

Abstract
Background:
Presence of plaque may be the culprit for dental caries, gingivitis, periodontal problems, and halitosis. Many mechanical aids are practiced worldwide to remove or control plaque, including tooth brushes, dental floss, mouth rinses, and dentifrices. The objective of this clinical study was to investigate the effectiveness of herbal toothpaste (Dabur Red) in controlling plaque and gingivitis, as compared to conventional (non-herbal) dentifrice (Pepsodent).
Materials and Methods:
In this study, 30 subjects aged 35–43 years with established gingivitis and at least 20 natural teeth, and having a probing depth <3 mm were investigated. After the washout period, plaque and gingival index (PI and GI, respectively) scores were assessed at days 0 and 30. Differences between groups were compared with Mann–Whitney U test and the mean scores of PI and GI by Wilcoxon test. Statistical difference between the weights of dentifrices tubes on days 0 and 30 was evaluated by Student's t-test.
Results:
At the end of 30 days of the study, there was statistically significant difference between both the groups for plaque and gingival scores.
Conclusion:
After 30 days of trial, both test and control groups showed effective reduction of plaque and gingivitis, which was statistically significant. No adverse reactions to dentifrices products were observed during the trial. It was concluded that herbal dentifrice was as effective as non-herbal dentifrices in the control of plaque and gingivitis.
Keywords: Anti-plaque, gingivitis, herbal, non-herbal, toothpaste
INTRODUCTION
Dental plaque deposit on teeth is a concern for both cosmetic and its pathogenic nature. Presence of plaque may be the culprit for dental caries, gingivitis, periodontal problems, and halitosis. Many mechanical aids are used worldwide to remove or control plaque, including tooth brushes, dental floss, mouth rinses, and dentifrices.[1] Mechanical plaque removal is one of the most accepted methods of controlling plaque and gingivitis. But it is expected that less than one-third of the population can effectively perform mechanical plaque removal. Several chemical preventive agents have beneficial effects in the control of plaque and to reduce or prevent oral disease. Hence, various chemical formulations were tried in dentifrices.[2] Chemicals, mainly triclosan and chlorhexidine, have been added in mouth rinses and dentifrices to prevent plaque and gingivitis. But some of these substances show undesirable side effects such as tooth staining and altered taste.[1,3] This had led to paying increased attention on using natural ingredients in herbal dentifrices. Herbal ingredients have several benefits; chamomile has anti-inflammatory effect, echinacea has immune stimulatory property, sage and rhatany have anti-hemorrhagic properties, myrrh is a natural antiseptic, and peppermint oil has analgesic, antiseptic, and anti-inflammatory properties.[4] There are limited studies available regarding the efficacy of herbal dentifrices; hence, the present study was undertaken to assess their plaque and gingival preventive action.
MATERIALS AND METHODS
In this clinical trial, 30 subjects in the age range of 35–43 years (15 females and 15 males) were recruited from OPD, Department of Periodontics, Humnabad Dental College, Humnabad, Karnataka. Ethical approval was obtained from the institutional review board and written consent from the participant subjects (control and test groups). Subjects who met the following inclusion criteria were included in this retrospective study: Having a minimum of 20 teeth, good general health, presence of established gingivitis, willing to give a written informed consent, willing to follow the schedule and has not participated in a similar investigation in past 4 weeks. The exclusion criteria were: Presence of advanced periodontitis, probing depth >4 mm, subjects under antimicrobial therapy, smokers, pregnant women, using orthodontic appliances, having used mouth rinse containing chemical agents in previous 3 months, and having a history of allergy to toothpastes. Control group consisted of those who were healthy, having no history of known sensitivity or oral mucosal tissue reaction to toothpaste, not having used any herbal dentifrices/mouth wash, and not under any medication for past 3 months.
