

Highlights
-
•
Esophageal leiomyoma is most common benign esophageal tumor.
-
•
Robot assisted surgery allows for resection of giant esophageal leiomyoma using minimally invasive approach.
Abbreviations: CT, computed tomography; Endo-GIA, endoscopic gastrointestinal automatic stapler
Keywords: Esophageal leiomyoma, Robot assisted thoracoscopic surgery, Minimally invasive surgery
Abstract
INTRODUCTION
Esophageal leiomyoma represents the most common benign esophageal tumor. Robot-assisted thoracoscopic surgery has provided ability to remove it successfully using a minimally invasive approach.
PRESENTATION OF CASE
A 63-year old female with history of chronic chest pain presented with an esophageal mass on chest CT and endoscopic ultrasound. Robot-assisted surgery was performed using three robot arms, a camera and an assistant port. A 10 cm leiomyoma was enucleated and removed through a 2 cm myotomy. Completion endoscopy confirmed integrity of the esophagus. Patient's chest pain resolved postoperatively, and she was discharged on postoperative day 3.
DISCUSSION
Our case describes successful removal of the giant esophageal leiomyoma (10 cm) by robot assisted minimally invasive resection through a 2 cm myotomy.
CONCLUSION
Use of robot allows for removal of large esophageal leiomyoma. The improved dexterity and patient outcome offered by robot suggests its potential as the mainstay technique for giant esophageal leiomyoma removal.
1. Introduction
Robot-assisted thoracoscopic surgery is a relatively new technique employed for treatment of esophageal lesions. We report a case of robot-assisted resection of an esophageal leiomyoma. We successfully removed a 10 cm esophageal leiomyoma through a 2 cm myotomy using the robot.
Esophageal leiomyoma represents 80% of all benign tumors of the esophagus. Most esophageal leiomyomas are located in the lower 2/3 of the esophagus. They typically do not become symptomatic until they grow to be greater than or equal to 5 cm.1 Consequently, they are most often discovered incidentally on radiologic examination of the thorax.2 Most common symptoms are epigastric pain, dysphagia, and odynophagia.3
Recently, robot-assisted thoracoscopic surgery using the da Vinci robotic system (Intuitive Surgical Inc., Sunnydale, CA) has provided improved visualization and dexterity in the surgical field for the surgeon using minimally invasive incisions. There are reports of removal of the esophageal leiomyoma using the robot technology1,4,5; however, none of the other cases describe an approach of removing a giant esophageal leiomyoma (10 cm) in the middle esophagus. Here, we describe a case where we removed a 10 cm mass using a 2 cm myotomy incision.
2. Presentation of case
The study was approved by the institutional review board at Houston Methodist Hospital. A 63 year old female presented with longstanding history of chest pain. A CT of the chest revealed a 4 cm esophageal lesion (Fig. 1A) which was confirmed as a submucosal mass on endoscopy and endoscopic ultrasound. Patient underwent surgical resection of the submucosal mass.
Fig. 1.
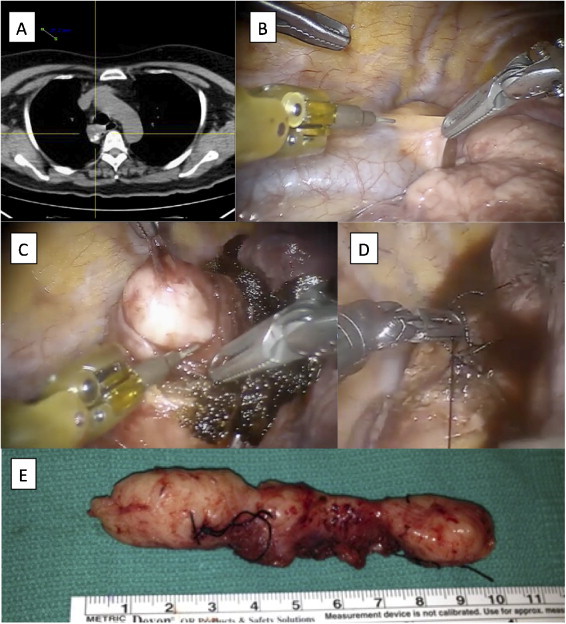
Esophageal leiomyoma. (A) Computed tomography scan of the chest shows a large calcified mass adjacent to the esophagus. (B) Intra-operative image demonstrating a bulge below the azygous vein. (C) A 2 cm esophageal myotomy was performed and the esophageal leiomyoma was enucleated. (D) The myotomy was closed with interrupted 3-0 silk sutures. (E) And a 10 cm esophageal leiomyoma was confirmed on final pathology.
