

Abstract
Sever studies were performed to assess the association between multiple sclerosis (MS) and fracture risk. However, the results were inconsistent and inconclusive. In the present study, the possible association was investigated by a meta-analysis. Eligible articles were identified for the period up to August 2014. Pooled risk ratios (RR) with 95% confidence intervals (CI) were appropriately derived from random-effects models. Nine studies with more than 9,000,000 subjects were eligible. We found that MS was significant associated with fracture risk in overall population (OR = 1.58, 95% CI 1.36-1.84, P < 0.01). In terms of subgroup analyses by fracture sites, the associations were significant in femur (RR = 4.57, 95% CI 3.01-6.69, P < 0.01), hip (RR = 3.01, 95% CI 2.72-3.41, P < 0.01), tibia (RR = 2.72, 95% CI 2.22-3.32, P < 0.01), humerus (RR = 1.78, 95% CI 1.12-2.40, P = 0.02), pelvis (RR = 1.34, 95% CI 1.12-1.67, P < 0.01), and vertebrae (RR = 1.30, 95% CI 1.13-1.69, P < 0.01). This meta-analysis suggested that MS may be associated with fracture development.
Keywords: Multiple sclerosis, fracture, meta-analysis
Introduction
Multiple sclerosis (MS) is a neuroinflammatory disease which can affect all functions of the central nervous system. MS is the most common cause of non-traumatic disability among young and middle-aged adults in the western hemisphere, and as such, leads to high rates of disability and societal costs [1]. Various socio-demographic factors are associated with a higher risk for MS, such as female sex [2], place of residence during childhood [3], and low educational level [4].
Fractures represent a serious health risk in the elderly, with a significant associated morbidity and mortality. Approximately 13.5% of those who suffer a hip fracture die within 6 months and 24% within 1 year of the episode [5]. The identifiable risk factors for fracture are advanced age, female sex, osteoporosis, low vitamin D levels and calcium intake, and prior history of fractures [6]. Several studies found MS to be a risk factor in fracture, but other studies showed no association between MS and risk of fracture. These studies revealed an inconsistent conclusion [7-15]. Therefore, we conducted a meta-analysis to assess the association between MS and fracture risk.
Methods
Publication search
A computerized literature search was performed to identify the relevant studies from five electronic databases including PubMed, EMBASE, China National Knowledge Infrastructure (CNKI), Database of Chinese Scientific and Technical Periodicals, and China Biology Medical literature database (CBM). The search terms were used as follows: (multiple sclerosis) and (fractures or fracture). All searched studies were retrieved and the bibliographies were checked for other relevant publications.
Inclusion and exclusion criteria
The following criteria were used for the literature selection: first, studies should concern the association of MS and fracture risk; second, studies must be observational studies (case-control or cohort); third, studies must offer the size of the sample, risk ratios (RRs) and their 95% confidence intervals (CIs). Studies were excluded if one of the following existed: first, studies were not relevant to MS or fracture; second, no useful data were not reported; third, reviews and abstracts. As for the studies from the same institution, only the one with the largest sample size was included. No language restrictions were imposed.
Data extraction
Data were extracted by two authors independently. If encountered the conflicting evaluations, an agreement was reached following a discussion; if could not reached agreement, another author was consulted to resolve the debate. The following information was extracted from each study: first author, year of publication, ethnicity, age, gender, sample size.
Methodological quality assessment
Two authors assessed the study quality. The Newcastle-Ottawa Scale (NOS) was used to evaluate the methodological quality [16].
Statistical analysis
We estimated the RR with 95% CI for fracture. A random effects model (the DerSimonian and Laird method) was used. Statistical heterogeneity among studies was evaluated using the Q and I2 statistics. Subgroup analyses by site of fracture were performed. The publication bias was assessed using the Egger’s linear regression test [17]. All statistical analyses were performed with the STATA software (version 12.0, Stata Corporation, College Station, Texas).
Results
Characteristics of studies
A flowchart of the process of study selection is shown in Figure 1. Based on the inclusion and exclusion criteria, a total of 9 articles were included in the meta-analysis after full-text review [7-15]. The main characteristics of included studies are presented in Table 1. All of the studies were conducted in Caucasians. Two studies used female subjects. The quality scores of the studies were more than 7, suggesting that the quality of the included studies was high.
Figure 1.
