

Abstract
Awareness of anatomical variations in lungs is essential during segmental or lobar resections of lungs. We studied the variations of fissures, lobes and hilar structures in 65 right and 73 left isolated lungs from the dissection hall. Horizontal fissure was absent in 3.07% and incomplete in 35.38% of right lungs. Four point six one percentage of right lungs had 3 fissures and 4 lobes. Three point zero seven percentage of right lungs had 3 arteries, 67.69% had 2 arteries, and 29.23% had only one artery in the hilum. Sixty-three point zero seven percentage of right lungs had two veins in the hilum; 32.30% had 3 veins in the hilum; and 4.61% had more than 3 veins in the hilum. Ninety-eight point four six percentage of right lungs showed 2 bronchi in the hilum, and 1.53% of them showed 3 bronchi in the hilum. Two of the right lungs (3.07%) had an artery passing across the oblique fissure. Fifteen point zero six percentage of left lungs showed incomplete oblique fissure and 2.73% showed 2 fissures and 3 lobes. Five point four seven percentage of left lungs showed 2 arteries and 94.52% had only one artery in the hilum. Eighty point eight two percentage of left lungs had two veins in the hilum and 19.17% had 3 veins in the hilum. Twenty-one point nine one percent of left lungs had 2 bronchi and 78.08% had only one bronchus in the hilum. The knowledge of variations in the lobar and hilar anatomy of the lung presented in this study is clinically important while interpreting the radiological images and performing surgical procedures.
Keywords: Lung, Hilum, Pulmonary, Lobe, Fissure
Introduction
The lungs are essential organs of respiration and are situated in the thoracic cavity on either side of the mediastinum. Being vital organs of respiration, the lungs are divided by fissures into lobes which facilitate movements of lobes in relation to one another. Amongst the pair, the right lung is divided into three lobes namely upper, middle and lower by oblique and horizontal fissures. The left lung is divided into two lobes namely upper and lower by oblique fissure [1]. The arrangement of lung tissue into lobes by fissures facilitates the movements of the lobes in relation to one another thus helping in uniform expansion of the whole lung in inspiration [2]. Behind the cardiac impression in mediastinal surface each lung shows a triangular depression named the hilum, where the structures which form the root of the lung enter and leave the organ. Both the lungs admit two pulmonary veins and one pulmonary artery through the hilum. The bronchi differ in their mode of subdivision between the left and right lungs [1]. The right bronchus gives off a branch to the superior lobe about 2.5 cm from the bifurcation of the trachea. As this branch arises above the level of the pulmonary artery it is named as the eparterial bronchus. Other division come off below the artery and thus termed hyparterial bronchus. The left bronchus passes below the level of pulmonary artery before it divides and so all its branches are hyparterial.
Understanding of the normal anatomy is very essential foundation of the surgical knowledge. Though the fissures and the lobar pattern of the lungs are studied in a few populations, the hilar anatomy of the lungs has been overlooked [3]. Variant anatomy may lead to misinterpretation of a radiograph or computed tomography (CT) scan [4]. Certain radiological findings can mislead the diagnosis as in the cases of extra lobes, as it may misinterpret as lung lesions. In the presence of extra lobes, the CT scan shows a significant increase in the size of mediastinum around the trachea [5]. The accessory fissure might alter usual pattern of lung collapse in patients with endobronchial lesion, and pose difficulty in diagnosing the extent of lesion. Normally pneumonia will be restricted to the lobes affected by it, but in patients with incomplete fissures, it may spread to adjacent lobes through the parenchymal continuation [6, 7].
In the current study, we focused on the morphological variations of the lungs in the south Indian cadaveric samples.
Materials and Methods
One hundred thirty-eight isolated, adult formalin fixed cadaveric lungs preserved in the dissection hall were observed for the study. The lungs belonged to the adult age group between 45-75 years. No gender difference of the lungs was made in this study. Only those lungs which were covered all over by pleura except at the hilum were used in the study. If any part of the lung was cut off during its removal, such lung was excluded from the study. Out of 138 lungs, 65 were right lungs, and 73 were left lungs. Following parameters were noted in the current study: number of fissures and lobes, shape of lungs and their lobes, and variations in the hilar structures.
