

Abstract
Background:
Heart failure is incurable disease and patients often have an ongoing decline once diagnosed. The symptoms of heart failure may impair the ability of patient to perform activities of daily living. As heart failure progresses, patients normally increase their reliance on family caregivers.
Aims:
This paper explored the informational needs and related problems of family caregivers of heart failure patients as a part of the findings of a study exploring experiences of family caregivers in the caregiving situation.
Setting and Design:
Using a qualitative design, 19 family caregivers from three educational hospitals in Isfahan, Iran, were recruited.
Materials and Methods:
Participants were selected by purposive sampling. Data were collected through semi-structured interviews. Interviews were transcribed verbatim and analyzed concurrently.
Results:
Four major themes were emerged from the analysis of the transcripts: “Lack of care-related knowledge”, “Inaccessibility to responsible source of information”, “Lack of guidance from healthcare team” and “caring with ambiguity due to unpredictable nature of the disease”. Caregivers believed that they did not have the basic knowledge related to disease and medication administration. They received little guidance and support from the health care team on the caregiving roles. They experienced high level of ambiguity and stress in caregiving tasks due to lack of care-related knowledge and unpredictable nature of disease.
Conclusion:
The care, which was performed by the caregivers of HF patients, is beyond of their knowledge, capabilities, and resources. Nurses and other healthcare providers can use the findings of this study to develop effective educational and supportive programs to facilitate these needs.
Keywords: Family caregivers, heart failure, information needs, Iran, nursing
INTRODUCTION
Heart failure (HF) is a chronic disease resulting from a functional cardiac disorder, which impairs the ventricles’ ability to pumping blood.[1] It is estimated that 15 million people in Europe and more than 5.8 million people in the United States suffer from HF.[2,3] According to the Iranian Health Ministry's Management Center for Non-Communicable Diseases, the number of patients living with HF will increase to 3500 cases per 100,000 people in the near future.[4] Patients may become unable to continue self-care and require caregiving as heart failure progresses. Millions of family members are serving as caregivers for patients with HF.[5,6,7] Family caregivers may have a high-extended range of duties, such as medication administration, symptom monitoring, bathing, and transportation of HF patients, which require adequate care-related knowledge, capabilities, and resources.[8,9] Family caregiving is an essential factor to the health of each country. Without family caregivers, the healthcare system would be unable to meet the needs of chronically ill patients such as HF.[9,10] Availability and training of family caregivers of HF patients have a considerable impact on professional care delivery, health care and family costs reduction.[3,8,9] In Iran, despite the growing prevalence and incidence of HF, little is known about the challenges and needs of HF family caregivers in the caregiving situation. There are no supportive and educative resources for them in the current health care system. Iranian nursing studies about the HF context specifically focus on the patients’ care, while considering the patients’ families and their needs are necessary as well. For example, researchers have studied the quality of life,[11] the learning needs,[12] the self-care knowledge of HF patients,[13] and the application of the readmission caring model to control complications of patients with congestive heart failure.[4]
Furthermore, many studies about the HF family caregivers’ needs have been conducted at western countries especially in the USA, which showed several informational needs of HF caregivers.[14,15,16] Pinquart and Sörensen[17] and Dunbar[9] were asserted that family roles and needs in the family caregiving situation were influenced by socio-cultural factors and worldviews.[9,17]
To develop effective programs to help the caregivers, and to measure effectiveness of programs to promote caregivers’ care-related capabilities, we need an understanding of the characteristics of the caregiving needs among various ethnic groups and societies. Therefore, the researchers were interested to explore the informational needs and related problems of family caregivers of heart failure patients as a part of the findings of a study exploring experiences of family caregivers in the caregiving situation.
MATERIALS AND METHODS
This inquiry as a part of a PhD dissertation was conducted by a qualitative content analysis approach in order to present an authentic insight into peoples’ experiences. Current study was conducted at three educational hospitals in Isfahan, Iran, which are the main centers for cardiovascular disease treatment. Nineteen family caregivers were selected purposively after obtaining written; informed consent from all of them. They were 18 years or older and they were primary caregivers with several months experience in caregiving. They did not serve as a caregiver for other family members concurrently. Caregivers with physical or psychological disorders and inability to communicate were excluded from the study.
