

Highlights
-
•
Clear cell adenocarcinoma arising from endometriosis is very rare.
-
•
Preoperative diagnosis of the malignant transformation in endometriosis is very difficult.
-
•
The patient was undergone low anterior resection under the diagnosis of rectal carcinoma.
-
•
Sampson's criteria are useful for diagnosis of the malignant transformation in endometriosis.
-
•
The prognosis of malignant transformation in endometriosis is poor.
Keywords: Clear cell adenocarcinoma, Endometriosis, Rectal tumor
Abstract
INTRODUCTION
Malignant transformation of intestinal endometriosis occurring in the extraovarian sites is extremely rare. We report a very rare case of clear cell adenocarcinoma arising from endometriosis of the rectum.
PRESENTATION OF CASE
An 83-year-old woman was admitted with the complaint of hematochezia. Colonoscopy revealed a tumor around about half of the rectal circumference. Biopsy of the tumor revealed a well-differentiated adenocarcinoma. Low anterior resection was undergone laparoscopically under the diagnosis of rectal carcinoma. Histopathological examination revealed clear cell adenocarcinoma, invading the sub-serosa of the rectum, but no metastasis of the lymph nodes. Immunohistochemical staining showed strong positivity for cytokeratin 7, but no staining for cytokeratin 20 and CDX2. The tumor existed adjacent to the endometrial glands, which were stained positive for Estrogen receptor. Ultimately, the patient was diagnosed with clear cell adenocarcinoma arising from endometriosis. Eighteen months after surgery, there are no signs of tumor recurrence.
DISCUSSION
Clear cell adenocarcinoma arising from intestinal endometriosis has been reported in 7 cases, including our case. Careful observation is required because the prognosis of endometriosis after malignant transformation remains poor.
CONCLUSION
We report a very rare case of clear cell adenocarcinoma arising from endometriosis of the rectum treated by laparoscopic surgery.
1. Introduction
Malignant transformation in endometriosis is rare. While the precise incidence remains unknown, a 0.3–1.0% incidence has been reported.1 About 75% of the cases of malignant transformation have been reported to occur in the ovary, with the remainder occurring in extragonadal sites, most commonly the pelvic peritoneum, rectovaginal septum, colon/rectum, and vagina.2 About 70% of the histological types of endometriosis are endometrioid adenocarcinoma. The incidence of clear cell adenocarcinoma in the extraovarian sites of endometriosis is 4.5%.2–5 This paper reports a very rare case of clear cell adenocarcinoma arising from endometriosis in the rectum.
2. Presentation of case
An 83-year-old woman was admitted in June 2012, with the complaint of hematochezia. She has not suffered from endometriosis, and has not been treated with any hormonal agents.
Preoperative serum tumor-marker, carcinoembryonic antigen (CEA), carbohydrate antigen 19–9 (CA19-9), carbohydrate antigen125 (CA125) levels were not elevated. Barium enema showed a 45-mm-long polypoid lesion, accompanied with a trapezoidal change, located at the anterior wall of the rectum (Fig. 1). Abdominal computed tomography showed a heterogeneous enhanced wall thickness of the rectum (Fig. 2a). No metastasis was found in the liver, and lymph nodes in the mesorectum were not swollen. Pelvic magnetic resonance imaging showed a heterogeneous intensity mass in the rectum on T1 weighted imaging, with no suspicion of invasion to the uterus and sacrum (Fig. 2b). Bilateral ovaries were not swollen. Colonoscopy revealed tumor sizes around half of the rectal circumference, at the upper rectum, 13 cm from the anal verge. Biopsy of the tumor revealed a well-differentiated adenocarcinoma. Although, it was histologically atypical of a carcinoma of the colon, we could not perform the further histological examination. Consequently, we diagnosed the patient as having rectal carcinoma, and planned to perform laparoscopic low anterior resection. Under general anesthesia, the first port for the camera was created at the umbilicus. Next, a 12 mm port was inserted through the right lower quadrant, three 5 mm ports were placed at the right upper, left upper and lower quadrants, allowing placement of a total of 5 ports. Upon observation of an intraperitoneal cavity during laparoscopy, metastatic liver tumor, peritoneal tumor, and swollen lymph nodes were not recognized. Both ovaries appeared normal. The rectal tumor was partially adherent to the visceral peritoneum of the left side of the uterus. It was suspicious that the tumor invaded to the peritoneum. Thus, the adhered part was resected. Frozen section was performed and demonstrated no invasion to the peritoneum. After that, we proceeded to dissect the mesorectum circumferentially, and resect of the distal rectum by the endoscopic liner stapler. Reconstruction was done with the circular stapler, using the method of the double stapling technique (DST). In the resected specimen, a polypoid ulcerated tumor, measuring 38 mm × 38 mm in diameter (Fig. 3). Histopathological examination showed that clear cell adenocarcinoma was contiguous with endometriosis, infiltrating through the sub-serosa (Fig. 4a and b). In immunohistological staining, the tumor was positive for CK7, and negative for CK20, CDX2, Estorogen receptor (ER), progesterone receptor (PgR). Endometrial glands and stroma adjacent to the tumor were positive for ER (Fig. 4c and d). Finally, it was diagnosed as clear cell adenocarcinoma arising in endometriosis of the rectum. No metastatic lymph nodes were recognized pathologically.