Results
Right lungs
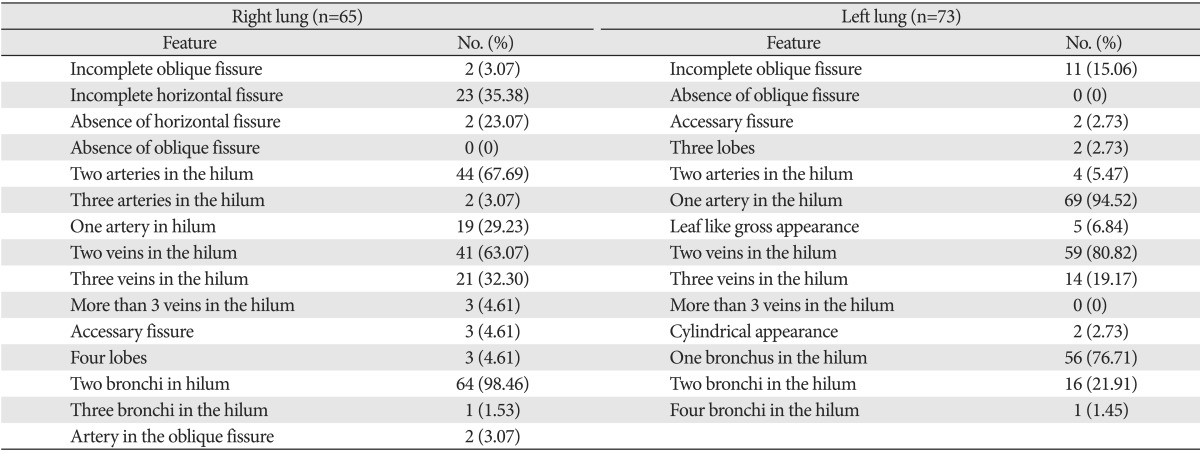
Among the 65 right lungs, 2 lungs (3.07%) showed absence and 23 (35.38%) showed incomplete horizontal fissures. Three right lungs (4.61%) showed 3 fissures and 4 lobes. Two (3.07%) lungs had 3 arteries, 44 (67.69%) had 2 arteries and 19 (29.23%) had 1 artery in the hilum. Forty-one lungs (63.07%) had 2 veins in the hilum; 21 (32.30%) had 3 veins in the hilum; and 3 (4.61%) had more than 3 veins in the hilum. Sixty-four of them (98.46%) showed 2 bronchi in the hilum, and only one of them (1.53%) showed 3 bronchi in the hilum. Two of the lungs (3.07%) had an artery passing across the oblique fissure.
Left lungs
Among the 73 left lungs, 11 (15.06%) showed incomplete oblique fissure. Two of them (2.73%) showed 2 fissures and 3 lobes. Four of them (5.47%) showed 2 arteries and 69 of them (94.52%) had only 1 artery in the hilum. Fifty-nine (80.82%) of the lungs had 2 veins in the hilum and 14 (19.17%) had three veins in the hilum. Sixteen of them (21.91%) had 2 bronchi and 56 (76.71%) had only one bronchus in the hilum. Five lungs (6.84%) had cylindrical and 2 lungs (2.73%) had leaf like external appearance.
Photographs of the specimens with some of the major variations can be seen in Figs. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10.
Fig. 1.

Left lung with three lobes and two fissures.
Fig. 2.
