

Abstract
INTRODUCTION
Although diverticular disease of the colon is frequent, perforated diverticulitis causing subcutaneous emphysema is a uncommon entity. We wish to present this extremely rare case of perforated colonic diverticulum in the subcutaneous tissue, which is the first one that we have encountered in our practice, along with the accompanying diagnostic and therapeutic issues and a review of the literature.
PRESENTATION OF CASE
We report the case of an 83-year-old man who admitted to the emergency room due to an abdominal subcutaneous emphysema. Physical examination revealed a severe subcutaneous emphysema especially in the left iliac fossa and abdominal pain. An urgent contrast enhanced abdominal CT scan showed multiple diverticula in the sigmoid colon and multiple air bubbles in the subcutaneous tissue. The exploratory laparotomy identified a perforation of diverticular in subcutaneous tissue. Forty centimeters of colon were resected. The subcutaneous emphysema resolved without specific treatment. The postoperative period was uncomplicated.
DISCUSSION
Subcutaneous emphysema of anterior abdomen wall is an obvious physical sign but its etiology is complex to determine and may be potentially lethal. The pathophysiological mechanism involved is the emergence of a pressure gradient between the peritoneum and surrounding structures, causing rupture of the anterior abdominal wall, allowing gas from a perforation to diffuse along tissue planes.
CONCLUSION
This physical sign may be of especial value in elderly patient groups amongst whom perforation may be less clinically obvious. General surgeons should bear in mind this rare complication of colonic diverticulosis.
Keywords: Subcutaneous emphysema, Acute abdomen, Colonic diverticulosis, Perforation, Surgery
1. Introduction
Although diverticular disease of the colon is frequent, perforated diverticulitis causing subcutaneous emphysema is an uncommon entity. Colonic diverticulosis is characterized by herniation of mucosa and submucosa through the muscular layer of the colon wall. Subcutaneous emphysema is an obvious physical sign but its etiology is complex to determine.1 The perforation of the colonic diverticulum can be fatal. We wish to present this extremely rare case of perforated colonic diverticulum in the subcutaneous tissue, which is the first one that we have encountered in our practice, along with the accompanying diagnostic and therapeutic issues and a review of the literature.
2. Presentation of case
We report the case of an 83-year-old man who admitted to the emergency room due to an abdominal subcutaneous emphysema. Her medical history included appendectomy, cholecystectomy, chronic pancreatitis, silicosis and Alzheimer's disease. He had abdominal pain, fatigue and fever. Physical examination revealed a severe subcutaneous emphysema especially in the left iliac fossa and abdominal pain. We noted a persistent inflammatory syndrome with hyperleukocytosis. An urgent contrast enhanced abdominal CT scan showed multiple diverticula in the sigmoid colon and multiple air bubbles in the subcutaneous tissue especially in the left iliac fossa (Figs. 1 and 2).
Figs. 1 and 2.
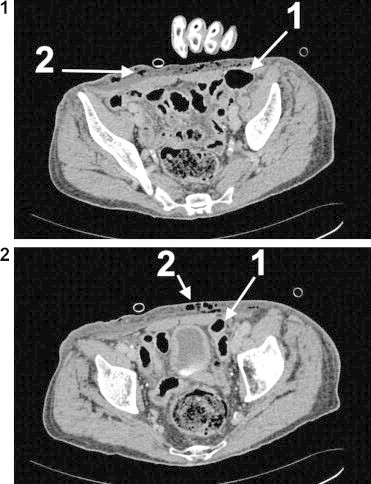
Abdominal CT scan revealed a multiple diverticula of the sigmoid colon. Findings are suggestive of perforated diverticulitis (1) causing subcutaneous emphysema and free gas in the tissue of the anterior abdominal wall (2).
