

Abstract
Background
Retaining patients with HIV infection in care is still a major challenge in sub- Saharan Africa, particularly in the Democratic Republic of Congo (DRC) where the antiretroviral treatment (ART) coverage is low. Monitoring retention is an important tool for evaluating the quality of care.
Methods and Findings
A review of medical records of HIV -infected children was performed in three health facilities in the DRC: the Amo-Congo Health center, the Monkole Clinic in Kinshasa, and the HEAL Africa Clinic in Goma. Medical records of 720 children were included. Kaplan Meier curves were constructed with the probability of retention at 6 months, 1 year, 2 years and 3 years. Retention rates were: 88.2% (95% CI: 85.1%–90.8%) at 6 months; 85% (95% CI: 81.5%–87.6%) at one year; 79.4% (95%CI: 75.5%–82.8%) at two years and 74.7% (95% CI: 70.5%–78.5%) at 3 years. The retention varied across study sites: 88.2%, 66.6% and 92.5% at 6 months; 84%, 59% and 90% at 12 months and 75.7%, 56.3% and 85.8% at 24 months respectively for Amo-Congo/Kasavubu, Monkole facility and HEAL Africa. After multivariable Cox regression four variables remained independently associated with attrition: study site, CD4 cell count <350 cells/µL, children younger than 2 years and children whose caregivers were member of an independent church.
Conclusions
Attrition remains a challenge for pediatric HIV positive patients in ART programs in DRC. In addition, the low coverage of pediatric treatment exacerbates the situation of pediatric HIV/AIDS.
Introduction
According to the UNAIDS 2013 report, worldwide 3.3 million children under 15 years were living with HIV in 2012. Over 90% of these infected children live in sub-Saharan Africa [1]. It was estimated that during the same year 260,000 new HIV infections occurred among children, most of them as a result of mother-to-child transmission of HIV (MTCT) [1]. Mother-to-child transmission rates declined overall from an estimated 26% in 2009 to 17% in 2012, and coverage of prevention of mother -to-child transmission (PMTCT) services increased to 65%. The number of children younger than 15 years receiving ART increased to 34% [1]. However, these summary estimates comprise enormous disparities between the different countries [1]. In 2012, the coverage of PMTCT services in the Democratic Republic of Congo (DRC) was estimated to be only 13%, and only 9% of children younger than 15 years in need of ART (according to the WHO 2010 guidelines) were receiving ART [2], [3].
Evidence shows that early administration of ART in HIV-infected infants reduces mortality and HIV progression by 75% [4]. However, achieving this depends on several factors, including the early diagnosis of HIV infection, adequate quality of antiretroviral (ARV) drug prescription, good support for children on ART and maintaining/retaining these HIV-infected children in care and ART programs [4], [5].
Patients' retention in care programs remains a major challenge in sub- Saharan Africa [6]–[10]. It is also one of the key indicators to assess the success of ART programs [6].
Retention rates among children vary from 71 to 95% at one year, and between 62 and 93% at 2 years in sub-Saharan Africa [5].
To maximize retention in ART programs, a number of factors need to be considered: structural factors such as transportation, availability and accessibility of services, service providers' attitude, caregiver's HIV status and religious and other beliefs (traditional healers), and patient-related factors [11], [12].
The objective of this study was to determine retention rates of HIV-infected children on ART in three different programs and sites in the DRC, and to assess risk factors for attrition. Based on the study findings, we propose recommendations to improve retention in pediatric HIV care and treatment programs.
Methods
Study Sites
Three facilities, known to offer care for HIV infected children and with a sufficient number of patients were asked and agreed to participate in the study. Two of these facilities are located in Kinshasa, the capital of the DRC (an Amo-Congo health facility and the Centre Hospitalier Monkole). The third facility (HEAL Africa) is located in Goma, the capital city in the North Kivu province ( Fig. 1 ). Amo-Congo is a Congolese non-governmental organization (NGO) that began in 1993 with providing support for orphans and vulnerable children in Kinshasa. Over the years this NGO expanded its activities to several provinces and included voluntary counseling and testing, and provision of HIV care to adults and children. In 2005 Amo-Congo started, with financial support from Global Fund for AIDS Tuberculosis and Malaria (GFATM) with the provision of ART in their Ambulatory Treatment Centers (ATCs), which are standalone clinics that offer counseling and testing, and HIV care. This study was conducted at the ATC in Kasa-vubu in Kinshasa.
Figure 1. Map of the Democratic Republic of Congo with provincial HIV prevalence.

The “Centre Hospitalier Monkole”, the Monkole Hospital, is a private health hospital (55 beds), in the Mount Ngafula I health zone in Kinshasa which started its activities in 1991. Their HIV unit started activities in 2005 with financial support from GFATM through the United Nations Development Programme (UNDP), and organizes HIV activities such as HIV prevention activities, ART and management of opportunistic infections. Both the Amo-Congo and Monkole health facility serve an urban population.
HEAL Africa Hospital was started in 1998 and is located in Goma/North- Kivu, and serves as a center of excellence for the province. It has 155 beds and works with 4 services/departments including surgery, internal medicine, pediatrics and obstetrics and gynecology. The HIV/AIDS pediatric care service of this facility is called AIDS Children Program (CAP), and was integrated into HEAL Africa hospital in 2005 (with financial support from UNICEF, Global Strategies and the Clinton Foundation). This facility serves populations from peri-rural and rural areas, and supports community organization in the rural area.
Study type and inclusion criteria
From October 2012 to August 2013, we conducted a retrospective cohort study of HIV-infected children on ART at these three health facilities in the DRC.