The study was designed as a randomized, double-blinded, parallel-arm, controlled clinical trial. The participants were randomly divided using the random number table. The random allocation sequence was generated and was concealed from the main examiner (FO) until the dentifrices were assigned to the participants. The main examiner was responsible for enrolling the subjects and assessing the study variables. Blinding and allocation concealment were controlled by the independent pharmacy “Formula e Acao,” which distributed the toothpastes in plain tubes identified as group A and group B tubes. All investigators and the study subjects were unaware of the contents of each tube. The pharmacy revealed the content of each tube only after the experimental period was over.
Two days after the initial washout period with professional prophylaxis, each subject was distributed new medium bristle tooth brush and toothpastes. The test group used commercial herbal dentifrice Dabur Red (Dabur Laboratory, Udham Sing Nagar, Uttarakhand, India) containing the following: Pudina satva (menthol 50–55%, methyl acetate, menthone), Tomar beej and laung ka tel (70–90% eugenol 50–55%, 50% sesquiterpenes). The control group used Pepsodent (Unilever Dental Research™ Reg Haridwar, India) containing- calcium carbonate, water, sorbitol, sodium lauryl sulfate, hydrated silica, flavor, magnesium aluminum silicate, sodium monofluorophosphate, potassium nitrate, benzyl alcohol, sodium silicate, cellulose gum, triclosan, and sodium saccharin.
All participants were instructed to brush their teeth for 3 min 2 times a day for 30 days with Bass method using the given toothpaste and brush. Verbal and written instructions were given to all subjects about the use of dentifrices. The plaque index (PI) (on the buccal/labial and lingual surfaces) and gingival bleeding index (GI) of all teeth were recorded by a single trained examiner on days 0 and 30. For PI, the values of two sites were averaged for each participant. The amount of plaque was scored using two-tone disclosing solution and Turesky's (1970) modification of the Quigley, Hein (1962) index (PI), and Gingival index scoring (GI) by Silness and Loe (1963). Oral cavity was examined for any adverse reaction on hard and soft tissues by the same examiner. Dentifrices tubes were collected from all subjects after completion of the study and weighed before and after trial to find the quantity used.
Statistical analysis was done using SPSS 16.0 Windows software (IBM Corporation, Chicago). Statistical difference between the weights of dentifrices tubes on days 0 and 30 was evaluated by Student's t-test. Statistical differences between the control and test groups on days 0 and 30 were evaluated by Mann–Whitney U test and the mean scores of PI and GI by Wilcoxon test.
RESULTS
All 30 study subjects (15 males and 15 females) completed the 30-day study period. At baseline, there was no significant difference between both the groups for plaque and gingivitis. At baseline, the PI median score for herbal and non-herbal groups was 2.61 and 2.47, respectively. Baseline values for gingivitis in herbal and non-herbal groups were 1.19 and 1.14, respectively. At 30 days, both test and control groups showed 18.8% and 17.4% reduction of plaque and 27.3% and 38.4% reduction of gingivitis, respectively. Reduction of plaque and gingivitis from 0 to 30 days was statistically significant in both the groups [Tables 1 and 2]. Statistically, there was no significant difference between the groups. No adverse reactions to dentifrices products were observed during the trial. There was a significant reduction of dentifrice tube weights between days 0 and 30 in both the groups (P < 0.001), which showed that volunteers actually used the toothpastes [Table 3].
Table 1.
Comparison of PI between groups or inter-group comparison
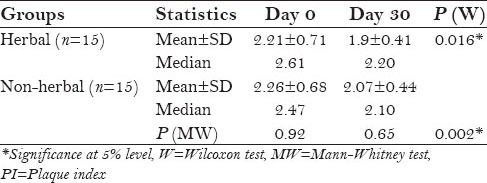
Table 2.
Comparison of GI between groups or inter-group comparison
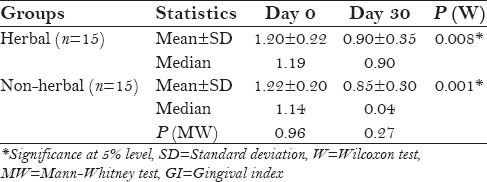
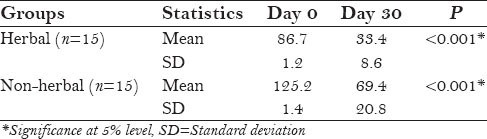
Table 3.
