

Abstract
Background
Nearly 90% of the children with heart disease in low- and middle-income countries (LMICs) cannot access cardiovascular (CV) services. Limitations include inadequate financial, human, and infrastructure resources. Nongovernmental organizations (NGOs) have played crucial roles in providing clinical services and infrastructure supports to LMICs CV programs; however, these outreach efforts are dispersed, inadequate, and lack coordination.
Methods
A survey was sent to members of the World Society for Pediatric and Congenital Heart Society and PediHeart.
Results
A clearinghouse was created to provide information on NGO structures, geographic reach, and scope of services. The survey identified 80 NGOs supporting CV programs in 92 LMICs. The largest outreach efforts were in South and Central America (42%), followed by Africa (18%), Europe (17%), Asia (17%), and Asia-Western Pacific (6%). Most NGOs (51%) supported two to five outreach missions per year. The majority (87%) of NGOs provided education, diagnostics, and surgical or catheter-based interventions. Working jointly with LMIC partners, 59% of the NGOs performed operations in children and infants; 41% performed nonbypass neonatal operations. Approximately a quarter (26%) reported that partner sites do not perform interventions in between missions.
Conclusions
Disparity and inadequacy in pediatric CV services remain an important problem for LMICs. A global consensus and coordinated efforts are needed to guide strategies on the development of regional centers of excellence, a global outcome database, and a CV program registry. Future efforts should be held accountable for impacts such as growth in the number of independent LMIC programs as well as reduction in mortality and patient waiting lists.
Keywords: congenital heart disease, congenital heart surgery, international collaboration, nongovernmental organizations
Introduction
Children living in low- and middle-income countries (LMICs), defined by the World Bank based on gross national income per capita, continue to face tremendous challenges accessing care for the prevention, diagnosis, and treatment of heart diseases.1 Congenital heart disease (CHD) is a common birth defect and important cause of death, after infections, in the first year of life in LMICs.2,3 Rheumatic heart disease is an important acquired and preventable heart disease in LMICs. Rheumatic heart disease can lead to cardiac valve dysfunction and congestive heart failure. Rheumatic heart disease affects 15.6 million people worldwide with more than 98% of the cases occurring in LMICs.4,5 Overall, cardiovascular (CV) diseases in children, congenital or acquired, remain a significant contributor to premature noncommunicable disease-related deaths in LMICs.3
In 1999, Dr Felix Unger reported dramatic discrepancies in CV resources between developing countries and their North American or European counterparts.7 This issue of CV health disparity persists to the present time. Despite major advances in cardiac surgery and cardiology with a corresponding reduction in postsurgical mortality to less than 5%, most children with heart disease in LMICs are still unable to access CV services.8,9 For nearly two decades since the Unger report, humanitarian CV nongovernmental organizations (NGOs) have invested large amounts of resources transferring medical skills, modern equipment, and building CV programs in LMICs. These humanitarian efforts aimed at providing clinical services at the patient level as well as helping to establish independent CV programs in LMICs.8–13 Persistent road blocks against program sustainability and patient access to care included severely limited financial, human, and infrastructure resources.6,9,13 Some NGOs achieved success using models which involved rigorous selection of partner sites and providing long-term commitments to twinning partnership.10 However, these successful efforts are not a model universally utilized by NGOs. Furthermore, there have been few examples of collaboration among NGOs to identify a global strategy and reduce overlap in efforts. As the first step toward facilitating collaborations, we created an information clearinghouse of the NGOs’ organization structures, geographic reach, and their scope of services.