Children older than 6 months and younger than 15 years at the moment of data collection who had initiated ART at least three months prior to data collection were included in the study.
Data collection
We conducted a retrospective chart review of 720 medical charts. In each of the three research sites a random sample of medical charts was selected from a sampling frame that consisted of all children ever started on ART at that site between September 2007 and May 2012. The sampling frame was prepared by the site supervisor; the list of the medical files to be selected was generated by the data analyst using a computerized random number generator (‘sample’ function in Stata). Randomly selected children that were not eligible for the study were replaced by the next child in the sampling frame. Only one child per family was included in the study (the first child from the family on the list).
A specifically designed study form was used for data abstraction, which was carried out by a team of two nurses. All the members of the study team were trained in ethics (for confidentiality issues) and data abstraction.
Data analysis and sample size
A random sample of 250 ART-treated children in each site was needed to allow the estimation of the retention rate to be measured with a precision of 5%, assuming the retention rate was at least 80%. In all three study sites, patients received ARV medication according to the WHO 2010 guidelines [3]. Once on ART, HIV-positive children were required to come to the clinic every three months. The child or the caregiver/guardian had to go to the pharmacy every month to collect the ARV drugs. A child or caregiver visiting the clinic within the three months preceding the data collection was considered to be retained in the program.
Attrition was defined as death or loss to follow-up. Lost to follow up stands for a person under treatment and missing the scheduled visits beyond 90 days [13].
Multivariable Cox regression was used to assess the association between retention and other variables in the models. The following baseline variables were assessed as potential risk factors for attrition: age, gender, clinical stage, CD4 count at ART start, presence of opportunistic infection, hemoglobin, weight (z-score weight-for-age), height (z-score height-for-age) and education level as children's characteristics; age, education level, gender, religion, profession, civil status and relation with the child as caregivers' characteristics. Variables with p-value ≤0.10 during univariable analysis were considered for inclusion in the multivariable model. Z-scores for weight-for-age and height-for-age were generated using the 2006 WHO growth standards and the zscore06 module in Stata (http://www.ifpri.org/staffprofile/jefleroy).
The complex model was reduced by stepwise backwards elimination approach. Study site was included in the model as a fixed effect. All associations were tested using likelihood-ratio tests.
For variables with less than 10% missing values conditional imputation was used and for variables with at least 10% missing data the missing indicator method (in which a separate category is generated for patients with data missing for a certain predictor). As HEAL Africa Hospital had the highest number of children in care, this site was considered as the reference site. Epi infoTM 7.0.9.34 was used to enter data from all the sites by a trained data manager in Kinshasa. The data analysis was conducted using Epi info and Stata 11.
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of the Kinshasa School of Public Health at the University of Kinshasa. All study members were trained in human subject research and good clinical practices.
Due to the nature of the study it was not possible and feasible to obtain informed consent from the patients whose medical charts were abstracted for the study. Data were extracted from routine records, and were analyzed anonymously.
Results
The number of HIV infected children under ART did not reach 250 as was reported by the Amo-Congo and Monkole facilities. Therefore in total only 720 medical files of children on ART were available at the three study sites. Applying the inclusion criteria, 198 patient files were excluded: 77 patients were above 15 years at the moment of data collection, in 58 files the date of ART initiation was missing and 63 patients started ART within 3 months prior to data collection. After this process, 522 patient files were selected and included for the analysis. The details regarding patient flow are presented in Fig. 2 .
Figure 2. Study flow of participants in three different HIV treatment centers in the Democratic Republic of Congo.

Children's characteristics (Table 1)
Table 1. Children's characteristics in three different programs and sites in the Democratic Republic of Congo.
| Children's characteristics | Amo-Congo Kinshasa | Monkole Kinshasa | HEAL Africa Goma | Total |
| Total, n (%) | 147 (28.16) | 61(11.69) | 314(60.15) | 522(100.0) |
| Age (years), n (%) | ||||
| ≤2 | 47 (31.9) | 34 (55.7) | 106 (33.8) | 187 (35.8) |
| >2- more | 100 (68.1) | 27 (44.3) | 208 (66.2) | 335 (64.2) |
| Sex, n (%) | ||||
| Male | 76 (51.8) | 30 (49.2) | 160 (51.0) | 266 (51.0) |
| Female | 71 (48.2) | 31 (50. 8) | 154 (49.0) | 256 (49.0) |
| Education, n (%) | ||||
| Not yet eligible | 47 (31.9) | 34 (55.8) | 252 (80.2) | 333 (63.8) |
| Kindergarden | 14 (9.5) | 3 (4.9) | 4 (1.3) | 21 (4.0) |
| Primary | 72 (48.9) | 18 (29.5) | 56 (17.8) | 146 (27.9) |
| Secondary | 2 (1.4) | 0 (0.0) | 2 (0.7) | 4(0.7) |
| Missing | 12(8.3) | 6(9.8) | 0(0.0) | 18(3.5) |
| Weight-for-age z-score, n (%) | ||||
| <−2 SD | 19(12.9) | 25(41.0) | 83(26.4) | 127(24.3) |
| ≥−2 SD | 85(57.8) | 18(29.5) | 122(38.9) | 225(43.1) |
| Missing | 43(29.3) | 18(29.5) | 109(34.7) | 170(32.6) |
| Height-for-age z-score, n (%) | ||||
| <−2 SD | 10(6.8) | 5(8.2) | 76(24.2) | 91(17.4) |
| ≥−2 SD | 38(25.9) | 5(8.2) | 109(34.7) | 152(29.1) |
| Missing | 99(67.3) | 51(83.6) | 129(41.1) | 279(53.5) |
| Clinical stage, n (%) * | ||||
| WHO I | 21 (14.3) | 5 (8.2) | 1 (0.3) | 27 (5.2) |
| WHOII | 55 (37.4) | 17 (27.9) | 4 (1.3) | 76 (14.5) |
| WHO III | 64 (43.5) | 36 (59.0) | 306 (97.5) | 406 (77.8) |
| WHO IV | 7 (4.8) | 3 (4.9) | 3 (0.9) | 13 (2.5) |
| Drug regimen, n (%) | ||||
| AZT/3TC/NVP | 84 (57.1) | 49 (80.3) | 207 (65.9) | 340 (65.1) |
| 3TC/D4T/NVP | 36 (24.5) | 9 (14.7) | 92 (29.3) | 137 (26.2) |
| Other | 27 (18.3) | 3 (4.9) | 15 (4.8) | 45 (8.7) |
| CD4 cell count * (cells/µL), n (%) | ||||
| 0–200 | 49 (33.3) | 25 (40.9) | 120 (38.3) | 194 (37.1) |
| >200–350 | 24 (16.3) | 7 (11.5) | 52 (16.5) | 83 (15.9) |
| >350-more | 27 (18.5) | 7 (11.5) | 89 (28.4) | 123 (23.6) |
| Missing | 47(31.9) | 22(36.1) | 53(16.8) | 122(23.4) |
| Cotrimoxazole, n (%) | ||||
| No | 2 (1.4) | 33 (54.1) | 12 (3.8) | 47 (9.0) |
| Yes | 145 (98.6) | 28 (45.9) | 302 (96.2) | 475 (91.0) |
*At the start of antiretroviral treatment.
