

Abstract
INTRODUCTION
Wrist pain is very common and there are several causes for this condition. It is extremely important to establish an accurate diagnosis so that appropriate treatment can be directed at the cause.
PRESENTATION OF CASE
We describe a case of a young man who presented to us with wrist pain of insidious onset. He had previous (ganglion) excision from the same wrist. Clinically there was tenderness in the base of second metacarpal with no swelling. The radiograph and MRI scan were suggestive of Brodie's abscess. But surgical exploration and subsequent histopathology showed evidence of osteoid osteoma. The patient had full resolution of symptoms after 3 months of surgery.
DISCUSSION
Osteoid osteoma of the wrist bones is rare. They usually present with atypical pain. The diagnosis of osteoid osteoma is challenging and often missed. A high index of suspicion and appropriate investigations are essential in the diagnosis.
CONCLUSION
We conclude that the diagnosis of osteoid osteoma should be considered in case of wrist pain of unknown aetiology with cystic lesions in the carpal or metacarpal bones.
Keywords: Wrist pain, Brodie's abscess, Osteoid osteoma
1. Introduction
Osteoid osteoma is a benign tumour of the skeleton which affects the femur and tibia predominantly and less commonly the bones of the hand.1 It is reported that the metacarpals are the least common site for this tumour.3 Osteoid osteoma usually affects children and young adults and account for 10% of all benign bone tumours.4 The patients most often complaints of pain which is nocturnal, intermittent and typically relieved by taking aspirin.5 The clinical diagnosis of osteoid osteoma in metacarpals is often missed or delayed. This is due to the fact that the clinical, radiological and histological features of osteoid osteoma in metacarpal bones may differ from that in long bones.6 The infrequent occurrence in the hand also contributes to the missed and delay in the diagnosis.7 We report a case of unusual and rare case of osteoid osteoma of the metacarpal which presented with wrist pain and radiologically diagnosed as Brodie's abscess.
2. Case report
A 35 year old right hand dominant Caucasian male was referred to our outpatient clinic with history of pain and a lump in this right wrist. He had previously undergone an operation for a possible (ganglion) at another hospital 3 years ago for the same symptoms. His symptoms had not changed in spite of surgery. The pain was mainly on the radial side of the wrist with exacerbations when he gripped things hard. He occasionally had sharp shooting pain in the index and middle finger. He had no night pain.
On examination there was a healed scar on the dorsum of the right hand in line with the second metacarpal. No lumps were palpable. There was tenderness and prominence of the base of the second metacarpal. No instability of the carpo-metacarpal joints or intercarpal joints was demonstrated.
The radiograph of the right hand revealed a slightly expanded base of the second metacarpal with a cyst formation (Fig. 1). An MRI scan was arranged to rule out the possibility of any occult ganglions or an injury to the scapholunate ligament (due to previous surgery). The scan reported an abnormal second metacarpal base with profound oedema and focal area of bone irregularity and a sclerotic margin. A provisional diagnosis of a Brodie's abscess was suggested by the radiologist (Fig. 2). The inflammatory markers showed normal white cell count and CRP of 13.
Fig. 1.

The radiograph of the hand showing a well circumscribed cystic lesion in the base of second metacarpal.
Fig. 2.

MRI picture of the hand showing cystic lesion with well-defined margins suggestive of Brodie's abscess.
The patient was offered surgery for exploration, curettage and debridement of base of second metacarpal. The second metacarpal base was exposed through the old scar. The findings were thickened capsule with synovitis of the second carpo-metacarpal joint. There was a cyst within the base of the second metacarpal with a soft tissue lining. The cyst was curetted and the specimen was sent for histopathology and culture and sensitivity. There were no post-operative complications.
The histopathology showed osteoid lined by plumb osteoblasts with highly vascularised connective tissue. There was no evidence of inflammation. It also showed exuberant new osteoid and bone formation, cellular and well vascularised stroma surrounded by a thickened layer of dense mature bone. The appearances were suggestive of a benign osteoid osteoma (Fig. 3). The culture did not grow any organism.