Materials and Methods
Survey Instrument
Survey questions were constructed by consensus among members of the World Society for Pediatric and Congenital Heart Surgery (WSPCHS) survey group, which includes congenital and adult cardiothoracic surgeons and pediatric cardiologists, most of whom have been directly involved in delivering pediatric CV services in LMICs. A 21-question online survey was sent to members of PediHeart and WSPCHS. PediHeart is a private, nonmoderated Internet discussion forum for health care professionals caring for children with heart disease. The estimated membership for PediHeart in 2009 was 1600. The World Society for Pediatric and Congenital Heart Surgery is a professional society of cardiothoracic surgeons and cardiologists with a mission to improve standards and access of CV care for children worldwide, with an emphasis on education and research and community service membership for WSPCHS in 2013 is 610. Survey respondents from PediHeart and WSPCHS were asked to identify and provide details about NGOs that are actively providing pediatric CV services in LMICs. The time period for collecting responses was from January 2013 to April 2013. When there were multiple responses for a specific NGO, data were combined to provide a more complete profile of the organization. When there were inconsistencies, we relied on responses from NGO administrators for definitive information. Direct follow-up with the NGOs was not performed.
Data Management
All data files were stored on a password-protected link to the Survey Monkey database (Survey Monkey, Palo Alto, California). The survey was structured to ensure anonymity of the respondents. At the close of the survey period (January 04, 2013), the data were exported to a Microsoft Excel Spread sheet (Microsoft Corp; Redmond, Washington) for review. Data storage and analysis were performed by Cardio Access, Inc (Fort Lauderdale, Florida).
Results
Respondents
There were 110 completed survey responses from members of WSPCHS and PediHeart. The majority (90 of 110) of the respondents were volunteers who participated in outreach cardiac missions. Administrative and nonmedical staff made up the remaining responses (20 of 110).
Nongovernmental Organization Characteristics
After accounting for duplicate or incomplete responses, 80 NGOs were identified. Although the majority (71%) of the NGOs had headquarters outside of the regions they serve, 29% of the NGOs represented local initiatives or in-country subsidiaries of multinational NGOs. Most of the NGO headquarters were in the America, followed by Europe and Asia-Western Pacific regions (Figure 1). The NGOs used various types of funding models, which included (1) full support from visiting teams (69.6%), from private foundations and individuals; (2) joint support from visiting teams and host programs (25.3%); or (3) full support from host programs (5.1%).
Figure 1.

Global distribution of headquarters of nongovernmental organizations providing pediatric cardiovascular care to low- and middle-income countries.
Nongovernmental Organization Geographic Reach and Scope of Services
The 80 NGOs identified in the survey provide pediatric CV services in 92 LMICs. Figure 2 depicts the distribution of NGO global outreach. By region, the largest percentage of NGO outreach efforts was in South and Central America (42%), followed by Africa (18%), Europe (17%), Asia (17%), and the Asia-Western Pacific region (6%; Figure 2). The majority (51%) of the NGOs supported two to five missions per year, whereas 20% supported one mission per year. Lack of growth or decline was a significant problem for nearly half (48.7%) of the NGOs. The primary reasons included lack of funding, limited equipment or medical volunteers, and inadequate infrastructure at partner sites in LMICs. Additionally, there were countries that sent requests but did not receive NGO supports due to restricted resources of NGOs. The countries most often identified were Haiti, Nigeria, Bangladesh, Cambodia, Costa Rica, and Nicaragua.
Figure 2.

Global distribution of NGO headquarters and geographic reach. Blue dots: NGO headquarters. Red dots: cardiac outreach partner sites. Red lines connect NGOs and outreach sites. A link to an interactive map is available at website: www.wspchs.org. NGO indicates nongovernmental organization.
Most of the NGOs (87%) provided comprehensive clinical and educational services during outreach missions. These activities fell into four categories including education, diagnostics, surgical interventions, and catheter-based interventions. Few NGOs (13%) provided only education and diagnostics outreach missions (Figure 3). Data were available for 77 NGOs regarding the types of interventions performed jointly by visiting NGOs and host teams during cardiac missions. Of the surgical interventions 59%, with or without cardiopulmonary bypass (CPB), were performed in infants and children. This was followed by non-CPB neonatal interventions (41%). Extensive interventions in children of all ages and lesion complexities were rarely performed (13%; Figure 4). The survey did not ask respondents to describe procedure complexity using the Risk Adjusted Classification for Congenital Heart Surgery 1, Aristotle scores, or the Society of Thoracic Surgeons/European Association for Cardio-Thoracic Surgery scoring system. Diagnostic and interventional catheter-based procedures were utilized by a significant number of NGOs (77%).