From 2007 to 20012, 522 HIV positive children were included in the analysis. The mean age of the children was 4.7 years (standard deviation [SD]: 3.3); 80% were in WHO clinical stage 3 or 4 at the start of ART. The first line ART regimen provided to 65% of the children was Zidovudine + Lamivudine + Nevirapine (AZT/3TC/NVP). The proportion of children who did not yet attend school was 43%; 27% attended primary school.
Care givers' characteristics (Table 2)
Table 2. Characteristics of the child's caregiver in three different programs and sites in the Democratic Republic of Congo.
| Caregivers' characteristics | Amo-Congo Kinshasa | Monkole Kinshasa | HEAL Africa Goma | Total |
| Total, n (%) | 147 (28.16) | 61(11.69) | 314(60.15) | 522 (100.0) |
| Type of Caregiver, n (%) | ||||
| Mother | 43 (29.3) | 20 (32.8) | 152 (48.4) | 215 (41.2) |
| Father | 31 (21.1) | 11 (18.0) | 50 (15.9) | 92 (17.6) |
| Grandparent | 9 (6.1) | 3 (4.9) | 22 (7.1) | 34 (6.5) |
| Brother/sister | 29 (19.7) | 15 (24.6) | 47 (14.1) | 91 (17.5) |
| Other | 35 (23.8) | 12 (19.7) | 43 (13.7) | 90 (17.2) |
| Age (years), n (%) | ||||
| >15–35 | 32 (21.8) | 11 (18.6) | 115 (36.6) | 158 (30.4) |
| >35–45 | 46 (31.3) | 21 (35.6) | 92 (29.3) | 159 (30.6) |
| >45 | 63 (42.8) | 20 (33.9) | 86 (27.4) | 169 (32.5) |
| Missing | 6(4.1) | 7(11.9) | 21(6.7) | 34(6.5) |
| Sex, n (%) | ||||
| Female | 91 (61.9) | 33 (54.1) | 230 (73.3) | 354 (67.8) |
| Male | 56 (38.1) | 28 (45.9) | 84 (26.7) | 168 (32.2) |
| Profession, n (%) | ||||
| Housewife | 48 (32.7) | 15 (28.8) | 123 (39.2) | 186 (35.6) |
| Student | 10 (6.8) | 4 (7.6) | 27 (8.6) | 41 (7.9) |
| Employee | 35 (23.8) | 16 (26.2 | 60 (19.1) | 111 (21.3) |
| Trader | 46 (31.3) | 17 (27.8) | 88 (28.1) | 151 (28.9) |
| Missing | 8(5.4) | 9(14.8) | 16(5.1) | 33(6.3) |
| Religion, n (%) | ||||
| Catholic | 44 (29.9) | 14 (22.9) | 109 (34.7) | 167 (32.0) |
| Protestant | 11 (7.5) | 14 (22.9) | 102 (32.5) | 127 (24.3) |
| Independent | 65 (44.2) | 20 (32.9) | 55 (17.5) | 140 (26.8) |
| Other | 22 (15.0) | 8 (13.1) | 36 (11.5) | 66 (12.6) |
| Missing | 5(3.4) | 5(8.2) | 12(3.8) | 22(4.2) |
| Education, n (%) | ||||
| Primary and less | 26 (17.7) | 12 (19.7) | 128 (40.8) | 166 (31.8) |
| Secondary | 83 (56.5) | 27 (44.2) | 132 (42.1) | 242 (46.4) |
| Higher education | 35 (23.8) | 10 (16.4) | 39 (12.3) | 84 (16.1) |
| Missing | 3(2.0) | 12(19.7) | 15(4.8) | 30(5.7) |
| Marital status, n (%) | ||||
| Not maried | 25 (17.0) | 8 (13.1) | 32 (10.1) | 65 (12.5) |
| Married (Poly and monogamous) | 53 (36.1) | 15 (24.5) | 150 (47.8) | 218 (41.8) |
| Widowed | 37 (25.2) | 11 (18.0) | 80 (25.5) | 128 (24.5) |
| Missing | 32(21.7) | 27(44.3) | 52(16.6) | 111(21.3) |
In 51%, the children's caregivers were direct parents (either mother of father). Among the caregivers, 51% were male and the mean age of the caregivers was 42 years (SD: 13). Those who had a formal job represented 53% of the caregivers, 66% had at least the secondary school education. 42% of the caregivers were married, 62% belonged either to the catholic or protestant church, and 37% to the independent church.