The staff of the cardiac wards helped the researchers by introducing caregivers who were able to describe their experiences. Those who were invited to participate in the study represented a maximum variation in demographic data and their experiences in the caregiving situation.
Data were collected through semi-structured interviews from February to June 2012. All interviews took place in a private setting, which was selected by the participants; 16 interviews at the hospital, and three interviews were conducted at the participants’ work place. Each interview began with an open question: “Tell me about your experiences in caring of this patient.” The next questions were based on the participant's response to the first question, for example “Explain about your needs in the caring situation,” or “Tell me about your problems in the caring situation. The interviews lasted between 23 and 60 min; all of them were recorded using a digital audio system and transcribed verbatim.
The research process was based on the inductive reasoning and the data collecting continued until no new information were emerged. Data saturation was achieved thorough 19 interviews.
The data were analyzed thematically in order to identify major themes and to reflect the participants’ experiences.[18] The data collection and analysis were carried out concurrently. It began with the first interview, which leads the researchers to ask more probing questions in the subsequent interviews.
The data analysis began by reading the transcripts several times and comparing with the recorded data to ensure the accuracy of the transcription. Then, using constant comparative data analysis, each transcript was coded individually. The codes were compared to identify similarities and differences.[19] In order to form subthemes and themes, the similar codes were grouped together.
This study applied Denzin and Lincolns’[20] model of trustworthiness.[20] Credibility was enhanced through the prolonged engagement with the caregivers, discussion of findings among the research team, and checks the transcripts codes with all of the participants. Transferability was strengthened using maximum variation in selecting the participants from three hospitals. Confirmability was enhanced through the reflective memos to develop an audit trail of the research activities that were made through the research process. Dependability was strengthened by engaging three experienced co-researchers in data analysis.
The Ethics Committee of Isfahan University of Medical Sciences approved the study. The participants were received verbal and written information about the purpose of the study. They were free to withdraw from the study at any time.
RESULTS
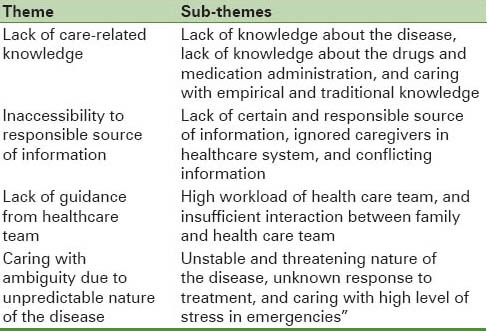
In total, 19 family caregivers participated in the study. Their mean age was 42 years (range from 20-50 years). A majority of them was female (78.94%), married (57.89%), and was patients’ daughter or spouse (68.41%) with primary and middle year of education (63.15%). The mean time that the caregivers enrolled to care the patient was 8.5 hours (range, 1-15 hour) per day [Table 1]. The overall analysis of the data produced the four following themes based on the participants’ information needs in the caregiving situation: “lack of care-related knowledge”, “inaccessibility to responsible source of information”, “lack of guidance from healthcare team” and “caring with ambiguity due to unpredictable nature of the disease” [Table 2].
Table 1.
Characteristics of family caregivers of patients with heart failure
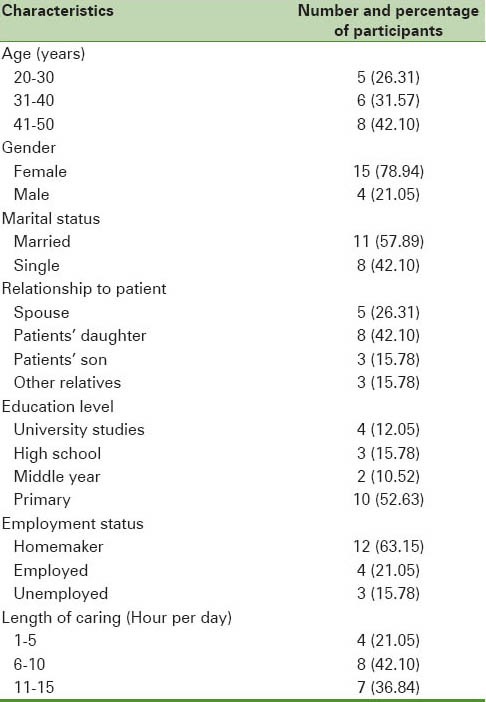
Table 2.