Figure 3.
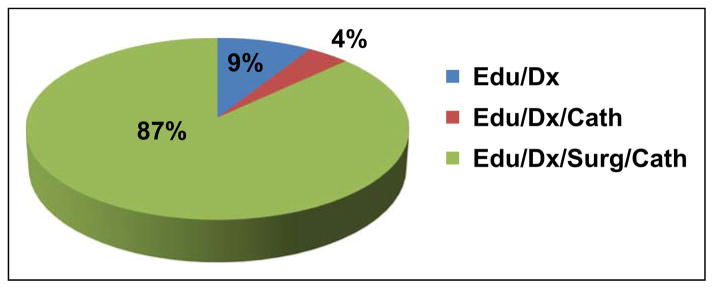
Types of clinical services provided by NGOs on cardiac missions. Edu indicates education; Dx, diagnostics; Cath, catheter-based interventions; Surg, surgical interventions; NGO, nongovernmental organization.
Figure 4.

Types of interventions performed jointly by visiting NGO and host teams. CPB indicates cardiopulmonary bypass; Inf, infant; Neo, neonates; NGO, nongovernmental organization.
Respondents also provided information on the limited scope of independent capabilities by LMICs partner programs. Nearly half (56%) reported that partner sites perform CPB cases in infants and children; 18% reported non-CPB cases on infants, children, and neonatal interventions limited to repairs of patent ductus arteriosus and coarctation of the aorta. A quarter (26%) of the NGOs reported that partner sites do not perform interventions in between outreach missions. Best practices followed by NGOs were as follows: outcome databases (80%), scouting mechanisms to identify prospective partner programs (60%), and participation in the International Quality Improvement Collaborative (24%).
Comment
This project was designed to create an information clearing-house of NGOs that are actively providing CV services to children living in LMICs. This represents an important first step in identifying opportunities for collaboration among the NGOs. Secondary goals were to describe the NGOs’ organizational characteristics, geographic reach, and scope of services. A link to the project summary and interactive map can be found on the WSPCHS Web site www.wspchs.org. Appendix A provides a list of the NGOs.
A Global Strategy is Needed to Improve NGO and Local CV Care Delivery in LMICs
Heart disease in LMICs is a rising public health issue with important economic impacts and significant contribution to mortality or morbidity.3,14 This survey demonstrates extensive CV NGOs outreach efforts; the majority of these missions are allocated to South and Central America, while Asia, Africa, and some parts of Europe remain undersupported. Many programs of the NGOs and LMICs utilize twinning partnerships, characterized by frequent on-location visits and gradual reduction in support of NGOs over time. This method has been shown to ensure establishment of independent and sustainable LMIC programs.10,15 This survey shows that NGOs send teams of volunteers and equipment cargos across great geographic distances to reach partner sites. These efforts require significant human and financial resources, and as a result, nearly half of the NGOs responding to this survey reported decline or no growth in their programs in the last five years. This is reflected in the number of outreach missions; 51% of the NGOs provide two to five missions per year while 20% of NGOs provide one mission per year. Meanwhile, ongoing requests for assistance remain unmet because of NGOs resource limitations. Local ability to perform independent interventions remains severely limited, as suggested by 26% of the NGOs reporting that their LMIC partners are not performing interventions in between missions. A global strategy is urgently needed, and the first step involves formalizing an LMICs CV community of practice. Key stakeholders will need to formulate rules of engagement, agree to work together on key issues of needs assessment, goal setting, and program development. The LMICs CV community of practice will guide and support the individual NGO and LMIC programs on how to achieve more with less through coordinating efforts and sharing resources to deliver sustainable and impactful CV care in LMICs. Organizations with global health emphasis such as the World Society for Pediatric and Congenital Heart Disease, World Heart Federation, and the World Health Organization (WHO) can play key leadership roles in providing frameworks and supports for the LMICs CV community of practice.