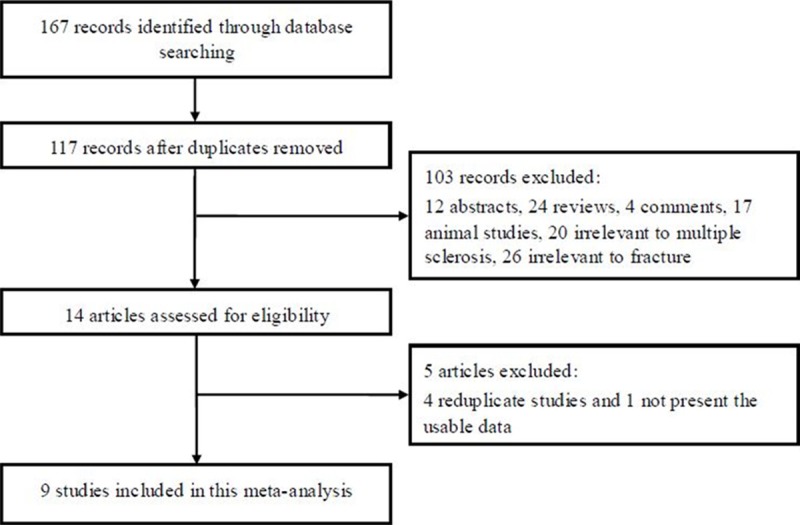
The flow diagram of search process.
Table 1.
Characteristics of the studies
| First author | Year | Race | Mean age | Gender | No. of participants | Quality score |
|---|---|---|---|---|---|---|
| Bazelier 1 | 2011 | Caucasian | 44.8 | Mixed | 38925 | 8 |
| Moen | 2011 | Caucasian | 37.1 | Mixed | 231 | 7 |
| Bazelier 2 | 2012 | Caucasian | 43.6 | Mixed | 15056 | 7 |
| Bazelier 3 | 2012 | Caucasian | 46.4 | Mixed | 68430 | 8 |
| Bazelier 4 | 2012 | Caucasian | 36.9 | Mixed | 18399 | 8 |
| Dennison | 2012 | Caucasian | NR | Female | 52960 | 7 |
| Ramagopalan | 2012 | Caucasian | NR | Mixed | 7908570 | 9 |
| Bhattacharya | 2014 | Caucasian | 65 | Mixed | 1066404 | 9 |
| Gregson | 2014 | Caucasian | ≥ 55 | Female | 60393 | 7 |
NA, not reported.
Meta-analysis results
The results of this meta-analysis are shown in Table 2. We found that MS was significant associated with fracture risk in overall population (OR = 1.58, 95% CI 1.36-1.84, P < 0.01, Figure 2). In terms of subgroup analyses by fracture sites, the associations were significant in femur (RR = 4.57, 95% CI 3.01-6.69, P < 0.01), hip (RR = 3.01, 95% CI 2.72-3.41, P < 0.01), tibia (RR = 2.72, 95% CI 2.22-3.32, P < 0.01), humerus (RR = 1.78, 95% CI 1.12-2.40, P = 0.02), pelvis (RR = 1.34, 95% CI 1.12-1.67, P < 0.01), and vertebrae (RR = 1.30, 95% CI 1.13-1.69, P < 0.01).
Table 2.
Results of meta-analysis and subgroup analysis
| RR (95% CI) | P Value | I 2 (%) | |
|---|---|---|---|
| Overall | 1.58 (1.36-1.84) | < 0.01 | 98 |
| Femur | 4.57 (3.01-6.69) | < 0.01 | 70 |
| Hip | 3.01 (2.72-3.41) | < 0.01 | 0 |
| Tibia | 2.72 (2.22-3.32) | < 0.01 | 55 |
| Humerus | 1.78 (1.12-2.40) | 0.02 | 52 |
| Pelvis | 1.34 (1.12-1.67) | < 0.01 | 0 |
| Vertebrae | 1.33 (1.12-1.59) | < 0.01 | 0 |
| Ribs | 1.10 (0.71-1.58) | 0.48 | 31 |
| Radius/ulna | 0.78 (0.56-1.03) | 0.13 | 0 |
Figure 2.
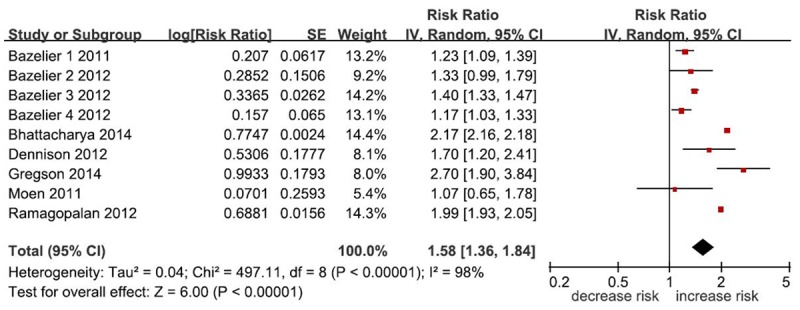
Meta-analysis between MS and fracture risk.