The patient was placed in the left lateral decubitus position. Right lung was isolated and trocars were placed. An 8-mm robot trocar (Intuitive Surgical) was placed at the midaxillary line above the fifth rib. A camera was placed in this trocar while other ports were placed under direct visualization. Next, an 8-mm robot trocar (Intuitive Surgical) was placed 1 cm lateral to the spine over the eighth rib. A third 8 mm robot trocar (Intuitive Surgical) was placed 8 cm from the last trocar over the eighth rib. Next, a 12 mm Endopath Xcel camera port (Ethicon, New Brunswick, New Jersey) was placed 8 cm from the last trocar over the eighth rib near the posterior axillary line. Finally an assistant 12 mm Endopath Xcel trocar (Ethicon) was placed 8 cm inferior to the camera port above the diaphragm. The robot was then docked with robot arms connected to Thoracic Grasper (Intuitive Surgical) in the far left port to camera, Cadiere Robot Forceps (Intuitive Surgical) in the right port to the camera, and Permanent Cautery Spatula (Intuitive Surgical) in the left port to the camera.
Posterior mediastinal exposure revealed a bulge under the azygous vein (Fig. 1B). The azygous vein was mobilized using the cautery spatula and divided using an Endo-GIA stapler vascular load (Covidien, Mansfield, MA, USA). Careful dissection was undertaken along the line of the esophagus and subpleural fat overlying the esophagus. This brought the focal point to the esophageal bulge where we performed delicate dissection between the muscle fibers which were held with robot thoracic grasper and robot Cadiere forceps, allowing access to the glistening white surface of the esophageal leiomyoma. An approximately 2 cm incision was made on the esophageal muscle layer using the robot cautery spatula (Fig. 1C). A 3-0 silk was applied on the leiomyoma for retraction by placing the needle through the assistant port to Large Needle Driver (Intuitive Surgical) that was placed the robot port in the right side of the camera. Pulling the mass toward the right and left using the robot thoracic grasper while simultaneously performing a blunt dissection of muscle fibers using the robot cautery spatula allowed for the successful enucleation of 10 cm mass. The mass was removed in an Endo Catch bag. The myotomy was closed with 3-0 silk in interrupted fashion using the robot needle driver (Fig. 1D). Pathology confirmed the mass to be consistent with a 10 cm esophageal leiomyoma (Fig. 1E).
A completion endoscopy was performed (Fig. 2A) in which the mucosa was noted to be intact and the integrity was confirmed by filling the thoracic cavity with saline and insufflating the esophagus with air. There was no sign of perforation. A chest tube was placed and incisions were closed. After the resection, patient's chest pain resolved. Esophagram on postoperative day 1 demonstrated no signs of leak (Fig. 2B). Her diet was advanced, and the chest tube was removed on postoperative day 3 when she was discharged home.
Fig. 2.
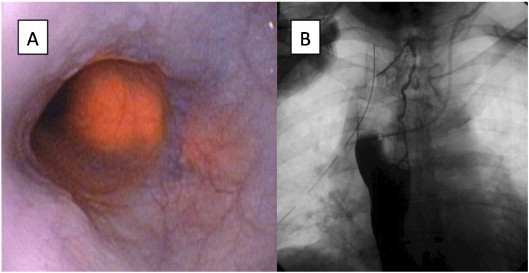
Post-resection evaluation. (A) Endoscopy shows no mucosal abnormality at the area of the leiomyoma resection. (B) Esophagram shows no esophageal leak.
