

Highlights
-
•
Fracture dislocations of radiocarpal joint are rare injuries.
-
•
Consider dorsal displacement of median nerve and flexor tendons, to dorsal compartent, following dorsal radiocarpal fracture-dislocation.
-
•
Surgically reduction is required.
Keywords: Distal radius, Fracture, Dislocation, Median nerve, Flexor tendons
Abstract
INTRODUCTION
High energy distal radius fractures may cause significant soft tissue injuries. Dorsal displacement of median nerve and flexor tendons to dorsal compartment between distal radioulnar joint was an unreported type of soft tissue injury.
PRESENTATION OF CASE
35-Year male admitted following fall from height diagnosed as closed distal radius fracture with dorsal displacement. The patient had no flexion and extension of all fingers with loss of sensation. Radial artery pulse was not palpable. Radiography and CT imaging revealed distal radius fracture with dorsal displacement with dorsal carpal dislocation. After failure of closed reduction, operative treatment was performed. At surgery, flexor tendons and median nerve was found to be placed at dorsal compartment. Reduction of the soft tissues was facilitated by distraction of distal radioulnar joint.
DISCUSSION
Dorsal displacement of volar structures as the result of fracture dislocation was found to be an unreported type of injury. Difficulty during reduction of dorsally displaced structures is an important feature of the case.
CONCLUSION
For severely displaced and deformed distal radial fractures and fracture dislocations, threshold for operative treatment should be kept low.
1. Background
Fractures of distal radius with severe dorsal displacement occur due to high-energy trauma. Soft tissue interposition is one of the obstacles of reduction. Dorsal displacement of median nerve and flexor tendons to dorsal compartment, following dorsal radiocarpal fracture-dislocation is an unreported type of injury. We present such a case and challenges encountered during treatment.
2. Case
35-Year-old male patient admitted to emergency department after a fall from approximately 5 m of height on his right upper extremity. Physical examination revealed dinner fork deformity with loss of flexion and extension of all fingers with loss of sensation of 1st, 2nd and 3rd fingers. Radial artery pulse was not palpable. X-rays showed distal radius fracture with dorsal dissociation of carpal bones from the distal ulna (Fig. 1). Closed reduction under sedation was attempted. After failure of reduction computerized tomography imaging was performed. CT revealed fracture of radial styloid and multiple fragmented distal radial fracture with dorsal and proximal displacement of carpus. Distal radioulnar joint was stable (Fig. 2). Due to failure of reduction operative treatment was performed.
Fig. 1.

X-rays showing fracture-dislocation of distal radius, lateral (a) and AP (b) view.
Fig. 2.

Axial (a and b) and sagittal (c and d) CT images showing dorsally and proximally displaced radiocarpal fracture dislocation.
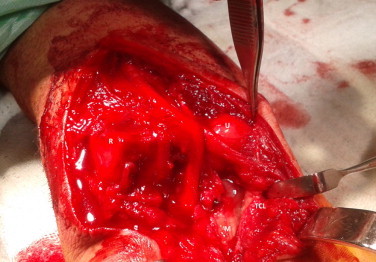
Surgery
Volar approach was performed. After superficial dissection, radial artery (RA), tendon of flexor carpi radialis (FCR) and palmaris longus (PL) were seen coursing over distal radius directly (Fig. 3). Avulsions of pronator quadratus (PQ) from radius and triradiate fibrocartilaginous complex (TFCC) from distal ulna, as well as avulsion of volar capsule of distal radioulnar joint were also encountered. After incision of transverse carpal ligament, median nerve (MN), and tendons of flexor digitorum profundus (FDP), flexor digitorum superficialis (FDS) and flexor pollicis profundus (FPL) were found to be located behind the radius and ulna on the dorsal compartment (Fig. 4). It was concluded that these structures (MN, FDS, FDP, FPL) passed between distal ulna and radius, as the result of dorsal directed shear force. Reduction of displaced soft tissue structures could be achieved by two 2.2 mm. K-wires placed longitudinally to distal radius and ulna (Fig. 5). After reduction integrity of tendons was checked. Contusion of median nerve was noted and neurolysis was performed (Fig. 6). After reduction of the fracture, fixation was achieved by Penning external fixator and a KW inserted to radial styloid (Fig. 7). TFCC was reattached to ulnar styloid with transosseous sutures. Ulnar artery and nerve with tendon of FCU were intact. Skin closure could be facilitated by split thickness grafting due to excessive swelling of soft tissues.
Fig. 3.