Information needs of caring for patients with heart failure in perspective of Iranian family caregivers
Lack of care-related knowledge
This was a major theme in explaining the concept of family caregivers’ informational needs. The subthemes of this theme were “lack of knowledge about the disease”, “lack of knowledge about the drugs and medication administration”, and “caring with empirical and traditional knowledge”.
Lack of knowledge about the disease
Most of the participants noted that they did not have the basic knowledge about the disease, sign and symptoms, prognosis and complications.
I had known his heart did not work well, but I did not know what his problem is actually. Why his breath shortened at night or his leg swallowed constantly… (caregiver 3).
Another participant said: Sometimes I ask myself, why his condition gets worse day-to-day despite of all of the treatments … perhaps, it may not be therapeutic, and the rest of his body will be damaged (caregiver 6).
Lack of knowledge about the drugs and medication administration
Family caregivers stated that they did not have the basic knowledge about the drugs side effects, and medication administration. They believed that their patients have a multiple drugs on several times, which will confuse them when they want to give on patients.
We have a cabinet, which is full of the cardiac drugs at home. Because they are too many, I do not know the names. I do not know about the side effects when I give them (caregiver 9).
Due to the family caregivers’ knowledge deficit about the drugs, despite of appearing the side effects of drugs, they continued giving the drugs and finally the patient was referred to the hospital with severe drug side effects such as hemorrhage or cardiac arrhythmia. For example, one caregiver said:
A few days ago, I saw several blood spots under the skin of her hands. I did not know these are related to what. We have transferred her to the hospital due to her nose bleeding. In the hospital, I realized that Warfarin could cause bleeding and even death to the patient (caregiver 7).
Caring with personal and traditional knowledge
Caregivers noted that their little care-related knowledge was formed during the patient care and in many cases; they are not sure about the accuracy of their activities on the caregiving situation.
I had learned a few things gradually. I care for her using my own experiences, some times; I think that my care is incorrect and therefore she is getting worse (caregiver 13).
Inaccessibility to responsible source of information
This is another theme. The subthemes of this theme were “lack of certain and responsible source of information”, “ignored caregivers in healthcare system” and “conflicting information”.
Lack of certain and responsible source of information
Although most of the caregivers attempted to receive more care-related information especially in the hospital, but this need usually remained unmeet:
We has been hospitalized him on different hospitals several times. However, there is no certain place for us, which we will refer to it and ask our questions about the caregiving (caregiver 9).
Ignored caregivers in healthcare system
Caregivers believed that the healthcare teams have a lot to do and were unable to pay attention on the caregivers’ needs. According to them, the healthcare team more follows the patient needs and usually forgets the family.
In the hospital, no one listen to us…I asked them [the healthcare team] how to help him to be healthy again? …But nobody considers our questions…It seems like that we have been forgotten (caregiver 19).
Unreliable information
Caregivers believed that due to lack of certain and responsible source of information, they have to capture care-related information from all possible ways. This information often is inconsistent and lead to caregivers’ uncertainty in caregiving.
When I ask a same question about my patient's condition such as her shortness of breath. I receive a different answer from each of them. I do not know about the correct answer (caregiver 16).
Lack of guidance from healthcare team
Another derived theme from the experiences of caregivers was lack of guidance from the healthcare team. The subthemes of this theme were “high workload of health care team” and “insufficient interaction between family and health care team”.
High workload of health care team
Caregivers noted that due to high workload of medical staffs, and the large number of patients, which were admitted to the governmental hospitals, the staffs did not have enough time for considering the caregivers’ challenges.