3. Discussion
In our case presentation, we show that a giant 10 cm esophageal leiomyoma can be safely removed using a small myotomy incision with robotic assistance. Our case is novel in its clear demonstration of the robot-assisted enucleation of the largest reported esophageal leiomyoma at 10 cm in the middle esophagus. The next largest esophageal leiomyoma reported to be removed using a robot was 7 cm.5 This case illustrates the current trend in esophageal surgery going from open thoracotomy to minimally invasive routes. The minimally invasive surgery has shown significant advantages of decreased hospital length of stay and postoperative pain. Use of the robot provides advantages of three-dimensional vision, natural eye-hand coordination, motion scaling,1 and tremor filtration.5 The use of the robot has yielded significant reduction in mucosal injury from 1 to 15%, in both open thoracoscopy and laparotomy, to 0% in robotic-assisted thoracoscopic surgery for resection of esophageal leiomyoma.5 Furthermore, robot application in the mediastinum has a longstanding display of avoidance of surgical mortality and intraoperative blood loss.6 Finally, robot assisted resection offers decreased hospital stay and quicker postoperative return to normal activities than laparotomy.1 Although the cost of the robot is at times prohibitive to wide use, the benefits of this technology in certain procedures that require dissection in confined space tip the scale of making this a significant benefit for the patient compared to the cost of the procedure. In our case, for instance, the leiomyoma was densely adherent to the mucosa and the muscular layer where robot allowed safe dissection of the lesion, which would have been otherwise difficult to visualize even with a thoracoscopic approach.
4. Conclusion
We demonstrate that a giant 10 cm esophageal leiomyoma can be safely removed employing only a 2 cm myotomy incision with robotic assistance. This case, alongside the removal of a 7 cm esophageal leiomyoma noted in the literature,5 may support comfortable application of robot for large esophageal lesions. In summary, the benefits of increased precision, improved patient comfort, and complication reduction support robot-assisted thoracoscopic surgery as the mainstay mode of resecting esophageal leiomyomas.1
Conflict of interest
There is no direct conflict of interest with contents of this manuscript. However, MPK has received honoraria from Ethicon and Covidien for giving a talk at VATS lobectomy course and MPK has applied for patent for 4D lung cancer model.
Funding
Research supported by Thoracic Surgery Fund form Houston Methodist Foundation.
Consent
The study was approved by the institutional review board at Houston Methodist Hospital.
Author contribution
SC, PG and MPK were involved in study design, data collection, data analysis and writing of the manuscript.
Acknowledgement
Research supported by Thoracic Surgery Fund form Houston Methodist Foundation.
References
- 1.Khalaileh A., Savetsky I., Adileh M., Elazary R., Abu-Gazala M., Abu Gazala S. Robotic-assisted enucleation of a large lower esophageal leiomyoma and review of literature. Int J Med Robot. 2013;9:253–257. doi: 10.1002/rcs.1484. [DOI] [PubMed] [Google Scholar]
- 2.Lee L.S., Singhal S., Brinster C.J., Marshall B., Kochman M.L., Kaiser L.R. Current management of esophageal leiomyoma. J Am Coll Surg. 2004;198(1):136–146. doi: 10.1016/j.jamcollsurg.2003.08.015. [DOI] [PubMed] [Google Scholar]
- 3.Mutri C.J., Donahue D.M., Wain J.C., Wright C.D., Gaissert H.A., Grillo H.C. Esophageal leiomyoma: a 40-year experience. Ann Thorac Surg. 2005;79:1122–1125. doi: 10.1016/j.athoracsur.2004.08.029. [DOI] [PubMed] [Google Scholar]
- 4.Elli E., Espat N.J., Berger R., Jacobsen G., Knoblock L., Horgan S. Robotic-assisted thorascopic resection of esophageal leiomyoma. Surg Endosc. 2004;18:713–716. doi: 10.1007/s00464-003-8829-y. [DOI] [PubMed] [Google Scholar]
- 5.DeUgarte D.A., Teitelbaum D., Hirschl R.B., Geiger D. Robotic extirpation of complex esophageal leiomyoma. J Labaroendosc Adv Surg Tech. 2008;18:2. doi: 10.1089/lap.2007.0067. [DOI] [PubMed] [Google Scholar]
- 6.Augustin F., Schmid T., Bodner J. The robotic approach for mediastinal lesions. Int J Med Robot. 2006;2:262–270. doi: 10.1002/rcs.84. [DOI] [PubMed] [Google Scholar]