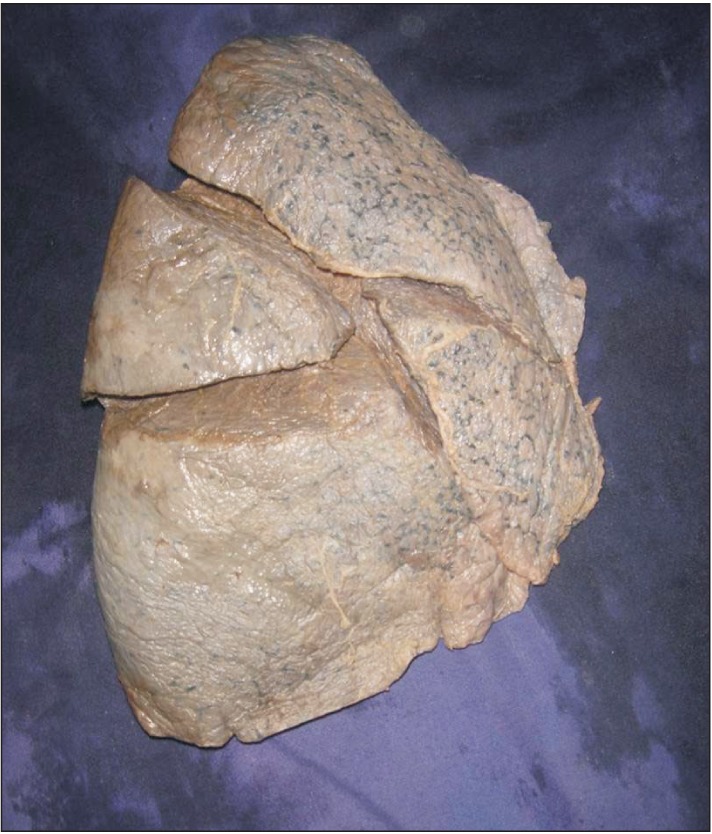
Right lung with four lobes and three fissures.
Fig. 3.
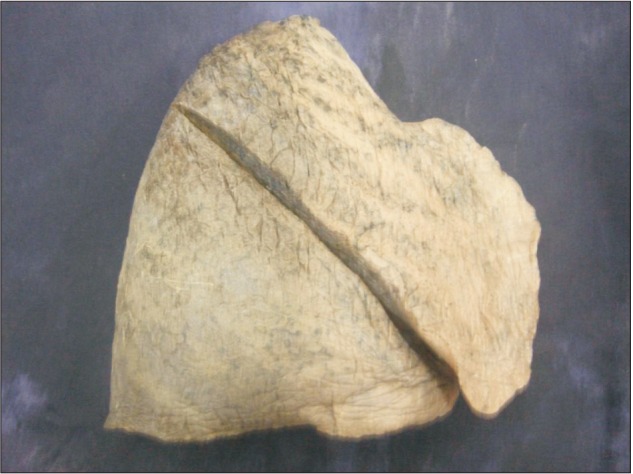
Right lung with two lobes and one fissure.
Fig. 4.
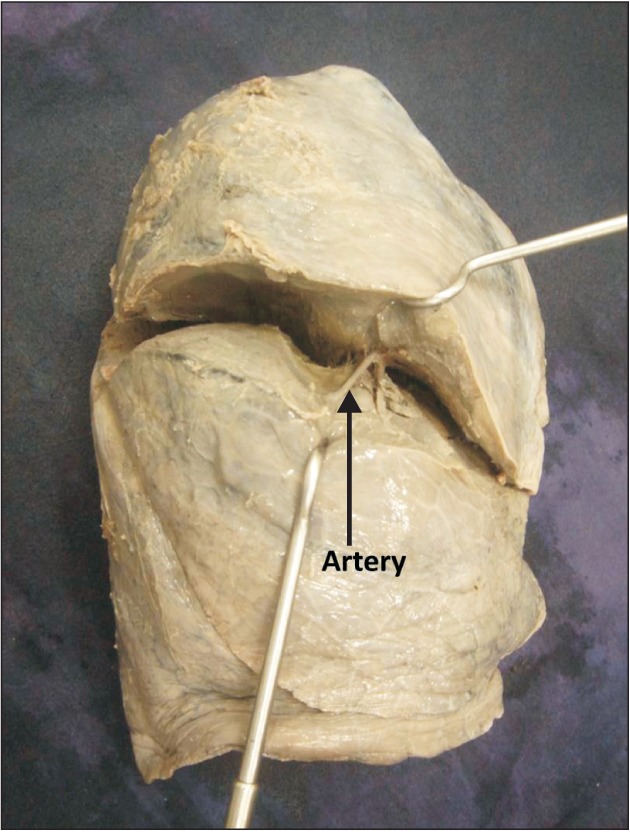
Visible artery in the fissure.
Fig. 5.