Fig. 3.
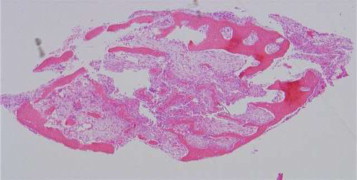
Histopathology slide showing seams of osteoid and new bone formation lined by osteoblasts suggestive of osteoid osteoma.
The patient was followed up in the clinic 2 weeks after the surgery. The wound had healed satisfactorily. There was complete resolution of the pre-operative pain. The patient was reviewed again in the clinic after 3 months. By then patient had made a full clinical and functional recovery. The radiograph showed that the cyst had healed completely (Fig. 4). He was discharged from the clinic. Quick DASH (Disabilities of the Arm, Shoulder and Hand) score was 23.9 at 3 months.
Fig. 4.

The radiograph at 3 months follow-up showing the lesion well healed.
3. Discussion
The causes of wrist pain are many. The commonest causes include ganglia, osteoarthritis and post-traumatic conditions like Scapho Lunate Advanced Collapse (SLAC) and Scaphoid Non-union Advanced Collapse (SNAC). Infection has to be suspected in all patients who have had prior surgery (as in our case).
Osteoid osteoma is a benign tumour of the growing skeleton and usually affects young adults in the second and third decades. There is a male predominance with a male to female ratio of 2:1. It is not common among African and American population. It has got a tendency to affect the lower limb bones especially towards the ends of femur and tibial shafts. Approximately 10% are equally distributed between spine, hand and foot.8
The commonest site for osteoid osteoma in hand is the phalanges followed by the carpal bones. The metacarpals are the least common site for osteoid osteoma.9 The largest series of hand osteoid osteoma was described by Ambrosia et al.10 They reported 19 cases of osteoid osteomas in which included two in capitate, one in hamate and one in the triquetrum. It rarely grows more than 1 cm in diameter.11 Basu et al. described a painless osteoid osteoma in the metacarpal with a size above 1 cm and the radiological picture suggested an infection.12
The patients usually present with pain and swelling. Pain is present in about 80% of cases and is typically relieved by salicylates and other non-steroidal anti-inflammatory agents which inhibits the production of prostaglandins.13 There are various theories postulated to explain the cause and intensity of pain associated with osteoid osteoma. The prostaglandins produced by the tumour directly stimulate the nerve endings by lowering the threshold of pain receptors.14 The nerve endings may be stimulated by the pressure of increased blood flow to the region as a result of inflammation or neo-growth.15 These nerve fibres which are mostly incorporated in the fibrous tissue surrounding the nidus of the osteoid osteoma belong to the autonomic nervous system also contribute to the origin of pain.16
The radiographic features of osteoid osteoma are characteristic and diagnostic. Conventional radiographs reveal a well-demarcated lytic lesion (nidus) surrounded by a distinct zone of sclerosis. But in metacarpals the diagnosis is difficult. As in our case, the nidus may not be visible, so additional imaging techniques, such as computed tomography, radioisotope scanning, and magnetic resonance imaging, may be necessary to document the lesions.16 MRI is useful not only for illustrating the lesion but also for demonstrating the existence of local inflammation and bone oedema, especially on T2-weighted or Gd-enhanced images. This could be seen in our patients scan, but in view of the history of previous surgery the possibility of a Brodie's abscess was raised.