The sigmoid colon was perforated causing subcutaneous emphysema and an emergent laparotomy was performed. A midline incision was made. The exploratory laparotomy revealed the presence of multiple diverticula of the sigmoid colon and identified a multiple perforation in subcutaneous tissue. We did not perform a peroperative pathological study. Forty centimeters of colon were resected, followed by peritoneal lavage with saline solution and drainage. The perforation of the anterior abdominal wall was closed with an absorbable suture and a colostomy was performed. A colostomy was performed. In postoperative period, the patient remained asymptomatic with an antibiotic (Augmentin). The subcutaneous emphysema resolved without specific treatment. The postoperative period was uncomplicated. The patient tolerated the procedure and discharged on the 9th postoperative day. Histopathology report confirmed a multiple diverticula of the sigmoid colon. He was asymptomatic after 5 month of follow-up (no damage or hernia occurred).
3. Discussion
Colonic diverticulosis is a common disease of the aging population of the Western world. The prevalence of diverticular disease ranges from 65% of those aged 85 years, 30% of those aged 60 years and in less than 5% in those aged 40 year.2
The subcutaneous emphysema is a rare but recognized manifestation of intra-abdominal pathology. Henry D.I. De’Ath et al. described the case of a case of a sigmoid perforation presenting as a pneumoscrotum with progressive surgical emphysema. There are many causes of gas in the subcutaneous tissues: trauma, iatrogenic (high and low endoscopy),3,4 infectious (necrotizing fasciitis, Fournier gangrene, etc.), fecaloma.5,6 One should consider the respiratory tract (pneumothorax, bronchial fistula chest radiograph should be performed to look for a pneumothorax.7
The etiopathogenesis of colonic diverticulosis is unclear, although the current hypothesis focuses (predisposing factor) on abnormalities in the smooth muscle and on high intraluminal pressures. There are three types of microscopic abnormalities: 1/visceral neuropathy = axonal and neuronal degeneration. 2/visceral myopathy = fibrosis and degenerated smooth muscle cells. 3/progressive systemic sclerosis = fibrosis and decreased numbers of normal muscle cells. The causes of diverticular perforation are: an acute necrotizing inflammatory (82%), a foreign body (6%) or blunt trauma to the abdominal wall (12%). In our case, the mechanism responsible for diverticular perforation is difficult to identify.
We have reported our experience in the management of a patient with perforated diverticulitis, whose main physical sign was subcutaneous emphysema of abdomen. Subcutaneous emphysema is an obvious physical sign but its etiology is complex to determine and may be potentially lethal.1 In our case, the pathophysiological mechanism involved is the emergence of a pressure gradient between the peritoneum and surrounding structures, causing rupture of the anterior abdominal wall with subsequent dissection of the abdominal muscles sheath and infiltration of the pneumoperitoneum in subcutaneous tissue. This rupture of the anterior abdominal wall allows gas from a perforation to diffuse along tissue planes.8
Diagnosis is often delayed because clinical symptoms are not specific and the diagnosis is performed mainly by imaging studies. In our case, the patient had abdominal pain, fatigue and fever. A delayed diagnosis can be fatal, because perforation is associated with a high mortality. Abdominal CT is the diagnostic tool of choice even if it's not possible to identify all colonic diverticula. Computed tomography is useful to suggest this diagnosis, to estimate the extend of the inflammatory reaction, and to exclude other causes of acute abdominal pain. Martí de Gracia et al. concluded that “radiologists must be aware of abnormal gas in soft tissue because it may be the main or unique sign leading to an underlying pathology, which can be lethal”.9 In our case, abdominal CT scan showed multiple diverticula in the sigmoid colon and multiple air bubbles in the subcutaneous tissue especially in the left iliac fossa. The risk of infection associated with the dissemination of subcutaneous emphysema is poorly documented and justifies a monitoring of this physical sign.
4. Conclusion
Although the incidence of perforated colonic diverticulum in the subcutaneous tissue is extremely low, surgeons should be aware of the existence of this kind of atypical presentation of colonic diverticulitis.