In addition to developing a global strategy, a major paradigm shift in the current modus operandi is necessary. Greater proportion of resources should be given to support regional centers of excellence (COEs) instead of city or country-based programs in collaboration and consistent with priorities mutually set by governments, professional associations, and the local health givers and teams. These regional hubs should be staffed with well-trained clinicians in the areas of cardiothoracic surgery, cardiology, anesthesia, and intensive care. These COEs should be supported with appropriate modern CV equipment and pharmaceuticals. In order for the COE to work effectively, they would need to be partnered with satellite city-based programs capable of providing diagnostic evaluations, preventive cardiology, and outpatient monitoring. With severe resource constraints and long-waiting lists, a strong network of COEs and intensive NGO–LMIC supports can reduce the distance and wait time for patients to receive CV services. Furthermore, NGO resources should be allocated to support infrastructures and team educational initiatives, in collaboration with professional organizations, both national and international.
Identification of in-country needs and capabilities will help NGOs and LMICs CV programs set priorities and plan program development to improve CV outcomes.
The WHO’s annual world health statistics reports provide limited information on health systems. There is a complete lack of data on LMIC cardiac capabilities, needs, and challenges. This survey shows that only 60% of the NGOs perform scouting missions and maintain internal information on partner LMIC programs. However, this information is spotty, incomplete, and is not shared. Creation of a CV registry of LMIC programs can provide information on country or region’s capabilities and needs; this in turn can inform decisions on future NGO efforts, policies and program development, as well as allocation of resources to provide targeted interventions. Currently, a CV LMICs outcome database does not exist. Of the NGOs who responded to this survey, 80% maintain internal outcome databases but the CV LMICs community at large has no access to information regarding the types of data collected or patient and program outcomes achieved thus far. To paraphrase Peter Drucker, what we measure we improve. Building a CV program registry and a global CV outcome database for LMICs is a high-order need. The scope of this task is enormous and will require dedicated resources, leadership, and constituent participation. Deliberate decisions need to be made regarding the types of data to collect, standardization of collection methods, data verification as well as building and maintaining the data. More importantly, these initiatives involve the courage to undergo systematic self-examination with the potentials for quality improvement and succeed. The WSPCHS is uniquely positioned to play a leadership role in this effort.
Establishing a Collaborative Framework is Needed to Improve Communication and Enable Collaborations Among NGO and LMIC Programs
The survey identified 80 CV NGOs supporting 92 LMICs. These outreach efforts extend into every continent but they are not well coordinated. For example, many LMICs in Asia, Africa, and parts of Europe receive dual supports from both Europe and North America (Figure 1). In an editorial, Dr A. Thomas Pezzella urged the community, “Let’s get everyone into the boat, going in the same direction.”16 Cultivating a collaborative working culture and framework among NGOs and LMICs strengthens the identity of the LMIC CV community of practice and can help the NGO and LMIC programs be more effective in delivering CV care in LMICs. Concrete steps to support the collaborative framework include global meetings of the WSPCHS, the World Congresses of Pediatric Cardiology and Cardiac Surgery, or the Global Forum on Humanitarian Medicine. These gatherings are important opportunities for face-to-face networking, sharing best practices, coordinating training programs, and exploring future collaborations. In addition, a 21st century Web-based collaborative forum can facilitate ongoing interactions among constituents of the LMICs CV community of practice, including clinicians, patients and families, CV NGOs, philanthropists, supply companies, and health care advocates or policy makers. This interactive “Common” would be where the community collaborates to solve problems that plague the community at large share cross-linked calendars of NGOs outreach efforts and access central resources such as equipment warehouses. Multilingual education curriculum developed by clinical experts in CV diagnostic imaging, surgical- or catheter-based intervention, arrhythmias, or intensive care can be readily accessed by clinicians in LMICs.
Limitations
Findings from this project are based on survey questions sent to members of PediHeart and WSPCHS. The results are prone to reporter bias and respondents’ variable depth of knowledge of the NGO programs. The sample size and the amount of data collected are also limited by survey reach and response rates. Furthermore, due to resource constraints, follow-up interviews were not conducted with the NGOs for qualitative data or elaboration on the site-specific capabilities.