The number of patients is very much in comparison of the number of medical staffs in the governmental hospitals. They have little time for each patient (caregiver 17).
Insufficient interaction between family and health care team
Caregivers believed that the level of interaction between them and health care team is not adequate for eliminating the caregivers’ informational needs. Moreover, they noted that due to managerial barriers, they could not stay at patient room during patient's visit and they are not sufficiently aware of their patient's condition.
When doctor come here for patients’ visit, they tell us “please exit from the ward until the doctor finishes the visits”. I want to know how and where we should aware from our patients’ condition. Without this how I can care him at home (caregiver 12).
Caring with ambiguity due to unpredictable nature of the disease
This is another theme. The sub themes of this theme were “unstable and threatening nature of the disease”, “unknown response to treatment” and “caring with high level of stress in emergencies”.
Unstable and threatening nature of the disease
Caregivers noted that the patients’ condition and their signs and symptoms were changing continuously and they did not know how to manage emergencies such as severe dyspnea and blood pressure crisis.
Sometimes, when he is sleeping, I take a mirror over his mouth to be sure that he is breathing or when I want to cook; I will lay his bed in the kitchen to check his chest's movements (caregiver 3).
Unknown response to treatment
Due to prolongation of the treatments process and progresses of patients’ impairments, caregivers noted to a feeling of doubt and indecision regarding the ongoing treatment of their patients.
I don’t know how many years treatment should be continued, it may be cured by drugs or need to heart surgery (caregiver 13).
Caring with high level of stress in emergencies
Caregivers believed due to care-related knowledge deficit they do not know how manage the patients’ needs especially in the emergency such as chest pain, dyspnea, and drugs side effects.
When his breathing is shortened, I think that this is his last breaths and my patient may be lost at any moment. I have a lot of stress and I do not know what to do (caregiver 19).
DISCUSSION
This is the first qualitative study that explored the informational needs and related problems of family caregivers of heart failure patients as a part of study exploring experiences of family caregivers in the caregiving situation; it is aimed to provide a deeper understanding of their challenges on caregiving situation.
As presented in the results, four main themes were derived. Lack of care-related knowledge formed an important element of the informational needs of family caregivers of heart failure patients. This common type of caregivers’ knowledge deficit reflected the need for information that usually must be provided by healthcare team about the disease, drugs, medication administration, and caregiving tasks. In this study, lack of knowledge about the disease, drugs and medication administration were similar to the findings of the previous studies.[14,16,21]
Moreover, caring with personal and traditional knowledge was a new finding in this study that contributed to more caregivers’ distress and uncertainty about the accuracy of their activities in the caregiving situation. Several studies concluded that caregivers did not know how to assume the caregiving roles and they were not familiar with the type and amount of care, which was needed. These studies mentioned that caregivers required sufficient care-related knowledge to provide safety care, to cope with caregiving roles, and to reduce their distress.[15,22,23]
Another important issue as a new finding was inaccessibility to responsible source of information that emerged in this study. Although most of the caregivers wanted to achieve more care-related information especially in the medical centers, but due to absence of certain educative and supportive center for them, this need usually remained unmeet. Thus, caregivers have little chance to receive reliable information and caregiving was continued with personal knowledge and uncertainty. Caregivers believed that existence of a family care center in the hospitals when their patients are admitted is a very practical way for providing them more caregiving information. The provision of appropriate care-related knowledge to family caregivers could be a crucial step towards reducing caregivers’ uncertainty and stress that would improve the quality of caregiving.[22]
Another important theme was lack of guidance from healthcare team that emerged in this study which was similar to the findings of previous studies. In Iran, most of the HF patients are admitted in governmental hospitals where,[24] there is a lot of workload and lack of time; therefore, the healthcare team has little opportunity to address the caregivers’ informational needs and challenges of caregiving. This thread identifies the need to establish a family center care in order to enhance the interaction between the health team and family caregivers especially in the governmental hospitals. This in turn provides more care-related knowledge and support for caregivers.