In order to compare the difference and evaluate the sensitivity of the meta-analyses, we used both models (the fixed effect model and random effect model) to evaluate the stability of the meta-analysis. All the results were not materially altered (data not shown). Hence, results of the sensitivity analysis suggest that the data in this meta-analysis are relatively stable and credible. There was no publication bias (P = 0.24).
Discussion
Although many studies analyzing the research results about MS and fracture risk, definite conclusions cannot be drawn. Therefore, we did this meta-analysis to estimate the relationship between MS and fracture risk. To our knowledge, this is the first meta-analysis regarding MS and fracture risk. The meta-analysis involved nine articles. The results from this meta-analysis showed that MS was significantly associated increased fracture risk. When we performed the subgroup analysis by site of fracture, significant association with susceptibility for the development of fracture was found in femur, hip, tibia, humerus, pelvis, and vertebrae.
There might be some reasons could be explained why MS patients had an increased fracture risk. MS is associated with an increased risk of osteoporosis and reduced bone mass, which when combined with the functional impairments of the disease, augments the possibility of fractures [18]. The development of osteoporosis in MS patients can be related to the cumulative effects of various factors. Physical inactivity and reduced mechanical load on the bones (offsetting gravity) is likely the major contributing factor for osteoporosis in MS [19]. Other possible factors leading to reduced bone mass are low vitamin D levels, use of medications such as glucocorticoids and anticonvulsants, and the role of the inflammatory processes of the disease [20].
Our meta-analysis has several strengths. First, we have followed the inclusion and exclusion criteria strictly to reduce possible selection bias. Second, Egger’s linear regression tests were used to assess publication bias. Third, the sensitivity analysis had been performed to confirm the reliability and stability of this meta-analysis.
This meta-analysis also had several limitations. First, there was only 9 studies investigated the association of MS and fracture risk. Therefore, more studies with large sample sizes are needed to further identify the association. Second, because small negative studies are less likely to published, the possibility of publication bias cannot be ruled out completely, even though the Egger’s test did not provide the evidence of publication bias in this meta-analysis. Third, we did not evaluate the impact of lifetime corticosteroid use, nor examine specific doses of vitamin D.
In conclusion, this meta-analysis showed MS conferred significantly increased fracture risk. This result should be validated in the future studies.
Disclosure of conflict of interest
None.
References
- 1.Amato MP, Battaglia MA, Caputo D, Fattore G, Gerzeli S, Pitaro M, Reggio A, Trojano M Mu. S. I. C. Study Group. The costs of multiple sclerosis: a cross-sectional, multicenter cost-of-illness study in Italy. J Neurol. 2002;249:152–163. doi: 10.1007/pl00007858. [DOI] [PubMed] [Google Scholar]
- 2.Alonso A, Hernán MA. Temporal trends in the incidence of multiple sclerosis: a systematic review. Neurology. 2008;71:129–35. doi: 10.1212/01.wnl.0000316802.35974.34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kennedy J, O’Connor P, Sadovnick AD, Perara M, Yee I, Banwell B. Age at onset of multiple sclerosis may be influenced by place of residence during childhood rather than ancestry. Neuroepidemiology. 2006;26:162–167. doi: 10.1159/000091658. [DOI] [PubMed] [Google Scholar]
- 4.Riise T, Kirkeleit J, Aarseth JH, Farbu E, Midgard R, Mygland Å, Eikeland R, Mørland TJ, Telstad W, Førland PT, Myhr KM. Risk of MS is not associated with exposure to crude oil, but increases with low level of education. Mult Scler. 2011;17:780–787. doi: 10.1177/1352458510397686. [DOI] [PubMed] [Google Scholar]
