

Abstract
Congenital anomalies of coronary arteries are a group of diseases that are infrequently found. Their prevalence has been reported from 0.6% to 1.3%. Most clinical manifestations are benign and asymptomatic. Congenital absence of the left circumflex artery is a very rare congenital anomaly of the coronary circulation, and only a few cases have been reported in the literature. We report a case of a 51-year-old man who underwent a cardiac catheterisation. Coronary angiography showed a left anterior descending coronary artery with no circumflex and a dominant right coronary artery.
Background
The congenital absence of the left circumflex artery (LCx) is a very rare anomaly, with uncertain incidence. There are very few cases reported in the literature.
Case presentation
A 51-year-old man with a history of type 2 diabetes, hypertension and obesity, was diagnosed, after an incidental finding, with abnormal repolarisation without clinical symptoms. An echocardiogram in 2010 had shown moderate left ventricular (LV) hypertrophy with a normal ejection fraction.
Investigations
ECG: sinus rhythm. T wave inversion in leads V3—4–5—6. Isoelectric T wave in leads II, III, aVF and I, and aVL.
Echocardiogram: non-dilated left ventricle. Normal LV systolic function. No alterations of segmentary motion. The remaining study was within normal limits.
Cardiac catheterisation was performed, which showed a normal left anterior descending (LAD) artery and absence of the LCx (figure 1; video 1). The patient had a dominant right coronary artery (RCA) with no coronary lesions. Interestingly, the circumflex artery was arising as a terminal extension of the posterolateral branch of the RCA (figure 2; videos 2 and 3)
Figure 1.
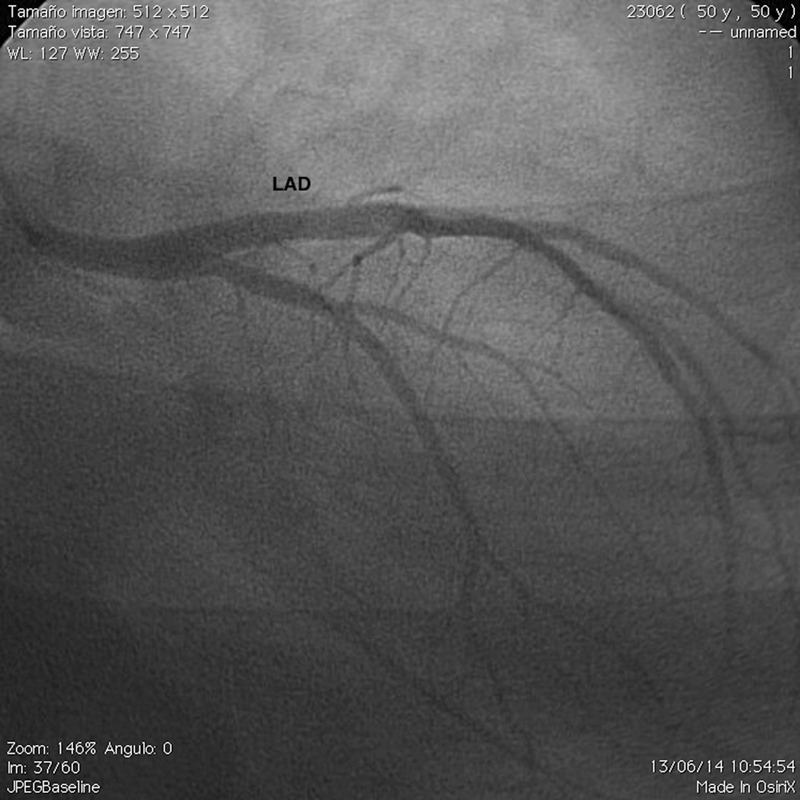
Left coronary angiogram with left interior descending. No left circumflex observed.
Figure 2.
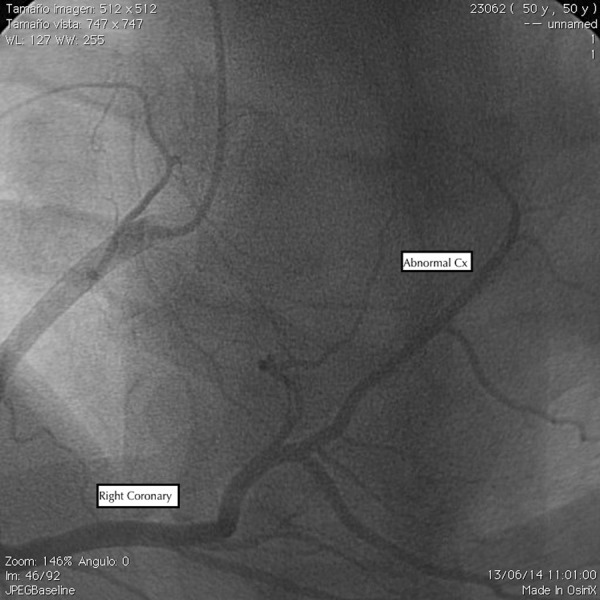
Right coronary angiogram with right coronary artery, with an abnormal left circumflex artery at the end.
Left coronary angiogram: LAD, left anterior descending.