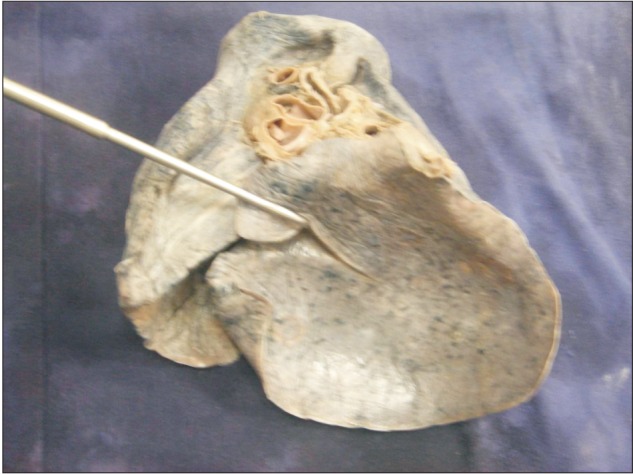
Oblique fissure extending on to the base.
Fig. 6.

Incomplete oblique fissure.
Fig. 7.
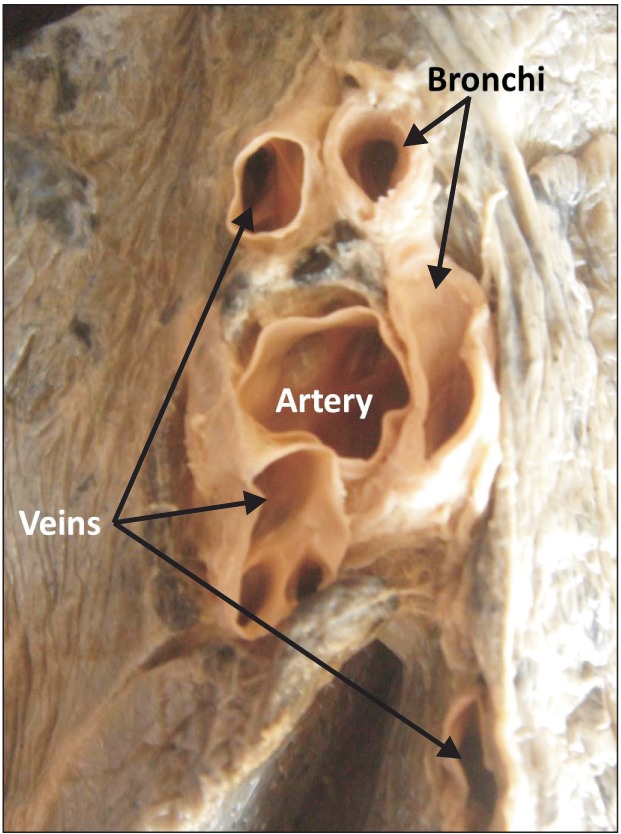
Hilum of the right lung with three veins, one artery, and two bronchi.
Fig. 8.
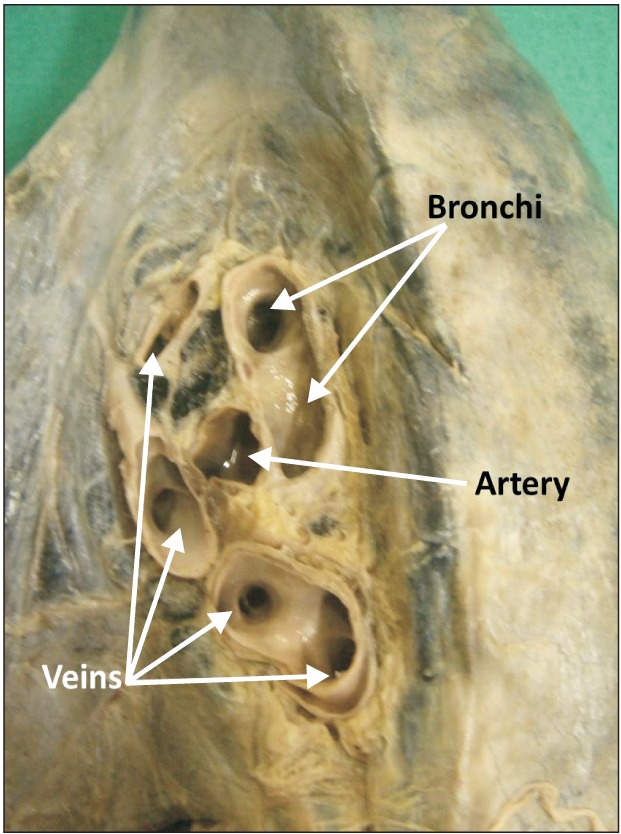
Hilum of the right lung with four veins, two bronchi, and one artery.