- 5.Hannan EL, Magaziner J, Wang JJ, Eastwood EA, Silberzweig SB, Gilbert M, Morrison RS, McLaughlin MA, Orosz GM, Siu AL. Mortality and locomotion 6 months after hospitalization for hip fracture: risk factors and risk-adjusted hospital outcomes. JAMA. 2001;285:2736–2742. doi: 10.1001/jama.285.21.2736. [DOI] [PubMed] [Google Scholar]
- 6.Carriero FP, Christmas C. In the clinic. Hip fracture. Ann Intern Med. 2011;155:ITC6-1–ITC6-15. doi: 10.7326/0003-4819-155-11-201112060-01006. quiz ITC6-16. [DOI] [PubMed] [Google Scholar]
- 7.Bazelier MT, van Staa TP, Uitdehaag BM, Cooper C, Leufkens HG, Vestergaard P, Bentzen J, de Vries F. The risk of fracture in patients with multiple sclerosis: the UK general practice research database. J Bone Miner Res. 2011;26:2271–9. doi: 10.1002/jbmr.418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Moen SM, Celius EG, Nordsletten L, Holmøy T. Fractures and falls in patients with newly diagnosed clinically isolated syndrome and multiple sclerosis. Acta Neurol Scand Suppl. 2011;191:79–82. doi: 10.1111/j.1600-0404.2011.01548.x. [DOI] [PubMed] [Google Scholar]
- 9.Bazelier MT, van Staa TP, Uitdehaag BM, Cooper C, Leufkens HG, Vestergaard P, Herings RM, de Vries F. Risk of fractures in patients with multiple sclerosis A population-based cohort study. Neurology. 2012;78:1967–73. doi: 10.1212/WNL.0b013e318259e0ff. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bazelier MT, de Vries F, Bentzen J, Vestergaard P, Leufkens HG, van Staa TP, Koch-Henriksen N. Incidence of fractures in patients with multiple sclerosis: the Danish National Health Registers. Mult Scler. 2012;18:622–7. doi: 10.1177/1352458511426739. [DOI] [PubMed] [Google Scholar]
- 11.Bazelier MT, Bentzen J, Vestergaard P, Stenager E, Leufkens HG, van Staa TP, de Vries F. The risk of fracture in incident multiple sclerosis patients: the Danish National Health Registers. Mult Scler. 2012;18:1609–16. doi: 10.1177/1352458512442755. [DOI] [PubMed] [Google Scholar]
- 12.Dennison EM, Compston JE, Flahive J, Siris ES, Gehlbach SH, Adachi JD, Boonen S, Chapurlat R, Díez-Pérez A, Anderson FA Jr, Hooven FH, LaCroix AZ, Lindsay R, Netelenbos JC, Pfeilschifter J, Rossini M, Roux C, Saag KG, Sambrook P, Silverman S, Watts NB, Greenspan SL, Premaor M, Cooper C GLOW Investigators. Effect of co-morbidities on fracture risk: findings from the Global Longitudinal Study of Osteoporosis in Women (GLOW) Bone. 2012;50:1288–93. doi: 10.1016/j.bone.2012.02.639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ramagopalan SV, Seminog O, Goldacre R, Goldacre MJ. Risk of fractures in patients with multiple sclerosis: record-linkage study. BMC Neurol. 2012;12:135. doi: 10.1186/1471-2377-12-135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bhattacharya RK, Vaishnav N, Dubinsky RM. Is there an increased risk of hip fracture in multiple sclerosis? Analysis of the Nationwide Inpatient Sample. J Multidiscip Healthc. 2014;7:119–22. doi: 10.2147/JMDH.S54786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gregson CL, Dennison EM, Compston JE, Adami S, Adachi JD, Anderson FA Jr, Boonen S, Chapurlat R, Díez-Pérez A, Greenspan SL, Hooven FH, LaCroix AZ, Nieves JW, Netelenbos JC, Pfeilschifter J, Rossini M, Roux C, Saag KG, Silverman S, Siris ES, Watts NB, Wyman A, Cooper C GLOW Investigators. Disease-specific perception of fracture risk and incident fracture rates: GLOW cohort study. Osteoporos Int. 2014;25:85–95. doi: 10.1007/s00198-013-2438-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. URL: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- 17.Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sioka C, Kyritsis AP, Fotopoulos A. Multiple sclerosis, osteoporosis, and vitamin D. J Neurol Sci. 2009;287:1–6. doi: 10.1016/j.jns.2009.09.012. [DOI] [PubMed] [Google Scholar]
- 19.Josyula S, Mehta BK, Karmon Y, Teter B, Batista S, Ostroff J, Weinstock-Guttman B. The nervous system’s potential role in multiple sclerosis associated bone loss. J Neurol Sci. 2012;319:8–14. doi: 10.1016/j.jns.2012.03.026. [DOI] [PubMed] [Google Scholar]
- 20.Gibson JC, Summers GD. Bone health in multiple sclerosis. Osteoporos Int. 2011;22:2935–49. doi: 10.1007/s00198-011-1644-8. [DOI] [PubMed] [Google Scholar]