Conflict of interest
No conflict of interests.
Funding
No source of funding.
Ethical approval
Informed consent was obtained from the patient in writing for the publication of this case report and the accompanying images.
Author contribution
Radwan Kassir: writing.
Karine Abboud and Joelle Dubois: conceptualized and designed the paper.
Tarek Debs, Imed Ben Amor, Jean Gugenheim Jean-Pierre Favre and Pauline Gastaldi: reviewed the paper.
Olivier Tiffet: reviewed and revised the paper.
Key learning points.
-
•
General surgeons should bear in mind this extremely rare presentation of colonic diverticulitis.
-
•
Subcutaneous emphysema is an obvious physical sign but its etiology is complex to determine.
-
•
The risk of infection associated with the dissemination of subcutaneous emphysema is poorly documented and justifies a monitoring of this physical sign.
-
•
The unusual presentation of the subcutaneous emphysema prompted us to do a diagnostic laparoscopy first.
-
•
A delayed diagnosis can be fatal, because perforation is associated with a high mortality in up to 40% of patients.
References
- 1.Souche R., Bouyabrine H., Navarro F. Subcutaneous emphysema of thorax, neck and face after elective left colectomy: a case report. Int J Surg Case Rep. 2013;4(5):489–492. doi: 10.1016/j.ijscr.2013.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sivarajah V., Jones C., Pittathankal A. Radiological evidence of subcutaneous emphysema leading to a diagnosis of retroperitoneal perforated diverticulum. Int J Surg Case Rep. 2013;4(6):531–533. doi: 10.1016/j.ijscr.2013.01.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cappello M., Randazzo C., Peralta S., Cocorullo G. Subcutaneous emphysema, pneumomediastinum and pneumoperitoneum after diagnostic colonoscopy for ulcerative colitis: a rare but possible complication in patient with multiple risk factors. Int J Colorectal Dis. 2011;26(3):393–394. doi: 10.1007/s00384-010-1005-7. [DOI] [PubMed] [Google Scholar]
- 4.Marwan K., Farmer K.C., Varley C., Chapple K.S. Pneumothorax, pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema following diagnostic colonoscopy. Ann R Coll Surg Engl. 2007;89(5):W20–W21. doi: 10.1308/147870807X188506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brunet C., Thomas P., Sielezneff I., Ugarte S., Giudicelli R., Sastre B. Subcutaneous cervical emphysema: complication of constipation. Review of the literature. J Chir. 1995;132(4):198–200. [PubMed] [Google Scholar]
- 6.Arana-Arri E., Cortés H., Cabriada V., Lekerika N., García-Verdugo A., Shengelia-Shapiro L. Giant fecaloma causing perforation of the rectum presented as a subcutaneous emphysema, pneumoperitoneum and pneumomediastinum: a case report. Eur J Emerg Med. 2007;14(6):351–353. doi: 10.1097/MEJ.0b013e3282004952. [DOI] [PubMed] [Google Scholar]
- 7.De’Ath H.D. Perforation of a sigmoid diverticulum presenting with a pneumoscrotum and surgical emphysema. BMJ Case Rep. 2008 doi: 10.1136/bcr.08.2008.0834. 2008:bcr0820080834, Epub 2008 Nov 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Agaba E.A., Kandel A.R., Agaba P.O., Wong L.S. Subcutaneous emphysema, muscular necrosis, and necrotizing fasciitis: an unusual presentation of perforated sigmoid diverticulitis. South Med J. 2010;103(4):350–352. doi: 10.1097/SMJ.0b013e3181c1a899. [DOI] [PubMed] [Google Scholar]
- 9.de Gracia M., Gutiérrez F.G., Martínez M., Dueñas V.P. Subcutaneous emphysema: diagnostic clue in the emergency room. Emerg Radiol. 2009;16(September (5)):343–348. doi: 10.1007/s10140-009-0794-x. [DOI] [PubMed] [Google Scholar]