Fig. 9.
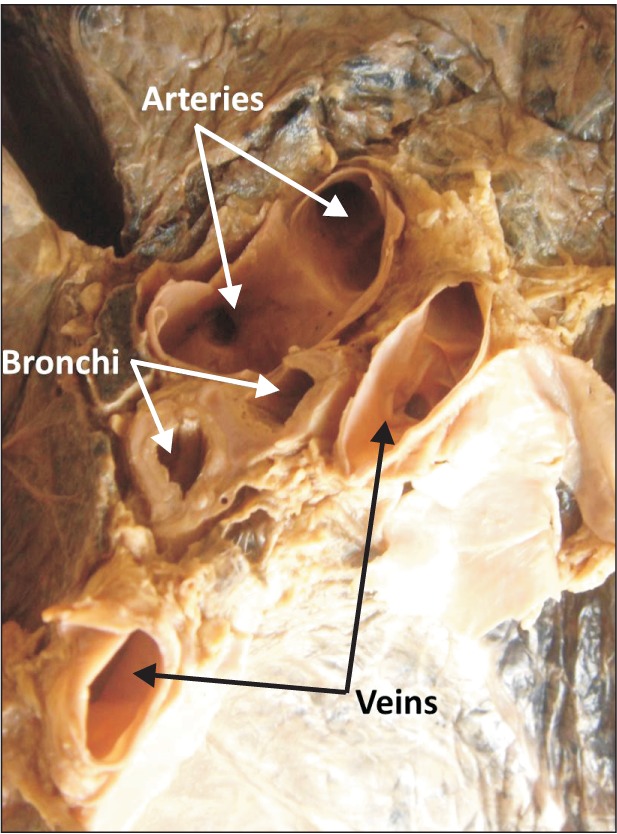
Hilum of the left lung with two veins, two arteries, and two bronchi.
Fig. 10.
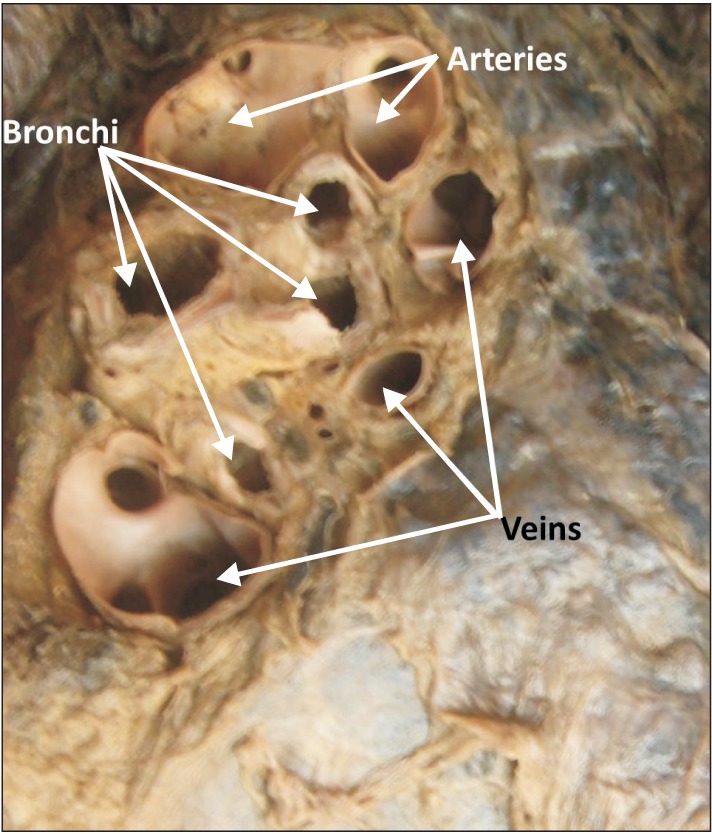
Hilum of the left lung with three veins, two arteries, and four bronchi.