Retention
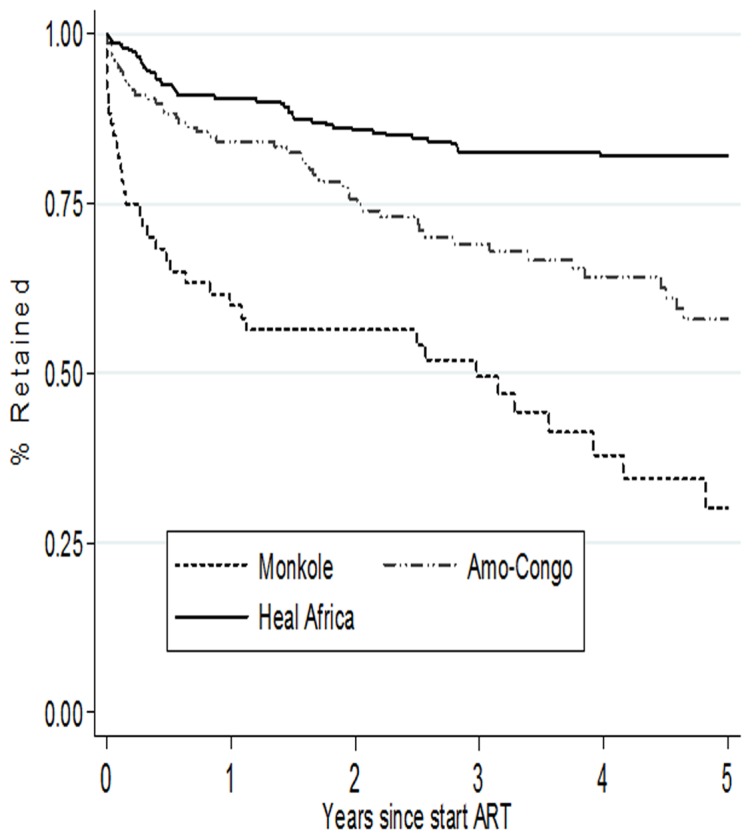
The overall retention probabilities are presented in Fig. 3 . Overall retention rates were 88% (95% CI [95% confidence interval]: 85%–91%) at 6 months, 85% (95% CI: 81%–87%) at one year, 79% (95%CI: 75%–83%) at two years and 74% (95% CI: 70%–78%) at 3 years. The overall median time in the ART program was 3 years (IQR [inter quartile range]: 1.3–5.0), with site-specific median times of 2.5 years (IQR: 1.3–4.6) at AMO-Congo Kasavubu, 1.5 years (IQR: 1.2–3.5) at the Monkole facility and 3.5 (IQR: 1.5–5.0) years at the HEAL Africa facility in Goma. Site-specific retention rates were 88%, 67% and 92% at 6 months; 84%, 59% and 90% at 12 months and 76%, 56% and 86% at 24 months, respectively for Amo-Congo/Kasa-vubu, Monkole facility and HEAL Africa ( Fig. 4 ).
Figure 3. Overall retention rates for children on ART in three different HIV treatment centers in the Democratic Republic of Congo.
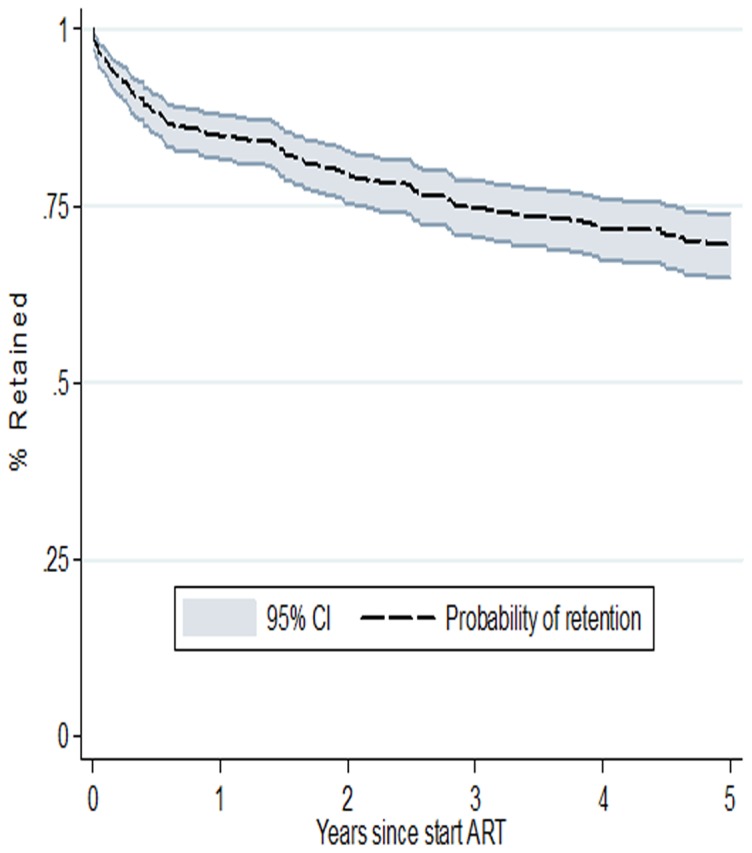
Figure 4. Retention rates for children on ART by facility in three different programs and sites in the Democratic Republic of Congo.