Fig. 1.
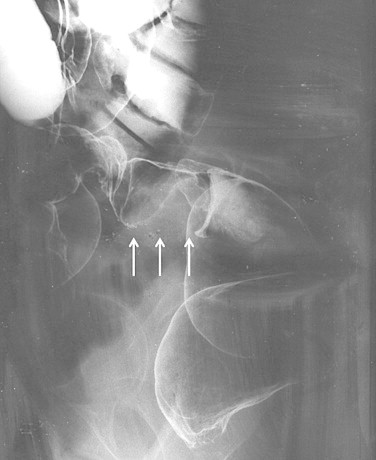
Barium enema showed a 45-mm-long polypoid lesion (arrow), with a trapezoidal change at the anterior wall of the rectum.
Fig. 2.
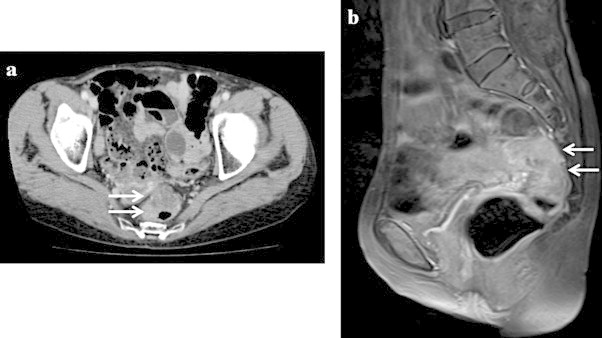
Abdominal computed tomography examination showed enhanced wall thickness of the rectum with no suspicion of invasion of the surrounding organs (arrow). There was no sign of swelling of the lymph nodes in the mesorectum (a). Pelvic magnetic resonance imaging (T1 weighted image) showed a heterogeneous intensity mass of the rectum, with no suspicious uterus or sacrum (b).
Fig. 3.

The surgical specimen consisted of a 14.0 cm length of the rectum. A polypoid ulcerated tumor, measuring 38 mm × 33 mm in diameter.
Fig. 4.
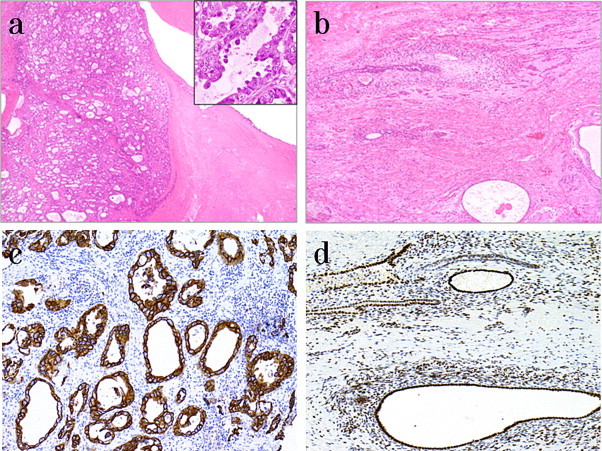
Clear cell adenocarcinoma was contiguous with endometriosis, infiltrating throughout the sub-serosa. H&E, ×100 (a, b). Strong CK7-positive staining of tumor cells. CK7, ×100 (c). ER-positive staining of the endometrial glands and stromal cells. ER, ×40 (d).
After surgery, she did not receive any chemotherapy of her own will. At 18-month follow-up, there was no evidence of recurrence.
3. Discussion
While adenocarcinoma arising in endometriosis has occasionally been reported in the ovaries, there has been a report that the rate of malignant transformation in endometriosis is 0.7–1.0%, with 80% occurring in the ovary.1 However, malignant transformation of endometriosis at extragonadal sites remains rare; the rates of occurrence are 5.7%, rectovaginal septum are 4.3%, colorectum are 4.3%.1 Moreover, the malignant transformation of clear cell adenocarcinoma occurring in the extraovarian sites continues to be extremely rare; with an incidence of 4.5%.1–5,7–8 Malignant transformation in endometriosis was first described by Sampson in 1925,9 who recommended that three criteria be met for a definitive diagnosis; namely: (1) there should be histological evidence of endometriosis in close proximity to the tumor; (2) no other primary site of malignancy should be identified; and (3) the histological appearance of the tumor should be compatible with an origin in endometriosis. Scoot10 also proposed additional criteria that transition from a normal endometrial gland to the malignant change in endometriosis was seen histologically in 1953. In our case, Sampson's criteria were all satisfied, but Scoot's additional criterion was not.