Conclusions and Future Directions
Disparity and inadequacy in pediatric CV services remain an important problem for LMICs. A global consensus and coordinated efforts are needed to guide strategies on the development of regional centers of excellence, a global outcome database, and a CV program registry. Infrastructure development and training for the LMIC clinicians should remain a high priority. It is said that “Give a man a fish and he will eat for a day; Teach a man to fish and he will eat for a lifetime.” Future efforts should be held accountable for measurable impacts such as growth in the number of independent LMIC programs as well as reduction in mortality and patient waiting lists.
Acknowledgments
We appreciate editorial supports from Stacey Tobin PhD in the preparation of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by advocacy funding from the Department of Pediatrics at Ann & Robert H. Lurie Children’s Hospital of Chicago, IL, USA.
Abbreviations and Acronyms
- CHD
congenital heart disease
- CPB
cardiopulmonary bypass
- CV
cardiovascular
- COEs
centers of excellence
- LMICs
low- and middle-income countries
- NGOs
nongovernmental organizations
- WSPCHS
World Society for Pediatric and Congenital Heart Surgery
- WHO
World Health Organization
Appendix A: List of Nongovernmental Cardiovascular Organizations
Cardiovascular Nongovernmental Organizations and Contacts Information
Asociación de Ayuda a Niños en Estado Crítico, ABP (ADANEC ABP), Chiapas, Mexico
Aiutare i Bambini Onlus, To Help Children Foundation, Milan, Italy
Akemi Chan Fund
http://sankei.jp/business/bu_akemi.html
Associazione Marchigiana per il Bambino Cardiopatico (Heart Is Life), Ancona, Italy
Association of Baptists for World Evangelism, Carolyn Kempton Memorial Hospital
David Harris MD, http://www.togo.abwe.org/kkmch-hbb
Bakoulev Scientific Center for Cardiovascular Surgery
Sergey Prosolov MD, www.bakulev.ru
Bambini Cardiopatici Nel Mondo
Alessandro Frigiola MD, www.bambinicardiopatici.it
Cardiac Kids Foundation of Florida
Cardiostart International
Cardiothoracic Associates, Corpus Christi, Texas, USA
Lucian A. Durham, MD, PhD, http://jmarkmoralesmd.com/international-outreach/
CARE Hospitals
Saurabh Varshney MD, drsaurabhvarshney@gmail.com, http://www.carehospitals.com/
Chain of Hope, UK
Chaîne de l’Espoir-Keten van Hoop Belgique
Children’s Hearts, UK
http://www.childrenshearts.org.uk/
Children’s Heart Link, Minnesota, USA
http://www.childrensheartlink.org/
Children’s Heart Group, Penn State, Pennsylvania, USA
http://www.pennstatehershey.org/web/globalhealth/home/outreach
Children’s Mercy Hospital, Kansas, Missouri
Christian Medical College and Hospital, Vellore, Tamil Nadu State, India
Coeurs pour tous (Hearts for All), Geneva, Switzerland
http://www.cptg.ch/fr/start.html
Congenital Heart Intervention Mission Support, Chicago, Illinois, USA
East Meets West, Oakland, California, USA
For Hearts and Souls, San Antonio Texas, USA
Fundación Abrigo, Tegucigalpa, Honduras
http://www.trafigurafoundation.com/
Fundación Aldo Castaneda, Guatemala City, Guatemala
www.fundacionaldocastaneda.org
Fundación Clínica Shaio, Bogota, Colombia
Fundación Corazones del Cibao, Santiago, Dominican Republic
http://www.fundacioncorazonesdelcibao.org.do/
Furlanetto Institute, São Paulo, Brazil, Heart-Life-Children
Glaucio Furlanetto PhD, gfurlanetto@terra.com.br, beatrizfurlanetto@gmail.com
Gift of Life Phoenix, Arizona, USA
Gift of Life International, Valhalla, New York, USA
www.giftoflifeinternational.org
Healing Hearts Northwest, Spokane, Washington
http://healingheartsnorthwest.com/
Heartaid Trust, Nigeria
Fidelia Bode-Thomas MD, www.heartaidtrust.org