Percentage statistics have been given in Table 1.
Table 1.
The variations seen in the right and left lungs
Discussion
Cadavers are the best means to study the variant anatomy of any organ. Various researchers have noted and reported the anomalous anatomy of the lungs in human cadavers [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14]. During development of the lungs numerous bronchopulmonary buds are formed and later they fuse completely except at the sites of fissure formation. This results in the formation of lobes and fissures. Incomplete fissure formation could be due to partial obliteration of these fissures [8]. Accessory fissure could be the result of non-fusion of spaces between the bronchopulmonary buds which normally are obliterated. If there is any factor affecting the fusion in the developmental stage, there will be variations in the formation of lobes and fissures of the lung [4]. In our literature survery, we could find a few reports on variations of the fissures of the lungs [15, 16, 17, 18]. Knowledge of development of minor lung segments and pulmonary veins is also useful clinically [19]. When compared to the previous studies, we found a higher incidence of incomplete horizontal fissures and two arteries in the hilum of right lung [9, 10, 11]. We did not find even a single case of absence of oblique fissure which was reported by earlier researchers as 2% for right and 5% for left lung respectively [12]. Fifteen point zero three percentage of left lungs in the current study showed incomplete oblique fissure, whereas the previous studies report the incidence of this variation as 12%-47% [11]
Accessary lobes and fissures can be misinterpreted on X-rays and CT scans. They can also be confused with certain clinical conditions such as linear atelectasis, pleural scars or walls of bullae [3, 11, 14]. In our study 3 such cases of right lungs with extra horizontal fissures were present, with which the lungs were divided into 4 lobes instead of 3 lobes. Two of the left lungs also showed an accessary fissure, which divided them into 3 lobes instead of 2 lobes. Some of the previous studies also report the presence of accessory lobes of lungs [20, 21, 22]. It is very rare to find an artery in the fissure of a lung. Awareness of this might be useful for surgeons to avoid excessive bleeding during pulmonary lobectomy. The shape anomaly such as cylindrical or leaf like appearance may be of congenital cause and when exists, might cause confusions in radiological diagnosis.
In conclusion, knowledge of the fissures and lobes of the lungs are important to plan various surgical procedures to avoid post-operative complications like air leakage. It can also help to explain various radiological appearances of lobar anatomy of the lungs and the position of the interlobar fluid. The results of the present study and their comparison with the previous studies shows that a variety of variations can occur at the hilar structures as well as the shape, fissures and lobes of the lungs in humans. Variations in the number and pattern of hilar structures in both human lungs have not been studied in detail by earlier researchers, thus this study add a database for the same. Prior anatomical knowledge and suspicion for probable variations may be crucial for clinicians, surgeons and radiologists.