The differential diagnosis for osteoid osteoma are acute and chronic osteomyelitis, Brodie's abscess, intracortical hemangioma, bone island, stress fracture, tuberculous and syphilitic lesions, and osteoblastoma, Ewing's sarcoma and intracortical osteosarcoma.1,2
The medical management of these patients is with prolonged treatment with no steroidal anti-inflammatory drugs.17 In our patient, symptoms had persisted for more than 3 years in spite of adequate analgesia. Complete surgical excision of the nidus, even if it is intralesional, is the treatment of choice for patients with osteoid osteoma in whom conservative management fails. It provides immediate relief and is usually curative.18 The dramatic resolution of pain in our patient confirms the rapid recovery following such surgery. Other less invasive methods of treatment have been described such as ablation of the nidus with a percutaneously placed radiofrequency, radionuclide-guided excision,19,20 CT-guided percutaneous excision,21 percutaneous laser photocoagulation22 and computer assisted surgery.23 Surgery is also preferred if diagnosis is in doubt.
4. Conclusion
The diagnosis of wrist pain can be challenging especially if faced with unusual diagnosis such as our patient. History of prior surgery to the wrist should always raise the possibility of infection or iatrogenic injury to the intercarpal ligaments. A thorough examination and radiological investigation should be performed in all cases. In spite of appropriate investigations, the diagnosis might still be challenging as in our case, due to rarity of this condition and the history of previous surgery.
We would like to emphasise the importance of ruling out a neoplastic cause of unexplained wrist pain and also to keep the diagnosis of osteoid osteoma in mind, in the presence of lytic lesions in the metacarpal. Histopathological examination is strongly recommended. Excellent functional recovery is to be expected after surgical excision.
Conflict of interest
There is no competing interest in relation to this article.
Funding
No financial or funding has been received from anybody or organisation.
Ethical approval
Ethical approval has been got from the hospital trust and informed consent has been obtained.
Author contributions
Aysha Rajeev has contributed to study concept, design data collection, data analysis and writing of the paper. Mohammed Ali prepared the case report. Angela Ralte prepared the histology slide and its description. Jaganath Chakravarthy contributed towards the management and follow up of the patient.
References
- 1.Carroll R.E. Osteoid osteoma in the hand. J Bone Joint Surg Am. 1953;35A:888–893. [PubMed] [Google Scholar]
- 2.Morton K.S., Quenville N.V., Beauchamp C.P. Aggressive osteoblastoma. A case previously reported as a recurrent osteoid osteoma. J Bone Joint Surg (Br) 1989;71(3):428–431. doi: 10.1302/0301-620X.71B3.2722934. [DOI] [PubMed] [Google Scholar]
- 3.Chronopoulos E., Xypnitos F.N., Nikolaou V.S., Efstathopoulos N., Korres D. Osteoid osteoma of a metacarpal bone: a case report and review of the literature. J Med Case Rep. 2008;2:285. doi: 10.1186/1752-1947-2-285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Resnick D., Niwayama G. Saunders; Philadelphia, PA: 1988. Tumours and tumour like diseases in diagnosis of bone and joint disorders; pp. 3621–3635. [Google Scholar]
- 5.Greenspan A. Benign bone-forming lesions: osteoma osteoid osteoma, and osteoblastoma. Clinical, imaging, pathologic, and differential considerations. Skeletal. 1993;22(7):485–500. doi: 10.1007/BF00209095. [DOI] [PubMed] [Google Scholar]