Heart Beat Connection, Vietnam
Heart Care International, Greenwich, Connecticut, USA
Heart to Heart International Children’s Medical Alliance, Oakland, California, USA
Heartbeat International, Beirut, Lebanon
HeartGift Foundation, Austin, Texas, USA
Hearts and Minds of Ghana, Boston, Massachusetts, USA
Heartsandmindsofghana@gmail.com; www.heartsandmindsofghana.org/
Hearts with Hope, Los Angeles, California, USA
Juan Alejos MD, www.heartswithhope.org
Hospital Infantil de Mexico Fedderico Gomez, Mexico
Hospital Nacional de ninos de Costa Rica, San Jose, Costa Rica
Hospital Sant Joan de Deu, Barcelona, Spain
Hrudaya Cure A Little Heart Foundation, Hyderabad, India
International Children’s Heart Foundation, Memphis, Tennessee, USA
International Children’s Heart Fund, Worcester, Massachusetts, USA
Angelo Thomas Pezzella MD, http://www.ichfund.org/
Kenyatta National Hospital, Kenya, Nairobi, Kenya
Leiden University Medical Center, Netherlands
Lifeline, Variety Club, USA
Los Cabos Children’s Foundation, Sioux Falls, South Dakota, USA
Lund University Hospital, Sweden
http://www.lunduniversity.lu.se/
Medstar Washington Hospital Center, Washington, DC, USA
Jennifer Ellis MD and Louis Kanda MD, http://www.whcenter.org/
Mercy Medical Center, Des Moines, Iowa, USA
http://www.mercydesmoines.org/
Mt. Fuji Shizuoka Children’s Hospital, Japan
Norataka Ota MD; nori.ota@hotmail.com
Nuskin International
http://www.forceforgood.org/ffg/en/home.html
Open Hearts Haiti, New York, New York, USA
Francois Lacour-Gayet MD, www.openheartshaiti.org
Operation Open Heart, The Sydney Adventist Hospital, Sydney, Australia
www.sah.org.au/healthcare-outreach
Palestinian Children’s Relief Fund, Lebanon
Physicians Across Continents, Saudi Arabia
https://www.facebook.com/people/Physicians-Across-Continents/
Preemptive Love Organization, USA and Iraq
Project Hope, Millwood, Virginia, USA
Project Kids Worldwide, New York, New York
http://projectkidsworldwide.com/
Project open hearts, Denver, Colorado, USA
Pushpanjali Crosslay Hospital, Department of Cardiac Surgery, India
http://pushpanjalicrosslayhospital.com/
Resources Exchange International, REI-Vietnam
Rumah Sakit Medika BSD, Indonesia
hafil@abdulgani.com, http://www.rs-medikabsd.co.id/
Santiago Corazon, Medellin, Colombia
Save a Child’s Heart Foundation, Israel
Save a Heart Mission, Miami, Florida, USA
Carlos Traconis MD, www.saveaheartmission.com
Shaheed Rajaei Cardiovascular Research Center, Tehran, Iran
Surgeons of Hope Foundation, New York, New York, USA
Teamheart, Newton, Massachusetts, USA
R. Morton Bolman MD, www.teamheart.org
Hearts of East Africa, Tenwek Heart Project, Franklin, Tennessee, USA
Michael Liske, MD, http://www.heartsofafrica.org
TAIYARI, Hearts in Your Hands, Guadalajara, Mexico
The Cardiac Children Heart Foundation of Thailand
Tyumen Regional Hospital; Department of Pediatric Cardiac Surgery, Russia
Gorbatikovj@mail.ru
University of Padova, Pediatric Cardiac Surgery Unit, Italy
UVA-Cedimat Cardiac Charity, University of Virginia, Charlottesville, Virginia, USA
Scott Lim MD, http://www.medicine.virginia.edu/clinical/departments/medicine/divisions/cardiology/seminars/service-opps/overview
Variety Children’s, USA
Vina Capital Foundation, Vietnam
Voci e Volti, Onlus (Voices and Faces) Verona, Italy
http://www.vocievolti.it/home.html
Walter Sisulu Paediatric Cardiac Foundation, South Africa
Robin H. Kinsley MD; rkinsley@iafrica.com; http://www.wspcf.org.za/foundation.php
World Children’s Initiative, Menlo Park, California, USA
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- 1. [Accessed May 24.]; http://data.worldbank.org/about/country-classifications.