Family caregivers need working knowledge of the patient's plan of care and they must be able to interact with nurses and social workers. Health care providers should complete a formal skill assessment of caregivers as part of the plan to determine what training and supports are needed. Assessing caregivers’ capacity to provide care and identifying caregivers who need assistance is essential to improving patient care.[21,25]
Caring with ambiguity due to unpredictable nature of the disease is a new finding in this study. Current situation of caregiving without adequate care-related knowledge, accessibility to certain and scientific source of information, inadequate interaction with health care team, and threatening nature of the disease caused a stressful caregiving situation for the caregivers. Nurses and healthcare provider should assess the caregiving situation and help the family caregivers to develop their care-related knowledge, capabilities and to provide more support on them. This in turn caregivers report lower levels of burden and stress.
LIMITATIONS
This study has some limitations. Although the researchers attempted to consider maximum sample variation by selecting the participants from various demographic characteristics, the sampling population was limited to three governmental medical centers. It was a purposive non-probability sampling method. These issues might limit the generalizability of our results. Current study included small sample, in order to increase transferability, a larger sample of the family caregivers from a wide population including both private and governmental hospitals should be recruited in future surveys.
CONCLUSIONS
Quality of patients’ care is reduced in situations where the basic care-related knowledge and reliable source of information are not available for the caregivers and these contribute to the caregivers’ uncertainty and stress as well as deteriorate the patients’ conditions. Health professionals need to help family caregivers acquire more care-related knowledge, capabilities, and resources while keeping in mind cultural and ethnic differences. This information is vital for planning and implementing interventional programs that will help them. Translating care-related knowledge and related problems into family caregiving context establishes best practices.
Footnotes
Source of Support: This study was supported by the Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): Developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: Endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–235. doi: 10.1161/CIRCULATIONAHA.105.167586. [DOI] [PubMed] [Google Scholar]
- 2.Clark AM, Savard LA, Spaling MA, Heath S, Duncan AS, Spiers JA. Understanding help-seeking decisions in people with heart failure: A qualitative systematic review. Int J Nurs Stud. 2012;49:1582–97. doi: 10.1016/j.ijnurstu.2012.05.010. [DOI] [PubMed] [Google Scholar]
- 3.Hwang B, Luttik ML, Dracup K, Jaarsma T. Family caregiving for patients with heart failure: Types of care provided and gender differences. J Card Fail. 2010;16:398–403. doi: 10.1016/j.cardfail.2009.12.019. [DOI] [PubMed] [Google Scholar]
- 4.Hekmatpou D, Mohammadi E, Ahmadi F, Arefi S. The effectiveness of applying “Making Sensivity to Re-admission Caring Model” on controlling congestive heart failure complications among hospitalized patients in Tehran cardiovascular centers. Med J Iran Univ. 2009;17:33–49. [Google Scholar]
- 5.Jeon YH, Kraus SG, Jowsey T, Glasgow NJ. The experience of living with chronic heart failure: A narrative review of qualitative studies. BMC Health Serv Res. 2010;10:77. doi: 10.1186/1472-6963-10-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Molloy GJ, Johnston DW, Witham MD. Family caregiving and congestive heart failure. Review and analysis. Eur J Heart Fail. 2005;7:592–603. doi: 10.1016/j.ejheart.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 7.Pressler SJ, Gradus-Pizlo I, Chubinski SD, Smith G, Wheeler S, Wu J, et al. Family caregiver outcomes in heart failure. Am J Crit Care. 2009;18:149–59. doi: 10.4037/ajcc2009300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Saunders MM. Factors associated with caregiver burden in heart failure family caregivers. West J Nurs Res. 2008;30:943–59. doi: 10.1177/0193945908319990. [DOI] [PubMed] [Google Scholar]