Out of the 522 HIV infected children, 109 (20.8%) were lost from the ART program: 22 (20%) had died, 87 (80%) were lost to follow-up and, 4 (4%) were transferred to other ART programs.
Risk factors for attrition (Table 3)
Table 3. Risk factors for attrition in three different programs and sites in the Democratic Republic of Congo.
| Riskfactor | Participants N(%) | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | P-value | |
| Study site, n (%) | HEAL Africa | 314 (60.5) | 1 | 1 | <0.001 |
| Amo-Congo | 147 (27.9) | 2.29 (1.54–3.42) | 2.15 (1.35–3.40) | ||
| Monkole | 61 (11.6) | 5.14 (3.32–7.94) | 4.77 (2.90–7.85) | ||
| Initial age of Child (years), n (%) | >2 years | 334(66.2) | 1 | 1 | <0.001 |
| ≤2 years | 170(33.8) | 2.41(1.71–3.40) | 2.16 (1.48–3.16) | ||
| Initial CD4 cell count of child (cells/µL), n (%) | ≥350-more | 121 (23.4) | 1 | 1 | 0.039 |
| >200–<350 | 83 (15.9) | 3.12 (1.55–6.27) | 2.87 (1.36–6.07) | ||
| >0–200 | 193 (37.2) | 3.29 (1.77–6.11) | 2.70 (1.40–5.21) | ||
| Missing | 122 (23.5) | 3.80 (1.98–7.29) | 2.24 (1.11–4.51) | ||
| Education of child, n (%) | Primary or less | 138 (27.6) | 1 | / | / |
| Secondary school | 149 (29.7) | 2.74 (1.56–4.82) | |||
| Not yet eligible | 214 (42.7) | 2.90 (1.70–4.95) | |||
| Religion of caregiver, n (%) | Catholic | 166 (33.4) | 1 | 1 | 0.003 |
| Protestant | 144 (29.0) | 0.78 (0.44–1.36) | 1.90 (0.51–1.59) | ||
| Independant/other | 187 (37.6) | 2.07 (1.34–3.21) | 1.86 (1.19–2.90) | ||
HR: Hazard Ratio; CI: Confidence Interval;
P-value from Cox-regression model adjusted for all factors in final model, including site as a fixed effect.
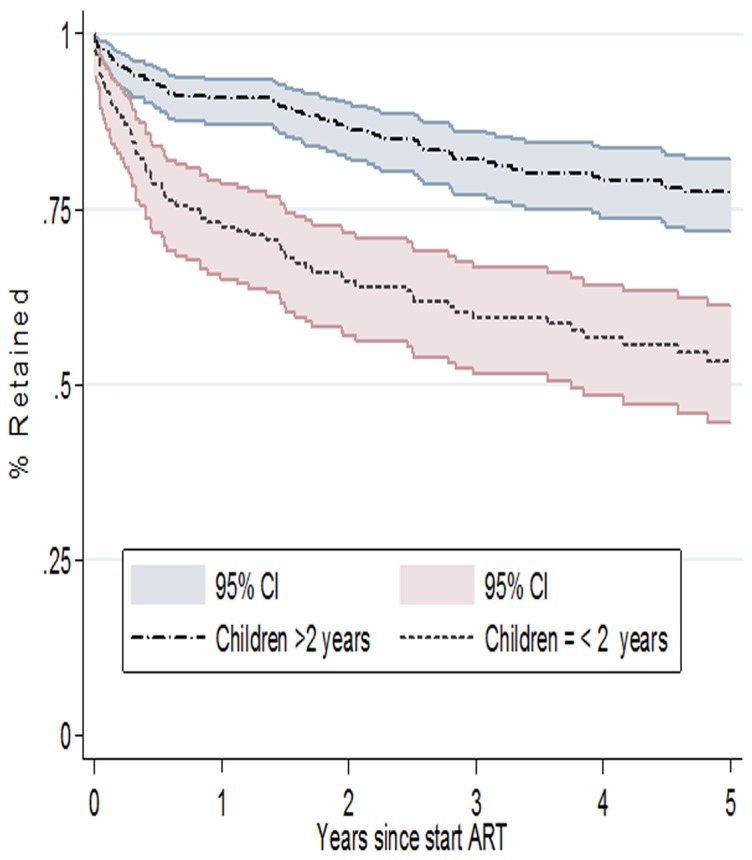
The following variables were considered in the multivariable model: study site, the child's age, CD4 count, education level and uptake of Cotrimoxazole; type, gender and religion of caregiver. In the final model four variables remained associated with children's attrition from ART programs: study site, the child's age and CD4 count at ART start and religion of the caregiver. Patients enrolled in the Monkole facility (aHR: 4.77, 95% CI: 2.90–7.85) were likely to experience higher risk of attrition compared to the patients enrolled in care at the HEAL Africa hospital. Children ≤2 years age (aHR: 2.16, 95% CI: 1.48–3.16) experienced higher attrition compared to older children ( Fig. 5 ). Children with a CD4 cell count ≤200/µL (aHR: 2.70, 95% CI: 1.40–5.21) and those with a CD4 cell count between >200–<350/µL (aHR: 2.87, 95% CI: 1.36–6.07) were likely to experience higher risk of attrition compared to children with CD4 count ≥350/µL.
Figure 5. Retention rates for children on ART by age categories in three different programs and sites in the Democratic Republic of Congo.