- 2.Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39(12):1890–1900. doi: 10.1016/s0735-1097(02)01886-7. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. [Accessed May 24th, 2013.];Causes of death 2008. http://www.who.int/healthinfo/global_burden_disease/cod_2008_sources_methods.pdf.
- 4.Carapetis JR. Rheumatic heart disease in developing countries. N Engl J Med. 2007;357(5):439–441. doi: 10.1056/NEJMp078039. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Rheumatic Fever and Rheumatic Heart Disease. Report of a WHO Expert Consultation, 29 October–1 November 2001. Geneva: World Health Organization; 2004. (Technical Report Series, No. 923) [Google Scholar]
- 6.Cox JL. Presidential address: changing boundaries. J Thorac Cardiovasc Surg. 2001;122(3):413–418. doi: 10.1067/mtc.2001.118489. [DOI] [PubMed] [Google Scholar]
- 7.Unger F. Worldwide survey on cardiac interventions 1995. Cor Europaeum. 1999;7:128–146. [Google Scholar]
- 8.Tchervenkov CI, Jacobs JP, Bernier PL, et al. The improvement of care for paediatric and congenital cardiac disease across the World: a challenge for the world society for pediatric and congenital heart surgery. Cardiol Young. 2008;18(suppl 2):63–69. doi: 10.1017/S1047951108002801. [DOI] [PubMed] [Google Scholar]
- 9.Neirotti R. Paediatric cardiac surgery in less privileged parts of the world. Cardiol Young. 2004;14(3):341–346. doi: 10.1017/S1047951104003191. [DOI] [PubMed] [Google Scholar]
- 10.Dearani JA, Neirotti R, Kohnke EJ, et al. Improving pediatric cardiac surgical care in developing countries: matching resources to needs. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2010;13(1):35–43. doi: 10.1053/j.pcsu.2010.02.001. [DOI] [PubMed] [Google Scholar]
- 11.Jonas RA. Rewards, risks, and responsibilities of globalization for the cardiothoracic surgeon. J Thorac Cardiovasc Surg. 2007;134(1):1–14. doi: 10.1016/j.jtcvs.2006.09.067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Novick WM, Stidham GL, Karl TR, et al. Paediatric cardiac assistance in developing and transitional countries: the impact of a fourteen year effort. Cardiol Young. 2008;18(3):316–323. doi: 10.1017/S1047951108002175. [DOI] [PubMed] [Google Scholar]
- 13.Pezzella AT. International cardiac surgery: a global perspective. Semin Thorac Cardiovasc Surg. 2002;14(4):298–320. doi: 10.1053/stcs.2002.0140298. [DOI] [PubMed] [Google Scholar]
- 14.Laslett LJ, Alagona P, Jr, Clark BA, 3rd, et al. The worldwide environment of cardiovascular disease: prevalence, diagnosis, therapy, and policy issues: a report from the American college of cardiology. J Am Coll Cardiol. 2012;60(25 suppl):S1–S49. doi: 10.1016/j.jacc.2012.11.002. [DOI] [PubMed] [Google Scholar]
- 15.Velebit V, Montessuit M, Bednarkiewicz M, Khatchatourian G, Mueller X, Neidhart P. The development of cardiac surgery in an emerging country: a completed project. Tex Heart Inst J. 2008;35(3):301–306. [PMC free article] [PubMed] [Google Scholar]
- 16.Pezzella AT. Global statistics/outcomes. J Thorac Cardiovasc Surg. 2006;132(3):726. doi: 10.1016/j.jtcvs.2006.05.009. [DOI] [PubMed] [Google Scholar]