

Abstract
A 7 month infant presented with fever and breathlessness with raised total counts. Examination revealed 90 % blasts with prominent nucleoli. Flow cytometry revealed a tight cluster in the monocytic region. The blasts showed homogenous bright CD 33/4/64/HLA D with heterogeneous expression of CD14/15/11c. Blasts were negative for CD13/MPO/Cytoplasmic CD3/19/7/34/117/5/22/TdT/CD 61/41. FISH revealed MLL gene rearrangements in the blasts. No evidence of Down’s syndrome on cytogenetic studies was noted. Diagnosis of Infantile acute monoblastic leukemia was made. These leukemias are rare in infants and are associated with a poor outcome.
Keywords: Acute leukemia, Infantile, Monoblastic, MLL
A 7 month old male infant presented with fever and breathlessness. On examination, child had pallor. Hemogram revealed hemoglobin of 4.6 g/dL, TLC 1.64 lacs/cu mm, platelet counts of 90,000 per cu mm with 90 % blasts, having high nucleo cytoplasmic ratios, vesicular chromatin and prominent nucleoli (Fig. 1). A provisional diagnosis of acute leukemia was made with differentials of infantile acute lymphoblastic leukemia/acute myeloid leukemia (AML)/mixed phenotype acute leukemia.
Fig. 1.
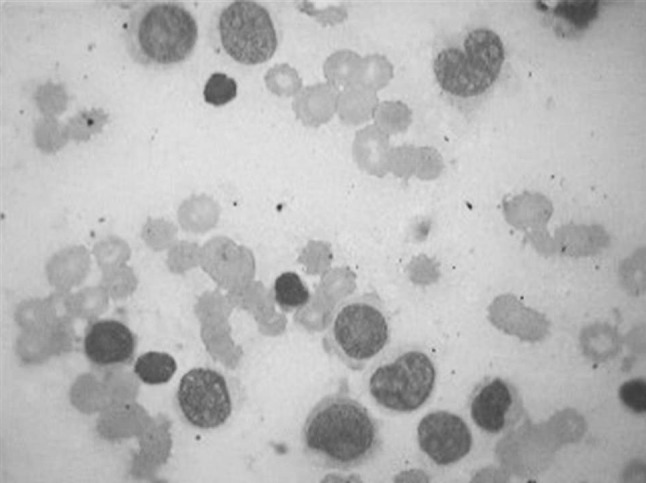
Peripheral smear showing blasts with high N/C ratios, vesicular chromatin and prominent nucleoli (Giemsa, 100×)
Cytochemistry showed NSE positive in majority of blasts with occasional blast showing MPO staining.
Flow cytometry revealed a tight cluster in the monocytic region. The blasts showed homogenous bright CD 33/4/64/HLA D with heterogeneous expression of CD14/15/11c. Blasts were negative for CD13/MPO/Cytoplasmic CD3/19/7/34/117/5/22/TdT/CD 61/41(Fig. 2).
Fig. 2.

Flow cytometric plots showing tight cluster in monocytic region (1st plot, displaying CD 45 Per CP on X axis vs SSC Y axis), Positivity for CD 33 (2nd plot CD 33 PE, Y axis vs CD 34 FITC), HLA DR (3rd plot, HLA DR APC on Y axis vs CD 45 X axis), CD4, 64 (4th plot showing co expression of CD 4 APC, Y axis vs CD 64 FITC, X axis), 11c (5th plot showing CD 11c PE, Y axis vs CD 45 Per CP, X axis) and positive MLL rearrangement on FISH (last plot, break apart probe for MLL)
FISH revealed MLL gene rearrangements in the blasts. No evidence of Down’s syndrome on cytogenetic studies was noted.
A diagnosis of Infantile AML M5 was made and multi drug chemotherapy initiated. The child unfortunately succumbed to the disease. Infantile M5 have an incidence of 0.8–1.1 per million per year. Predisposing factors include Congenital (Downs/KF/Fanconi/Blooms etc.) and acquired factors such as prenatal exposure to tobacco, alcohol, chemo/radiation etc.
MLL rearrangements are common [1], and identify a subset of cases that will respond poorly to chemotherapy and have poorer prognosis. Commonest abnormality is t (9; 11), MLL T3.
References
- 1.Bower M, Parry P, Carter M, Lillington DM, Amess J, Lister TA, Evans G, Young BD. Prevalence and clinical correlations of MLL gene rearrangements in AML-M4/5. Blood. 1994;84(11):3776–3780. [PubMed] [Google Scholar]