- 6.Burger I.M., McCarthy E.F. Phalangeal osteoid osteomas in the hand: a diagnostic problem. Clin Orthop Relat Res. 2004;427:198–203. doi: 10.1097/01.blo.0000142623.97901.39. [DOI] [PubMed] [Google Scholar]
- 7.Doyle L.K., Ruby L.K., Nalebuff B.G., Belsky M.R. Osteoid osteoma of the hand. J Hand Surg. 1985;10A:408–410. doi: 10.1016/s0363-5023(85)80045-9. [DOI] [PubMed] [Google Scholar]
- 8.Kransdorf M.J., Stuli M.A., Gilkey F.W., Moser R.P., Jr. Osteoid osteoma. Radiographics. 1991;11:671–696. doi: 10.1148/radiographics.11.4.1887121. [DOI] [PubMed] [Google Scholar]
- 9.Uda H., Mizuzeki T., Tsuge K. Osteoid osteoma of the metacarpal bone presenting after an injury. Scand J Plast Reconstr Surg Hand Surg. 2002;36:238–242. doi: 10.1080/02844310260259932. [DOI] [PubMed] [Google Scholar]
- 10.Ambrosia J.M., Wold L.E., Amadio P.C. Osteoid osteoma of hand and wrist. J Hand Surg. 1987;12A:794–800. doi: 10.1016/s0363-5023(87)80072-2. [DOI] [PubMed] [Google Scholar]
- 11.Dick H.M. Bone tumours. In: Green D.P., editor. Operative hand surgery. Churchill Livingstone; New York: 1982. p. 1684. [Google Scholar]
- 12.Basu S., Basu P., Dowell J.K. Painless osteoid osteoma in a metacarpal. J Hand Surg. 1999;24B:133–134. doi: 10.1054/jhsb.1998.0048. [DOI] [PubMed] [Google Scholar]
- 13.Healey J.H., Ghelman B. Osteoid osteoma and osteoblastoma. Current concepts and recent advances. Clin Orthop Relat Res. 1986;204:76–85. [PubMed] [Google Scholar]
- 14.Greco F., Tamburrelli F., Ciabattoni G. Prostaglandins in osteoid osteoma. Int Orthop. 1991;15:35–37. doi: 10.1007/BF00210531. [DOI] [PubMed] [Google Scholar]
- 15.Golding J.S. The natural history of osteoid osteoma; with a report of twenty cases. J Bone Joint Surg Br. 1954;36B(2):218–229. doi: 10.1302/0301-620X.36B2.218. [DOI] [PubMed] [Google Scholar]
- 16.Sherman M.S., McFarland G., Jr. Mechanism of pain in osteoid osteomas. South Med J. 1965;58:163–166. doi: 10.1097/00007611-196502000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Barei D.P., Moreau G., Scarborough M.T., Neel M.D. Percutaneous radiofrequency thermal ablation of osteoid osteoma. Oper Tech Orthop. 1999;9(2):72–78. doi: 10.1097/00003086-200004000-00014. [DOI] [PubMed] [Google Scholar]
- 18.Pettine K.A., Klassen R.A. Osteoid-osteoma and osteoblastoma of the spine. J Bone Joint Surg Am. 1986;68(March (3)):354–361. [PubMed] [Google Scholar]
- 19.Cioni R., Armillotta N., Bargellini I., Zampa V., Cappelli C., Vagli P. CT-guided radiofrequency ablation of osteoid osteoma: long-term results. Eur Radiol. 2004;14(July (7)):1203–1208. doi: 10.1007/s00330-004-2276-6. [DOI] [PubMed] [Google Scholar]
- 20.Wioland M., Sergent-Alaoui A. Didactic review of 175 radionuclide-guided excisions of osteoid osteomas. Eur J Nucl Med. 1996;23(August (8)):1003–1011. doi: 10.1007/BF01084380. [DOI] [PubMed] [Google Scholar]
- 21.Sans N., Galy-Fourcade D., Assoun J., Jarlaud T., Chiavassa H., Bonnevialle P. Osteoid osteoma: CT-guided percutaneous resection and follow-up in 38 patients. Radiology. 1999;212(September (3)):687–692. doi: 10.1148/radiology.212.3.r99se06687. [DOI] [PubMed] [Google Scholar]
- 22.Witt J.D., Hall-Craggs M.A., Ripley P., Cobb J.P., Bown S.G. Interstitial laser photocoagulation for the treatment of osteoid osteoma. J Bone Joint Surg Br. 2000;82(November (8)):1125–1128. doi: 10.1302/0301-620x.82b8.11307. [DOI] [PubMed] [Google Scholar]
- 23.Donahue F., Ahmad A., Mnaymneh W., Pevsner N.H. Osteoid osteoma, computed tomography guided percutaneous excision. Clin Orthop Relat Res. 1999;366:191–196. [PubMed] [Google Scholar]