Comparison of weights of dentifrices tubes (in grams) between groups or inter-group comparison using Student's t-test
DISCUSSION
Dental plaque is the main culprit for gingival inflammation and dental caries. Chronic gingival inflammation may lead to tissue destruction, and if left untreated, may progress into the more destructive stages of periodontitis.[1] Hence, plaque and gingivitis control helps in maintenance of healthy oral cavity. This can be achieved effectively by mechanical plaque control using tooth brush and medicated toothpastes.
The primary purpose of this study was to evaluate the efficacy of herbal dentifrice in the control of plaque and gingivitis. Hence, the content of the products was not our main focus; rather it was the preventive effect of dentifrices. All 30 study subjects (15 males and 15 females) completed the 30-day study period. At baseline, there was no significant difference between both the groups for plaque and gingivitis. At baseline, the PI median score for herbal and non-herbal groups was 2.61 and 2.47, respectively.
At 30 days, both test and control groups showed 18.8% and 17.4% reduction of plaque, respectively. Reduction of plaque was statistically significant in both the groups at baseline and at 30 days (for herbal group P = 0.016 and for non-herbal group = 0.002) [Table 1]. Herbal dentifrice was as effective as the conventional one in plaque reduction. This is in accordance with the reports of Ozaki et al. (19.9% and 18.3% reduction, respectively, for herbal and non-herbal dentifrices) and Sushma et al. (60.36% and 59.89% reduction, respectively, for herbal and non-herbal dentifrices).[5,6] Similar results were observed by de Oliveira et al. with the herbal product Aloe vera in plaque reduction.[3] Several other studies proved the effectiveness of herbal dentifrices in plaque control, compared to the conventional one.[2,4,7,8,9]
At 30 days, both test and control groups showed 27.3% and 38.4% reduction of gingivitis, respectively. Statistically, there was no significant difference between the groups. Reduction of gingivitis was statistically significant in both the groups from baseline to 30 days (for herbal 0.008 and for non-herbal <0.001) [Table 2]. We found herbal dentifrices to be as effective as the non-herbal ones in the reduction of gingivitis. This is in agreement with the report by Ozaki et al. (28.4% and 36.3% reduction, respectively).[5] Also, it is similar to the findings of George et al. and Mateu et al.[2,8] de Oliveira et al. found slightly lower efficacy of herbal product on gingivitis and gingival bleeding compared to the conventional one, whereas Sushma et al. and Pannuti et al. observed slightly higher gingivitis reduction with herbal products.[6,7]
No adverse reactions to dentifrices products were observed during the trial in the present study. This is in agreement with the reports by Oliveira et al. and Ozaki et al.[3,5] There was a significant reduction of dentifrice tube weights between days 0 and 30 in both the groups (P < 0.001), which shows that the volunteers had actually used the toothpastes [Table 3]. This is in accordance with the report of de Oliveira et al.[3]
Rubido et al. found in their study that medicated toothpaste use significantly reduces salivary bacterial count.[10] George et al. found no significant difference between the effects of herbal and conventional toothpastes on salivary pH values.[2] Saxena et al. found in an in vitro study that herbal dentifrices showed the maximum inhibition zone.[11]
The control group composed of fluoride and triclosan ingredients in toothpaste. Triclosan is an antimicrobial agent with well-established safety and efficacy.[4] Fluoride has anti-caries effect, but some of the constituents of the conventional toothpastes have undesirable side effects like staining and taste alterations. Hence, natural products with added benefits are advised for use.[3] Several studies have proven the anti-plaque and anti-gingival effects of herbal toothpaste, which were comparable to those of conventional toothpastes.[2,4,5,6,9]
The present study has proved that herbal dentifrices do not cause any adverse effects on the oral cavity and are effective in reduction of plaque and gingivitis, as that of fluoridated non-herbal dentifrice. Several studies have proven the medicinal values of herbal products.[2,9] Hence, medicated herbal toothpastes can be safely used to control plaque and gingivitis. Further long-term studies are required to prove their effectiveness.