Children whose caregivers were affiliated to the independent church (aHR: 1.86; 95% CI: 1.19–2.90) were more likely to experience attrition compared to those whose caregivers were affiliated to the catholic and protestant church.
Risk factors for loss to follow up and death (Table 4)
Table 4. Risk factors associated with LTFU and death among children in three study sites.
| Loss to follow up | Reported deaths | ||||
| Riskfactor | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | |
| Study site | HEAL Africa | 1 | 1 | 1 | 1 |
| Amo-Congo | 2.28 (1.49–3.50) | 2.06(1.27–3.36) | 9.52(4.15–21.83) | 7.22(2.92–17.84) | |
| Monkole | 4.31 (2.69–6.92) | 3.41(1.98–5.86) | 12.63(5.14–30.99) | 7.49(2.84–19.77) | |
| Initial age of Child (years) | >2 years | 1 | 1 | 1 | 1 |
| ≤2 years | 2.20(1.52–3.18) | 1.89(1.25–2.85) | 1.80(1.03–3.14) | 2.78(1.19–6.51) | |
| Initial CD4 cell count of child (cells/µL) | ≥350-more | 1 | 1 | 1 | / |
| >200–<350 | 3.81 (1.74–8.33) | 3.80 (1.64–8.77) | 1.47 (0.55–3.92) | ||
| >0–200 | 3.70 (1.82–7.51) | 3.13 (1.46–6.68) | 1.14 (0.48–2.69) | ||
| Missing | 4.29 (2.04–9.00) | 2.83 (1.27–6.29) | 2.64 (1.15–6.04) | ||
| Education of child | Primary or less | 1 | / | 1 | / |
| Secondary school | 2.47 (1.39–4.38) | 4.37 (1.64–11.61) | |||
| Not yet eligible | 2.31 (1.34–3.97) | 2.48 (0.92–6.66) | |||
| Religion of caregiver | Catholic | 1 | 1 | 1 | / |
| Protestant | 0.85 (0.46–1.54) | 1.02 (0.55–1.88) | 0.33 (0.10–1.01) | ||
| Independant/other | 2.10 (1.31–3.37) | 1.79 (1.10–2.90) | 2.02 (1.04–3.90) | ||
HR: Hazard Ratio; CI: Confidence Interval.
In multivariate analysis, four variables remained associated with loss to follow up: study site, the child's age and CD4 count at ART start and religion of the caregiver. Children enrolled in the Monkole facility (aHR: 3.41, 95% CI: 1.98–5.86) were likely to experience higher risk of loss to follow up compared to the patients enrolled in care at the HEAL Africa hospital. Children ≤2 years age (aHR: 1.89, 95% CI: 1.25–2.85.) experienced higher risk of loss to follow up compared to older children. Children with a CD4 cell count ≤200/µL (aHR: 3.13, 95% CI: 1.46–6.68) and those with a CD4 cell count between >200–<350/µL (aHR: 3.80, 95% CI: 1.64–8.77) were likely to experience higher risk of loss to follow up compared to children with CD4 count ≥350/µL. Children whose caregivers were affiliated to the independent church (aHR: 1.79; 95% CI: 1.10–2.90) were more likely to experience attrition compared to those whose caregivers were affiliated to the catholic and protestant church.
Two variables remained associated with death: study site and the child's age. Patients enrolled in the Monkole facility (aHR: 7.49, 95% CI: 2.84–19.77) were likely to experience higher risk of death compared to the patients enrolled in care at the HEAL Africa hospital. Children ≤2 years age (aHR: 2.78 95% CI: 1.19–6.51) experienced higher risk of death compared to older children.
Discussion
Retention rates varied widely across the study facilities: between 93% and 67% at 6 months; 90% and 59% at 12 months and 86% to 56% at 24 months. The highest retention rate was found in Goma, which can be described as a mixture of a peri-rural and rural setting. The community support organization active in this rural area may have played a role in retaining ART patients as was also observed in other settings [14]. Our findings corroborate also with other studies that report higher retention rates in rural areas compared to urban areas [4], [15]–[20].Retention rates among children on ART in our study were high compared to another study conducted among adults in the DRC, where retention rates of 81%, 75%, 65% and 57%, respectively at 6 months, one year, two years and three years were found [21]. Somehow these better results among children highlight the low quality of care level for patients with HIV infection in the DRC in general.
In the DRC the coverage in HIV care services is amongst the lowest in the world. PMTCT interventions remain the entry point for pediatric care treatment in DRC, but PMTCT coverage is very low (13%) [2]. Also coverage of family planning in DRC is very low, only 6% of women of childbearing age have access to family planning [22]. The ART coverage in adults is less than 20%, with huge disparities across the country and alarming figures in the rural areas. ART coverage is even more dramatic in children: 9% in 2012 [2]. As a consequence of this low coverage of family planning, PMTCT and ART the number of HIV infected children is increasing. Advocacy and increased commitment from government and international organizations is needed to increase services for family planning, PMTCT and ART coverage [2]. HIV services should be implemented in all health facilities allowing nurses to provide the ARV.
Retention rates were significantly higher in HIV specialized facilities like HEAL Africa and Amo-Congo/Kasa-vubu compared to Monkole which is a general hospital and which offers a packet of integrated health services. In the DRC, most of public facilities are general health facilities that do not pay special attention to a complex health issue such as HIV. Poor quality of health services is associated with high attrition rates [23].