Immunohistological staining of cytokeratin (CK) is useful for discrimination between colon cancer and endometrioid adenocarcinoma. Chu et al.11 reported that CK7−/CK20+ were recognized in 75–95% cases of colonic adenocarcinoma; otherwise CK7+/CK20− were recognized in over 80% of cases of endometrioid adenocarcinoma. In our case, immunohistological staining showed CK7+/CK20−. Thus, this case was diagnosed as arising from endometriosis.
Clear cell adenocarcinoma arising from bowel endometriosis has been reported in 7 cases, including our case (Table 1). The age of onset is to 41 years from 83 years; with an average age of 56.3 years. The chief complaint was hematochezia in all cases. It is very difficult to preoperatively diagnosis malignant transformation in endometriosis. A colonoscopy can sometimes be a helpful method to detect intestinal endometriosis. However, endoscopic findings or histological examination of superficial, endoscopic biopsy material may be difficult to assess definitively unless the tumor is exposed with destruction of the surface layers. In case adenocarcinoma is found by the endoscopic method, differential diagnosis of endometrial adenocarcinoma from primary colon carcinoma would be far more difficult.12 Including our case, all cases with a preoperative diagnosis were rectal carcinoma. Surgical resection is the first choice of treatment. Surgery had been performed laparoscopically in 2 out of 7 cases, including our case. Laparoscopic surgery is superior to open resection, with respect to the observation of the intraperitoneal cavity; especially narrow spaces, such as the pelvis. We observed that the rectal tumor adhered to the surrounding organ or tissues, i.e., the ovaries and uterus laparoscopically, which led to curative operation. In addition to the surgical treatment, there has also been a report of the potential of hormonal treatment and systemic chemotherapy.1,6 While systemic chemotherapy uses multidrug chemotherapy, consisting of cisplatin, cyclophosphamide, epirubicin, carboplatin, Taxol etc., the therapeutic effect is generally poor. Meanwhile, the prognosis of malignant transformation in endometriosis remains poor.1 However, Ikeda et al. reported that the primary prognosis of patients without lymph node metastasis was good.13 Following surgery, chemotherapy was carried out in two cases. One reason was the recognition of metastatic lymph nodes, and the other was due to the size of the tumor. In our patient, no metastatic lymph nodes were seen. Consequently, she would not receive any chemotherapy postoperatively, following her wishes. It is necessary to carefully follow-up.
Table 1.
Clear cell adenocarcinoma arising from intestinal endometriosis.
| Author | Year | Age | Location | Symptoms | Operative methoda | Histology | Postoperative therapy | Prognosisb |
|---|---|---|---|---|---|---|---|---|
| 1. Sasaki14 | 1996 | 49 | Lower rectum | Hematochezia | APR (open), hysterectomy with bilateral salpingoophorectomy | Adeno ca | (–) | DOD (1 M) |
| SCCc | ||||||||
| Clear cell ca (unknown) | ||||||||
| 2. McCluggage et al.4 | 2001 | 65 | Upper rectum | Hematochezia abdrmnal pain | AR (open) | Clear cell adeno ca (CK7+/CK20−) | Unknown | Unknown |
| 3. Sawai15 | 2007 | 56 | Upper rectum | Hematochezia | LAR (open) | Clear cell adeno ca (CK7+/CK20−) | (+) paclitaxel, carboplatin | ANR (18 M) |
| 4. Houma16 | 2007 | 50 | Upper rectum | Hematochezia | LAR (open) | Clear cell adeno ca (CK7+/CK20−) | (+) paclitaxel, carhoplatin | ANR (6 M) |
| 5. Finkelstem et al.17 | 2010 | 41 | Upper rectum | Hematochezia diarrhea | AR (open) hysterectomy with bilateral salpingoophorectomy | Clear cell adeno ca (CK7+/CK20−) | (+) Taxol. carboplatin | Unknown |
| 6. Kyueng-Whan18 | 2012 | 50 | Rectum | Hematochezia | LAR (lap) | Clear cell adeno ca (CK7+/CK20−) | (–) | ANR (15 M) |
| 7. Our case | 2012 | 83 | Upper rectum | Hematochezia | AR (lap) | Clear cell adeno ca (CK7+/CK20) | (–) | ANR (18 M) |
AR, anterior resection; LAR, low anterior resection; APR, abdominoperineal resection.
Months after operation. ANR, alive with no recurrence; DOD, dead of disease.
Squamous cell carcinoma.
We report a very rare case of clear cell adenocarcinoma arising from endometriosis of the rectum treated by laparoscopic surgery.