Limitations of the study were as follows: The sample size was small and a clinical trial with longer duration on subjects in the age range of 18–65 may be required to prove the effectiveness of herbal dentifrice in reduction of plaque and gingivitis.
CONCLUSION
After 30 days of trial, both test and control groups showed effective reduction of plaque and gingivitis, which was statistically signi›cant. No adverse reactions to dentifrices products were observed during the trial. It can be concluded that clinically, herbal dentifrices are as effective as non-herbal (conventional) dentifrices in the control of plaque and gingivitis. Addition of chemical agents in dentifrices aids in plaque control and improves oral health.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Barnes VM, Richter R, DeVizio W. Comparision of the short-term antiplaque/antibacterial efficacy of two commercial dentifrices. J Clin Dent. 2010;21:101–4. [PubMed] [Google Scholar]
- 2.George J, Hegde S, Rajesh KS, Kumar A. The efficacy of a herbal-based toothpaste in the control of plaque and gingivitis: A clinic-biochemical study. Indian J Dent Res. 2009;20:480–2. doi: 10.4103/0970-9290.59460. [DOI] [PubMed] [Google Scholar]
- 3.de Oliveira SM, Torres TC, Pereira SL, Mota OM, Carlos MX. Effect of dentifrice containing Aloe vera on plaque and gingivitis control. A double-blind clinical study in humans. J Appl Oral Sci. 2008;16:293–6. doi: 10.1590/S1678-77572008000400012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Radafshar G, Mahboob F, Kazemnejad E. A study to assess the plaque inhibitory action of herbal-based toothpaste: A double blind controlled clinical trial. J Med Plants Res. 2010;4:1182–6. [Google Scholar]
- 5.Ozaki F, Pannuti CM, Imbronito AV, Pessotti W, Saraiva L, de Freitas NM, et al. Efficacy of a herbal tooth paste on patients with established gingivitis--a randamised controlled trial. Braz Oral Res. 2006;20:172–7. doi: 10.1590/s1806-83242006000200015. [DOI] [PubMed] [Google Scholar]
- 6.Sushma S, Nandlal B, Srilatha KT. A comparative evaluation of a commercially available herbal and non-herbal dentifrice on dental plaque and gingivitis in children- A residential school based oral health programme. J Dent Oral Hyg. 2011;3:109–13. [Google Scholar]
- 7.Pannuti CM, Mattos JP, Ranoya PN, Jesus AM, Lotufo RF, Romito GA. Clinical effect of a herbal dentifrice on the control of plaque and gingivitis: A double-blind study. Pesqui Odontol Bras. 2003;17:314–8. doi: 10.1590/s1517-74912003000400004. [DOI] [PubMed] [Google Scholar]
- 8.Mateu FA, Boneta AE, DeVizio W, Stewart B, Proskin HM. A clinical investigation of the efficacy of two dentifrices for controlling established supragingival plaque and gingivitis. J Clin Dent. 2008;19:85–94. [PubMed] [Google Scholar]
- 9.Mazumdar M, Chatterjee A, Majumdar S, Mahendra C, Patki PS. Evaluation of the safety and efficacy of complete care herbal toothpaste in controlling dental plaque, gingival bleeding and periodontal diseases. J Homeop Ayurv Med. 2013;2:1–5. [Google Scholar]
- 10.Rubido S, Fernández-Feijoo J, Limeres J, García-Caballero L, Abeleira MT, Diz P. In vivo antiplaque effect of three edible toothpastes. Med Oral Patol Oral Cir Bucal. 2014;19:e88–92. doi: 10.4317/medoral.18973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Saxena S, Prashant GM, Chandu GN. Labaroterial evaluation of antimicrobial efficacy of herbal dentifrices commercialized in India. Arch Oral Res. 2011;7:51–60. [Google Scholar]