Patients with a CD4 cell count <350/µL were more likely to experience attrition compared to those with higher CD4 counts. We should be cautious about the interpretation of these findings. More than 10% of data on CD4 cell count was missing and the CD4 cell count percentage (to determine the eligibility for ART in children) was not available for most of the children. We speculate that children with a CD4 cell count <350/µL were at higher risk of mortality and lost to follow up as reported in other studies where attrition was associated with advanced disease stage [4]–[6].
Younger children (≤2 years) were also more likely to experience attrition. These findings corroborate with others studies conducted in developing countries [5]–[6], [24]. The children whose caregivers were affiliated to the independent churches were more likely to experience attrition compared to those whose caregivers were affiliated to the catholic church or protestant church. These independent churches often promise miracle healing. Therefore patients affiliated to these churches are more at risk for attrition. These findings corroborate with others studies where independent church members appear to have lower uptake of health services [25], [26]. Given the impact of religion on people in the DRC, collaboration with religious leaders could help to convince caregivers about the importance not to stop the ART. Specific training sessions for religious leaders about this topic should be considered.
Reinforcement of community interventions such as the “Mentor Mothers (MM)” and “Community ART groups (CAG)” is critical [27], [28]. MM approach consists of using HIV positive peer mothers to support, educate, and empower other pregnant women, new mothers and their partners [27]. CAG are peer support groups that provide psychosocial support to HIV-positive women, men, and children in their own community [28]. Each CAG comprises between 6 to 12 members and keeps linkage with the health facility in order to receive ARVs and clinical support as needed. CAG members organize themselves to meet and provide peer support without involvement of the health providers. These support groups also play a key role in defaulter tracing and encouraging attendance at health facility appointments. The CAG approach helps to reduce the frequency of drugs' collection from the pharmacy and therefore the cost for traveling to the clinic. One patient (volunteer) travels to the clinic to collect ARVs for other members of the CAG. The CAG strategy was shown to improve significantly patients' retention and adherence [14], [28].
Our study has several limitations. As in most retrospective studies, some important information was not available in the medical charts e.g. weight, height and CD4%. Moreover, we were unable to assess the influence of the caregivers HIV status because this information was only available in a few of them. Other studies have shown that an HIV positive status of the caregiver may have a negative impact on the children's retention [28].
Our study was performed in three non-public facilities. We speculate that the support provided to these facilities had a positive impact on the quality of data and services. Results may be worse in public facilities in the DRC where the support is scarce.
In conclusion, attrition remains a challenge for pediatric HIV positive patients in ART programs in the DRC. In addition, the low coverage of pediatric treatment and the delayed start of ART exacerbate the situation of pediatric HIV/AIDS. Whilst moving towards the new 2013 WHO guidelines [29], serious commitment, in terms of government's political will and more support from the international donors, is needed to increase access to ART and retention in ART programs.
Acknowledgments
We thank the General Direction of Cooperation and Development (GDCD) from the Belgium Technical Cooperation for the funding tis study. We recognize the significant contribution of Kinshasa School of Public Health (KSPH) and the Institute of Tropical Medicine at Antwerp.
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and its Supporting Information files.
Funding Statement
This study was carried out with funding provided by the General Direction of Cooperation and Development (GDCD) from the Belgium Technical Cooperation. GDCD didn't have any role in study design, data collection and analysis, manuscript development or decision to publish.
References
- 1.UNAIDS (2013) Global report: UNAIDS report on the global AIDS epidemic 2013. Available at http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf. Accessed 2014 Jan 31.
- 2.UNAIDS (2013) Progress report on the Global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive. Available at http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2013/20130625_progress_global_plan_en.pdf. Accessed 2014 Feb 3.
- 3.WHO (2010) Antiretroviral drugs for treating pregnant women and preventing HIV infection s in infant s, Recommendations for a public health approach. World Health Organization website. Available at: http://whqlibdoc.who.int/publications/2010/9789241599818_eng.pdf. Accessed 2014 Feb 3. [PubMed]
- 4. Violari A, Cotton MF, Gibb DM, Babiker AG, Steyn J, et al. (2008) Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med. 359(21):2233–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. McNairy ML, Lamb MR, Carter RJ, Fayorsey R, Tene G, et al. (2013) Retention of HIV-infected children on antiretroviral treatment in HIV care and treatment programs in Kenya, Mozambique, Rwanda, and Tanzania. J Acquir Immune Defic Syndr. 62(3):e70–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. KIDS-ART-LINC (2008) Low risk of death, but substantial program attrition, in pediatric HIV treatment cohorts in Sub-Saharan Africa. J Acquir Immune Defic Syndr. 49:523–531. [DOI] [PubMed] [Google Scholar]
- 7. Davies MA, Keiser O, Technau K, Eley B, Rabie H, et al. (2009) Outcomes of the South African National Antiretroviral Treatment Programme for children: the IeDEA Southern Africa collaboration. S Afr Med J. 99:730–737. [PMC free article] [PubMed] [Google Scholar]