- 9.Dunbar SB, Clark PC, Quinn C, Gary RA, Kaslow NJ. Family influences on heart failure self-care and outcomes. J Cardiovasc Nurs. 2008;23:258–65. doi: 10.1097/01.JCN.0000305093.20012.b8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bakas T, Pressler SJ, Johnson EA, Nauser JA, Shaneyfelt T. Family caregiving in heart failure. Nurs Res. 2006;55:180–8. doi: 10.1097/00006199-200605000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Rahnavard Z, Zolfaghari M, Kazemnejad A, Hatamipour K. An investigation of quality of life and factors affecting it in the patients with congestive heart failure. J Fac Nurs Midwifery Tehran Univ Med Sci. 2006;12:77–86. [Google Scholar]
- 12.Rafii F, Shahpoorian F, Naasher Z, Azarabaad M, Hosseini F. The importance of learning needs of congestive heart failure patients from patients’ and nurses’ perspective. Iran Nurs J. 2009;22:19–30. [Google Scholar]
- 13.Habibollahzade H, Baghaei R, Abolfathi L, Gasemzade P. Study on causes of heart failure and evaluation of knowledge and attitude towards the disease. J Med Counc Islam Repub Iran. 2001;19:85–9. [Google Scholar]
- 14.Walden JA, Dracup K, Westlake C, Erickson V, Hamilton MA, Fonarow GC. Educational needs of patients with advanced heart failure and their caregivers. J Heart Lung Transplant. 2001;20:766–9. doi: 10.1016/s1053-2498(00)00239-4. [DOI] [PubMed] [Google Scholar]
- 15.Clark AM, Freydberg CN, McAlister FA, Tsuyuki RT, Armstrong PW, Strain LA. Patient and informal caregivers’ knowledge of heart failure: Necessary but insufficient for effective self-care. Eur J Heart Fail. 2009;11:617–21. doi: 10.1093/eurjhf/hfp058. [DOI] [PubMed] [Google Scholar]
- 16.Hupcey JE, Fenstermacher K, Kitko L, Fogg J. Palliative needs of spousal caregivers of patients with heart failure followed up at specialized heart failure centers. J Hosp Palliat Nurs. 2011;13:142–50. doi: 10.1097/NJH.0b013e31820ce15e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pinquart M, Sörensen S. Ethnic differences in stressors, resources, and psychological outcomes of family caregiving: A meta-analysis. Gerontologist. 2005;45:90–106. doi: 10.1093/geront/45.1.90. [DOI] [PubMed] [Google Scholar]
- 18.Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. [Google Scholar]
- 19.Corbin G, Strauss A. London: Sage Publisher; 2008. Basics of qualitative research: Techniques and Procedures for developing grounded theory. [Google Scholar]
- 20.Denzin N, Lincoln Y. London: Sage Publisher; 2005. Handbook of qualitative research. [Google Scholar]
- 21.Luttik ML, Jaarsma T, Veeger N, Tijssen J, Sanderman R, van Veldhuisen DJ. Caregiver burden in partners of Heart Failure patients; limited influence of disease severity. Eur J Heart Fail. 2007;9:695–701. doi: 10.1016/j.ejheart.2007.01.006. [DOI] [PubMed] [Google Scholar]
- 22.Fukui S. Information needs and the related variables of Japanese family caregivers of terminally ill cancer patients. Nurs Health Sci. 2004;6:29–36. doi: 10.1111/j.1442-2018.2003.00170.x. [DOI] [PubMed] [Google Scholar]
- 23.Cox A, Hayter M, Ruane J. Alternative approaches to ‘enhanced observations’ in acute inpatient mental health care: A review of the literature. J Psychiatr Ment Health Nurs. 2010;17:162–71. doi: 10.1111/j.1365-2850.2009.01507.x. [DOI] [PubMed] [Google Scholar]
- 24.Salehitali SH, Dehkordi AH, Hafshejani SM, Jafarei A. The effect of continuous home visits and health education on the rate of readmissions, referrals, and Health Care Costs among Discharged Patients with Heart Failure. HAYAT. 2010;15:43–9. [Google Scholar]
- 25.Given B, Sherwood PR, Given CW. What knowledge and skills do caregivers need? Am J Nurs. 2008;108(Suppl 9):28–34. doi: 10.1097/01.NAJ.0000336408.52872.d2. [DOI] [PubMed] [Google Scholar]