Volar approach: radial artery (a), tendons of FCR (b) and PL (c), distal radius (d), distal ulna (e), and avulsed pronator quadratus (f).
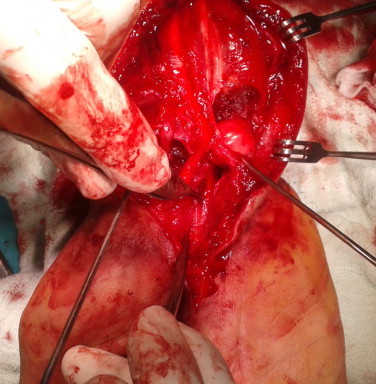
Fig. 4.
After release of transverse carpal ligament (TCL), median nerve (M) was found to be located behind radius (R) and ulna (U) with tendons of FDS, FDP and FPL.
Fig. 5.
Two K-wires were inserted to radius and ulna to distract radioulnar joint, to facilitate reduction of soft tissues.
Fig. 6.
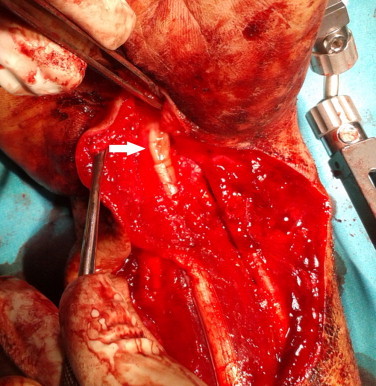
Median nerve (arrow) after relocation of dorsally displaced structures.
Fig. 7.

Post-operative AP (a) and lateral and (b) X-rays.
2.1. Aftertreatment
Active finger motion was encouraged after first postoperative day. Skin healed uneventfully. Fixator and K-wire were removed at post operative 6th week with rehabilitation with active motion. On the follow up, median nerve dysfunction persisted for 6 months with obvious thenar athrophy. Patient returned to work 6 months postoperatively. At first year follow-up visit, he had a range-of-motion of: 30–45° flexion, 0–10° extension, 45° pronation, 45° supination. Patient rated wrist score (PRWE) was 15 points for pain and 35 points for function, eventually total 50/100 which can be interpreted as “moderate result”. Hypoesthesia of 1st, 2nd, and 3rd fingers resolved but mild thenar athrophy persisted at first year follow up. Radiography revealed minimal dorsal subluxation of radiocarpal joint and a minimal ulnar translation (Fig. 8).
Fig. 8.

First year follow up, with minimal dorsal and ulnar translation.
3. Discussion
Radiocarpal dislocations tend to occur as a result of shear and rotational forces on wrist.1 They are usually fracture dislocations involving variable amounts of radial and ulnar styloid. A classification was introduced by Dumontier et al.2 According to this classification, this injury can be accepted as a type 2 injury with radial fracture involving more than 1/2 of scafoid fossa. It was also reported that type 2 cases tend to result with better outcome. Radial styloid repair with volar extrinsic ligamentous repair was reported to be correlated with better outcome.3,4
Soft tissue interposition is a relatively frequent cause of irreducible fractures and dislocations in upper extremity. Irreducible distal radius fractures due to tendon and epiphyseal plate interposition were reported in children previously.5,6 But failure of reduction due to soft tissue interposition is a very rare entity in adults. Dorsal displacement of soft tissues during injury was an unreported type of injury. Important feature of this case was not the entity itself, but the difficulty encountered during reduction of dorsally displaced structures. Forceful trial of closed reduction may have detrimental effect on soft tissues, especially on median nerve. For severely displaced and deformed distal radial fractures and fracture dislocations, threshold for operative treatment should be kept low.
Although Dumontier et al. recommended dorsal approach for reduction and repair of fractured styloid, reduction of the fragments and repair of soft tissue can be achieved safely through volar approach.
Conflict of interest
None declared.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author's contribution
Murat Songur collected the data; Ercan Şahin wrote the paper; Sinan Zehir organized the study design; Mahmut Kalem investigated the literature.
References
- 1.Ilyas A.M., Mudgal C.S. Radiocarpal fracture-dislocations. J Am Acad Orthop Surg. 2008;16(November (11)):647–655. doi: 10.5435/00124635-200811000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Dumontier C., Meyer zu Reckendorf G., Sautet A., Lenoble E., Saffar P., Allieu Y. Radiocarpal dislocations: classification and proposal for treatment. A review of twenty-seven cases. J Bone Joint Surg Am. 2001;83-A(February (2)):212–218. doi: 10.2106/00004623-200102000-00008. [DOI] [PubMed] [Google Scholar]
- 3.Mudgal C.S., Psenica J., Jupiter J.B. Radiocarpal fracture-dislocation. J Hand Surg Br. 1999;24(February (1)):92–98. doi: 10.1016/s0266-7681(99)90047-5. [DOI] [PubMed] [Google Scholar]
- 4.Brown D., Mulligan M.T., Uhl R.L. Volar ligament repair for radiocarpal fracture dislocation. Orthopedics. 2013;36(June (6)):463–468. doi: 10.3928/01477447-20130523-07. [DOI] [PubMed] [Google Scholar]
- 5.Mohanlal P., Jain S. Irreducible distal radial fracture due to extensor pollicis longus tendon interposition: a case report. Cases J. 2009;3(June (2)):6822. doi: 10.1186/1757-1626-2-6822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lesko P.D., Georgis T., Slabaugh P. Irreducible Salter-Harris type II fracture of the distal radial epiphysis. J Pediatr Orthop. 1987;7:719–721. [PubMed] [Google Scholar]