Right anterior oblique 30°.

Right coronary angiogram showing large right coronary artery supplying left ventricular posterolateral wall.

Differential diagnosis
Proximal occlusion of LCx versus anomalous origin of LCx.
Discussion
Most anomalies are discovered as incidental findings during coronary angiographic study; 0.6–1.3% incidence rates have been reported in the literature. Yamanaka and Hobbs1 described 126 595 patients undergoing cardiac catheterisation between 1960 and 1988, in the largest of these studies.
Absent left circumflex coronary artery with superdominant RCA is a very rare anomaly, in which the left main coronary artery continues as LAD artery. The RCA is superdominant and courses retrogradely, supplying the left ventricle.2 3
Anomalous origin of the LCx is diagnosed when the artery is not visualised during left coronary injection in the absence of proximal occlusion, and the ostium of the circumflex artery appears from the right sinus Valsalva or, as in our case, as a continuation of the RCA, which goes through the atrioventricular groove.4–6
The anomaly of the LCx is defined as a benign condition and has no significant clinical symptoms, but in some cases published, the authors discovered patients who had symptoms, mainly after exertion. The aetiology of symptoms is not exactly known, but a ‘steal phenomenon’ appears as the most probably hypothesis. The detection of congenitally absent LCx is necessary because some patients have symptoms that are similar to those who have coronary disease.7 8
In conclusion, the congenital absence of the LCx is an extremely rare anomaly of coronary arteries. The diagnosis, in many cases, is from an incidental finding and, in most cases, is an asymptomatic entity.
Learning points.
Congenital absence of the left circumflex artery (LCx) is an extremely rare anomaly of coronary arteries.
Most anomalies are discovered as incidental findings during coronary angiographic study.
Congenital absence of LCx is defined, normally, as a benign condition.
This anomaly can cause ‘angina-like’ symptoms, particularly on exertion.
Footnotes
Contributors: AQ-F and RP-G were involved in drafting the article and wrote the final paper to be published. MR-E contributed with the design of the article and gave final approval until published.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21:28–40. 10.1002/ccd.1810210110 [DOI] [PubMed] [Google Scholar]
- 2.Doven O, Yurtdas M, Cicek D et al. Congenital absence of left circumflex coronary artery with superdominant right coronary artery. Anadolu Kardiyol Derg 2006;6:208–9. [PubMed] [Google Scholar]
- 3.Ilia R, Jafari J, Weinstein JM et al. Absent left circumflex coronary artery. Cathet Cardiovasc Diagn 1994;32:349–50. 10.1002/ccd.1810320413 [DOI] [PubMed] [Google Scholar]
- 4.Ueyama K, Ramchandani M, Beall AC et al. Diagnosis and operation for an anomalous circumflex coronary artery. Annals Thorac Surg 1997;63:377–81. 10.1016/S0003-4975(96)00766-7 [DOI] [PubMed] [Google Scholar]
- 5.Uyan C, Altinmakas S, Pektas O. Left circumflex coronary artery arising as a terminal extension of the right coronary artery. Acta Cardiol 2000;55:101–2. 10.2143/AC.55.2.2005729 [DOI] [PubMed] [Google Scholar]
- 6.Majid Y, Warade M, Sinh J et al. “Superdominant right coronary artery with absent left circumflex Artery”. Biomed Imaging Interv J 2011;7:e2 1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lin T, Lee W, Kong C et al. Congenital absence of the left circumflex coronary artery. Japan Heart J 2003;44:1015–20. 10.1536/jhj.44.1015 [DOI] [PubMed] [Google Scholar]
- 8.Hongsakul K, Suwannanon R. Congenital absence of left circumflex artery detected by computed tomography coronary angiography: a case report. Case Rep Vasc Med 2012;2012:204657, 3 pages. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Left coronary angiogram: LAD, left anterior descending.
Right anterior oblique 30°.
Right coronary angiogram showing large right coronary artery supplying left ventricular posterolateral wall.