC. United Nations Publications; 2009. [Last accessed on 2013 March 31]. Report of the International Narcotics Control Board for 2008. Available at: http://www.incb.org/pdf/annual-report/2008/en/AR_08_English.pdf . [Google Scholar]
- 2.Malekinejad M, Vazirian M. Transition to injection amongst opioid users in Iran: Implications for harm reduction. Int J Drug Policy. 2012;23:333–7. doi: 10.1016/j.drugpo.2011.09.001. [DOI] [PubMed] [Google Scholar]
- 3.Strang J, Bearn J, Farrell M, Finch E, Gossop M, Griffiths P, et al. Route of drug use and its implications for drug effect, risk of dependence and health consequences. Drug Alcohol Rev. 1998;17:197–211. doi: 10.1080/09595239800187001. [DOI] [PubMed] [Google Scholar]
- 4.Froutan H, Zadeh AK, Kalani M, Andrabi Y. Lead toxicity: A probable cause of abdominal pain in drug abusers. Med J Islam Repub Iran. 2011;25:16–20. [Google Scholar]
- 5.Shiri R, Ansari M, Ranta M, Falah-Hassani K. Lead poisoning and recurrent abdominal pain. Ind Health. 2007;45:494–6. doi: 10.2486/indhealth.45.494. [DOI] [PubMed] [Google Scholar]
- 6.Fatemi R, Jafarzadeh F, Moosavi S, Afshar Amin F. Acute lead poisoning in an opium user: A case report. Gastroenterol Hepatol Bed Bench. 2008;1:99–101. [Google Scholar]
- 7.Verheij J, Voortman J, van Nieuwkerk CM, Jarbandhan SV, Mulder CJ, Bloemena E. Hepatic morphopathologic findings of lead poisoning in a drug addict: A case report. J Gastrointestin Liver Dis. 2009;18:225–7. [PubMed] [Google Scholar]
- 8.Pourmand A, Khedir Al-Tiae T, Mazer-Amirshahi M. Perspective on lead toxicity, a comparison between the United States and Iran. Daru. 2012;20:70. doi: 10.1186/2008-2231-20-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hu H, Shih R, Rothenberg S, Schwartz BS. The epidemiology of lead toxicity in adults: Measuring dose and consideration of other methodologic issues. Environ Health Perspect. 2007;115:455–62. doi: 10.1289/ehp.9783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gidlow DA. Lead toxicity. Occup Med (Lond) 2004;54:76–81. doi: 10.1093/occmed/kqh019. [DOI] [PubMed] [Google Scholar]
- 11.Chia BL, Leng CK, Hsii FP, Yap MH, Lee YK. Lead poisoning from contaminated opium. Br Med J. 1973;1:354. doi: 10.1136/bmj.1.5849.354-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Salehi H, Sayadi AR, Tashakori M, Yazdandoost R, Soltanpoor N, Sadeghi H, et al. Comparison of serum lead level in oral opium addicts with healthy control group. Arch Iran Med. 2009;12:555–8. [PubMed] [Google Scholar]
- 13.Hayatbakhsh Abbasi MM, Ansari M, Shahesmaeili A, Qaraie A. Lead serum levels in opium-dependent individuals. Addict Health. 2009;1:106–9. [PMC free article] [PubMed] [Google Scholar]
- 14.Aghaee-Afshar M, Khazaeli P, Behnam B, Rezazadehkermani M, Ashraf-Ganjooei N. Presence of lead in opium. Arch Iran Med. 2008;11:553–4. [PubMed] [Google Scholar]
- 15.Gillespie NA, Neale MC, Prescott CA, Aggen SH, Kendler KS. Factor and item-response analysis DSM-IV criteria for abuse of and dependence on cannabis, cocaine, hallucinogens, sedatives, stimulants and opioids. Addiction. 2007;102:920–30. doi: 10.1111/j.1360-0443.2007.01804.x. [DOI] [PubMed] [Google Scholar]
- 16.Yee HY, Nelson JD, Jackson B. Measurement of lead in blood by graphite furnace atomic absorption spectrometry. J Anal Toxicol. 1994;18:415–8. doi: 10.1093/jat/18.7.415. [DOI] [PubMed] [Google Scholar]
- 17.Benoist B, McLean E, Egll I, Cogswell M. Geneva: World Health Organization; 2008. Worldwide Prevalence of Anaemia 1993-2005: WHO Global Database on Anaemia. [Google Scholar]
- 18.Amiri M, Amini R. A comparison of blood-lead level (BLL) in opium-dependant addicts with healthy Control Group using the graphite furnace/atomic absorption spectroscopy (GF-AAS) followed by chemometric analysis. Iran Red Crescent Med J. 2012;14:488–91. [PMC free article] [PubMed] [Google Scholar]
- 19.Karrari P, Mehrpour O, Abdollahi M. A systematic review on status of lead pollution and toxicity in Iran; Guidance for preventive measures. Daru. 2012;20:2. doi: 10.1186/1560-8115-20-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Soltaninejad K, Flückiger A, Shadnia S. Opium addiction and lead poisoning. J Subst Use. 2011;16:208–12. [Google Scholar]
- 21.Ahamed M, Siddiqui MK. Environmental lead toxicity and nutritional factors. Clin Nutr. 2007;26:400–8. doi: 10.1016/j.clnu.2007.03.010. [DOI] [PubMed] [Google Scholar]
- 22.Rabinowitz MB, Kopple JD, Wetherill GW. Effect of food intake and fasting on gastrointestinal lead absorption in humans. Am J Clin Nutr. 1980;33:1784–8. doi: 10.1093/ajcn/33.8.1784. [DOI] [PubMed] [Google Scholar]
- 23.Maddaloni M, Lolacono N, Manton W, Blum C, Drexler J, Graziano J. Bioavailability of soilborne lead in adults, by stable isotope dilution. Environ Health Perspect. 1998;106(Suppl 6):1589–94. doi: 10.1289/ehp.98106s61589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patrick L. Lead toxicity, a review of the literature. Part 1: Exposure, evaluation, and treatment. Altern Med Rev. 2006;11:2–22. [PubMed] [Google Scholar]
- 25.Beghé C, Wilson A, Ershler WB. Prevalence and outcomes of anemia in geriatrics: A systematic review of the literature. Am J Med. 2004;116(Suppl 7A):3S–10S. doi: 10.1016/j.amjmed.2003.12.009. [DOI] [PubMed] [Google Scholar]
- 26.Haghpanah T, Afarinesh M, Divsalar K. A review on hematological factors in opioid-dependent people (opium and heroin) after the withdrawal period. Addict Health. 2010;2:9–16. [PMC free article] [PubMed] [Google Scholar]
- 27.van der Klooster JM. A medical mystery. Lead poisoning. Singapore Med J. 2004;45:497–9. [PubMed] [Google Scholar]
- 28.Jang WH, Lim KM, Kim K, Noh JY, Kang S, Chang YK, et al. Low level of lead can induce phosphatidylserine exposure and erythrophagocytosis: A new mechanism underlying lead-associated anemia. Toxicol Sci. 2011;122:177–84. doi: 10.1093/toxsci/kfr079. [DOI] [PubMed] [Google Scholar]