Conflict of interest
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for the review of the Editor-in-Chief of this journal on request.
Author contributions
Y. Okazawa contributed in writing the paper. R. Takahashi helped in attending physician of the presented patient. K. Mizukoshi, K. Takehara, S. Ishiyama, M. Goto, A. Okuzawa, and Y. Tomiki supervised the study. K. Sugimoto, M. Takahashi, and Y. Kojima helped in attending physician of the presented patient. T. Yao contributed in writing the paper and supervised the study. K. Sakamoto helped in writing the paper and in complete supervision.
References
- 1.Heaps J.M., Nieberg R.K., Berek J.S. Malignant neoplasma arising in endometriosis. Obstet Gynecol. 1990;75:1023–1028. [PubMed] [Google Scholar]
- 2.Petersen V.C., Underwood J.C.E., Wells M., Shepherd N.A. Primary endometrioid adenocarcinoma of the large intestine arising in colorectal endometriosis. Histopathology. 2002;40:171–176. doi: 10.1046/j.1365-2559.2002.01313.x. [DOI] [PubMed] [Google Scholar]
- 3.Ibrahim F.H., Sidney S.G., Stephane L. Clear cell carcinoma arising in extraovarian endometriosis – report of three cases and review of the literature. Gynecol Oncol. 1990;39:314–320. doi: 10.1016/0090-8258(90)90259-n. [DOI] [PubMed] [Google Scholar]
- 4.McCluggage W.G., Desai V., Toner P.G., Calvert C.H. Clear cell adenocarcinoma of the colon arising in endometriosis: a rare variant of primary colonic adenocarcinoma. J Clin Pathol. 2001;54:76–77. doi: 10.1136/jcp.54.1.76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shimamoto T., Nagai Y., Hoshino Y. Clear cell carcinoma arising from sigmoidal subserosal endometriosis. Int J Clin Oncol. 1999;4:311–314. [Google Scholar]
- 6.Marks H. Ein Beitrag zur Frage der bosartigen Entartung der Endometriose. Chirurg. 1949;20:441–443. [Google Scholar]
- 7.Sainz de la Cuesta R., Eichhorn J.H., Rice L.W. Histologic transformation of benign endometriosis to early epithelial ovarian cancer. Gynecol Oncol. 1996;60:238–244. doi: 10.1006/gyno.1996.0032. [DOI] [PubMed] [Google Scholar]
- 8.Mostoufizadeh M., Scully R.E. Malignant tumors arising in endometriosis. Clin Obstet Gynecol. 1980;23:951–963. [PubMed] [Google Scholar]
- 9.Sampson J.A. Endometrial carcinoma of the ovary arising in endometrial tissue in that organ. Arch Surg. 1925;10:71–72. [Google Scholar]
- 10.Scott R.B. Malignant change in endometriosis. Obstet Gynecol. 1953;2:283–289. [PubMed] [Google Scholar]
- 11.Chu P., Wu E., Weiss L.M. Cytokeratin 7 and cytokeratin 20 expression in epithelial neoplasm: a survey of 435 cases. Mod Pathol. 2000;13:962–972. doi: 10.1038/modpathol.3880175. [DOI] [PubMed] [Google Scholar]
- 12.Kobayashi S., Sasaki M., Goto T., Asakage N., Sekine M., Suzuki T. Endometrioid adenocarcinoma arising from endometriosis of the rectosigmoid. Dig Endosc. 2010;22:59–63. doi: 10.1111/j.1443-1661.2009.00925.x. [DOI] [PubMed] [Google Scholar]
- 13.Ikeda K. A case of malignant transformation of rectal endometriosis arising from post operative of endometriosis. Clin Gynecol Obstet. 2004;58:1471–1475. [Google Scholar]
- 14.Sasaki M. A case of malignant mixed epithelial tumor arising from endometriosis of the rectovaginal septum. J Jpn Surg Assoc. 1996;57:2268–2272. [Google Scholar]
- 15.Sawai K. Endometrioid adenocarcinoma arising from enddometriosis of the rectum. J Jpn Surg Assoc. 2008;69:2063–2067. [Google Scholar]
- 16.Honma S. A case of clear cell adenocarcinoma arising in the endometriosis of the rectum. J Jpn Soc Coloproctol. 2009;62:416–419. [Google Scholar]
- 17.Finkelstein A., Levy G.H., Hui P. Clear cell adenocarcinoma of the colon arising in the background of endometriosis: a case report and diagnostic approach. Lab Med. 2010;41:111–114. [Google Scholar]
- 18.Kyueng-Whan Min. Primary clear cell adenocarcinoma arising from rectal endometriosis. Dig Endosc. 2013;25:204–215. doi: 10.1111/den.12008. [DOI] [PubMed] [Google Scholar]