- 8. Sauvageot D, Schaefer M, Olson D, Pujades-Rodriguez M, O'Brien DP, et al. (2010) Antiretroviral therapy outcomes in resource-limited settings for HIV-infected children, 5 years of age. Pediatrics. 125:e1039–e1047. [DOI] [PubMed] [Google Scholar]
- 9. Ekouevi DK, Azondekon A, Dicko F, Malateste K, Toure P, et al. (2011) 12-month mortality and loss to-program in antiretroviral-treated children: the IeDEA pediatric West African Database to evaluate AIDS (pWADA), 2000–2008. BMC Public Health. 11:519 Available: http://www.biomedcentral.com/1471-2458/11/519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ellis J, Molyneux EM (2007) Experience of anti-retroviral treatment for HIV infected children in Malawi: the 1st 12 months. Ann Trop Paediatr. 27:261–267. [DOI] [PubMed] [Google Scholar]
- 11. Fenner L, Brinkhof MW, Keiser O, Weigel R, Cornell M, et al. (2010) Early mortality and loss tofollow-up in HIV-infected children starting antiretroviral therapy in Southern Africa. J Acquir Immune Defic Syndr. 54:524–532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Sutcliffe GC1, van Dijk JH, Bolton C, Persaud D, Moss WJ (2008) Effectiveness of antiretroviral therapy among HIV-infected children in sub-Saharan Africa. Lancet Infect Dis. 8:477–489. [DOI] [PubMed] [Google Scholar]
- 13. Rosen S, Fox MP, Gill CJ (2007) Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLoS Med 4:e298 Available at: http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.0040298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Grimwood A, Fatti G, Mothibi E, Malahlela M, Shea J, et al. (2012) Community adherence support improves programme retention in children on antiretroviral treatment: a multicentre cohort study in South Africa. J Int AIDS Soc. 15(2):17381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Fassinou P, Elenga N, Rouet F, Laguide R, Kouakoussui KA, et al. (2004) Highly active antiretroviral therapies among HIV-1-infected children in Abidjan, Cote d'Ivoire. AIDS. 18:1905–1913. [DOI] [PubMed] [Google Scholar]
- 16. Eley B, Nuttall J, Davies MA, Smith L, Cowburn C, et al. (2004) Initial experience of a public sector antiretroviral treatment programme for HIV-infected children and their infected parents. South African medical journal. 94:643–646. [PubMed] [Google Scholar]
- 17. Diack MB, Signate Sy H, Gueye DN, Ba A, Sylla A, et al. (2005) Epidemiological and clinical aspects of paediatric HIV infections in Albert-Royer Paediatric Hospital (Dakar, Senegal) Arch Pediatr. 12:404–409. [DOI] [PubMed] [Google Scholar]
- 18. Cowburn CA, Hatherill M, Eley B, Nuttall J, Hussey G, et al. (2006) Short-term mortality and implementation of antiretroviral treatment for critically ill HIV-infected children in a developing country. Arch Dis Child. 2007;92 (3):234–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. van Kooten Niekerk NK, Knies MM, Howard J, Rabie H, Zeier M, et al. (2006) The first 5 years of the family clinic for HIV at Tygerberg Hospital: family demographics, survival of children and early impact of antiretroviral therapy. Journal of tropical pediatrics. 52:3–11. [DOI] [PubMed] [Google Scholar]
- 20. O'Brien DP, Sauvageot D, Zachariah R, Humblet P (2006) In resource-limited settings good early outcomes can be achieved in children using adult fixed-dose combination antiretroviral therapy. AIDS. 20:1955–1960. [DOI] [PubMed] [Google Scholar]
- 21.Koole O, Kalenga L, Kiumbu M, Menten J, Ryder RW, et al. (2012) Retention in NGO supported antiretroviral program in the Democratic Republic of Congo, PLoS One, e40971. Available at: http://www.plosone.org/article/info%3Adoi%2F101371%2Fjournal.pone.0040971. [DOI] [PMC free article] [PubMed]
- 22.Ministères du plan et de la Santé, République Démocratique du Congo et Calverton: Macro International (2007) Enquête démographique et de santé 2007. Minister of Heath –Democratic Republic of Congo website. http://www.who.int/bulletin/volumes/86/12/07-049908/en/. Accessed February 3, 2014.
- 23.Forster M, Bailey C, Brinkhof MW, Graber C, Boulle A, et al. (2008) Electronic medical record systems, data quality and loss to follow-up: survey of antiretroviral therapy programmes in resource-limited settings. Bull World Health Organ. 86(12): 939–947. Available at: http://www.who.int/bulletin/volumes/86/12/07-049908/en/. [DOI] [PMC free article] [PubMed]
- 24.Baveewo S, Ssali F, Karamagi C, Kalyango JN, Judith A, et al. (2011) Validation of World Health Organisation HIV/AIDS Clinical Staging in Predicting Initiation of Antiretroviral Therapy and Clinical Predictors of Low CD4 Cell Count in Uganda. PLoS One. 6(5): e19089. Available at: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0019089. [DOI] [PMC free article] [PubMed]
- 25. Ditekemena J, Matendo R, Koole O, Colebunders R, Kashamuka M, et al. (2011) Male partner voluntary counselling and testing associated with the antenatal services in Kinshasa, Democratic Republic of Congo: a randomized controlled trial. Int J STD AIDS. 22(3):165–70. [DOI] [PubMed] [Google Scholar]
- 26. Musheke M, Bond V, Merten S (2012) Individual and contextual factors influencing patient attrition from antiretroviral therapy care in an urban community of Lusaka, Zambia. J Int AIDS Soc. 15 Suppl 1 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Shroufi A, Mafara E, Saint-Sauveur JF, Taziwa F, Viñoles MC (2013) Mother to Mother (M2M) peer support for women in Prevention of Mother to Child Transmission (PMTCT) programmes: a qualitative study. PLoS One. 2013. June 5;8(6):e64717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Decroo T, Telfer B, Biot M, Maïkéré J, Dezembro S, et al. (2011) Distribution of antiretroviral treatment through self-forming groups of patients in Tete Province, Mozambique. J Acquir Immune Defic Syndr. 2011. February 1;56(2):e39–44. [DOI] [PubMed] [Google Scholar]
- 29.WHO (2013) Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. World Health Organization website: Available at: http://www.who.int/hiv/pub/guidelines/arv2013/en/. Accessed February 3, 2014. [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and its Supporting Information files.