References
- 1.Shah P, Johnson D, Standring S. Thorax. In: Standring S, editor. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 39th ed. Edinburgh: Churchill Livingstone; 2005. pp. 1068–1069. [Google Scholar]
- 2.Rosse C, Gaddum-Rosse P. Hollinshead's textbook of anatomy. Philadelphia: Lipincott Williams & Wilkins; 1997. pp. 441–461. [Google Scholar]
- 3.Brahmbhatt RJ, Chauhan KB, Bansal M, Brahmbhatt JN. Cadaveric study of azygous lobe of lung. Int J Basic Appl Med Sci. 2013;3:30–33. [Google Scholar]
- 4.Meenakshi S, Manjunath KY, Balasubramanyam V. Morphological variations of the lung fissures and lobes. Indian J Chest Dis Allied Sci. 2004;46:179–182. [PubMed] [Google Scholar]
- 5.Speckman JM, Gamsu G, Webb WR. Alterations in CT mediastinal anatomy produced by an azygos lobe. AJR Am J Roentgenol. 1981;137:47–50. doi: 10.2214/ajr.137.1.47. [DOI] [PubMed] [Google Scholar]
- 6.Aldur MM, Denk CC, Celik HH, Tasçioglu AB. An accessory fissure in the lower lobe of the right lung. Morphologie. 1997;81:5–7. [PubMed] [Google Scholar]
- 7.Tarver RD. How common are incomplete pulmonary fissures, and what is their clinical significance? AJR Am J Roentgenol. 1995;164:761. doi: 10.2214/ajr.164.3.7863909. [DOI] [PubMed] [Google Scholar]
- 8.Larsen WJ. Human embryology. New York: Churchill Livingstone; 1993. pp. 111–130. [Google Scholar]
- 9.Polaczek M, Religioni J, Orłowski T. Anatomic variations of pulmonary vessels relevant with regard to lung tissue resections: literature review and personal experiences. Kardiochir Torakochirurgia Pol. 2013;10:232–238. [Google Scholar]
- 10.Prakash, Bhardwaj AK, Shashirekha M, Suma HY, Krishna GG, Singh G. Lung morphology: a cadaver study in Indian population. Ital J Anat Embryol. 2010;115:235–240. [PubMed] [Google Scholar]
- 11.Nene AR, Gajendra KS, Sarma MV. Lung lobes and fissures: a morphological study. Anatomy. 2011;5:30–38. [Google Scholar]
- 12.Ghosh E, Basu R, Dhur A, Roy A, Roy H, Biswas A. Variations of fissures and lobes in human lungs: a multicentric cadaveric study from West Bengal, India. Int J Anat Radiol Surg. 2013;2:5–8. [Google Scholar]
- 13.Sharma G, Vijayvergiya T. Anatomical variations in lobar pattern of the lungs: anatomical study and clinical significance. J Pharm Biomed Sci. 2013;26:301–303. [Google Scholar]
- 14.Mayuri J, Pradeep P, Vasudha N, Aparna T, Smita M. Anomalous lobar pattern of right lung: a case report. J Res Med Den Sci. 2013;1:80–81. [Google Scholar]
- 15.Berkmen T, Berkmen YM, Austin JH. Accessory fissures of the upper lobe of the left lung: CT and plain film appearance. AJR Am J Roentgenol. 1994;162:1287–1293. doi: 10.2214/ajr.162.6.8191982. [DOI] [PubMed] [Google Scholar]
- 16.Frija J, Schmit P, Katz M, Vadrot D, Laval-Jeantet M. Computed tomography of the pulmonary fissures: normal anatomy. J Comput Assist Tomogr. 1982;6:1069–1074. doi: 10.1097/00004728-198212000-00004. [DOI] [PubMed] [Google Scholar]
- 17.Medlar EM. Variations in interlobar fissures. Am J Roentgenol Radium Ther. 1947;57:723–725. [PubMed] [Google Scholar]
- 18.Otsuji H, Uchida H, Maeda M, Iwasaki S, Yoshiya K, Hatakeyama M, Ohishi H, Iioka S, Kitamura S, Narita N. Incomplete interlobar fissures: bronchovascular analysis with CT. Radiology. 1993;187:541–546. doi: 10.1148/radiology.187.2.8475304. [DOI] [PubMed] [Google Scholar]
- 19.Abe S, Yamamoto M, Noguchi T, Yoshimoto T, Kinoshita H, Matsunaga S, Murakami G, Rodríguez-Vázquez JF. Fetal development of the minor lung segment. Anat Cell Biol. 2014;47:12–17. doi: 10.5115/acb.2014.47.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Speckman JM, Gamsu G, Webb WR. Alterations in CT mediastinal anatomy produced by an azygos lobe. AJR Am J Roentgenol. 1981;137:47–50. doi: 10.2214/ajr.137.1.47. [DOI] [PubMed] [Google Scholar]
- 21.Aldur MM, Denk CC, Celik HH, Tasçioglu AB. An accessory fissure in the lower lobe of the right lung. Morphologie. 1997;81:5–7. [PubMed] [Google Scholar]
- 22.Esomonu UG, Taura MG, Modibbo MH, Egwu AO. Variation in the lobar pattern of the right and left lungs: A case report. Australas Med J. 2013;6:511–514. doi: 10.4066/AMJ.2013.1856. [DOI] [PMC free article] [PubMed] [Google Scholar]