

Abstract
Background:
In India, obesity is highly prevalent in women as compared to men. As the obesity epidemic spreads, there are growing concerns about efficient obesity management.
Aims:
To compare between circuit training (CT), treadmill (TM) walking and suryanamaskar (SN) training in weight management and physical fitness enhancement in obese females.
Settings and Designs:
Comparative controlled study conducted in a community setting.
Materials and Methods:
119 females of age between 20 and 40 years of body mass index (BMI) between 25.1 and 34.9 kg/m2. 87 participants completed the study. Group 1: CT; group 2: TM walking; group 3: Modified SN; group 4: Control. Outcome Measures: Body composition, cardio-respiratory and muscle endurance, flexibility.
Statistical Analysis:
Within-group data was analyzed with the paired t-test. P =0.05. Analysis between the groups was done using one way ANOVA test. Analysis between the groups was done using ANCOVA test controlling for baseline differences only for those variables that have significant differences at baseline. For those which do not have significant difference at baseline, RMANOVA was done at end of 8 weeks.
Results:
Reducation in mean body weight in CT group (2.2%), TM (1.7%) and SN (1.6%), (P < 0.05), BMI in all the three groups (P < 0.01), total body fat % in the CT (5%) and SN (3.7%), (P < 0.01), metabolic age with CT (2%) and TM (2%), (P = 0.001). Improvement in muscle mass in CT (4%, P = 0.009), VO2max in CT group by 17.2%, SN (14%), TM group (8%) (P < 0.05). Upper limb Muscle endurance in CT (51.3%), SN group (51.24%) and in TM group (40%), (P = 0.05), in lower limb TM (21.2%) and SN (24.5%) (P = 0.05), flexibility in SN (12.4%, P = 0.0001).
Conclusions:
All three methods were effective in weight and physical fitness management. CT and SN were more effective in improving cardio-respiratory fitness and upper limb muscle endurance while only SN was effective in improving body flexibility.
Keywords: Body composition, circuit training, exercise training, obesity, suryanamaskar
INTRODUCTION
Overweight and obesity are common health conditions and their prevalence is increasing globally. [1] In developing countries, obesity and sedentary behaviour coexists with under nutrition. [2] In India, obesity is highly prevalent in women as compared to men. [3] As the obesity epidemic spreads, there are growing concerns about efficient obesity management. Obesity comes with several causes which makes obesity management more complex. Some evidence suggests that lack of physical activity rather than caloric intake is a major determinant of obesity. [4,5]
It is the need of the moment to develop effective and comprehensive strategies which can reduce body weight and obesity related co-morbidities. [6] The current targets should be focused on improving overall physical health rather than only reducing body weight.
Physical activity and/or exercise are commonly included as components of lifestyle interventions for weight loss. There are no specific recommendation mentioned on type and intensity of exercise. Various studies using aerobic, resistance or combination of both types of exercises have shown to have health benefits.
Yoga is an ancient Indian form of physical activity which may assist in achieving recommended levels of fitness. Suryanamaskar (SN) is a part of yoga. It is a set of sequential yogic postures which are called as asanas. A review by Ross et al. [7] suggests that yoga may be equally effective or better than exercise at improving a variety of health-related outcome measures like blood glucose, blood lipids and oxidative stress. Nevertheless, there is a dearth of research in the field of SN and also not used frequently as a therapeutic exercise. [8] On the other hand, CT is a popular exercise training method addressing cardiorespiratory fitness (CRF) and muscle endurance in a shorter period of time [9,10,11] and can be used as a long term maintenance training program [12] in all age groups. [13] In addition, CT involves easily adjusted external resistance rather than fixed body weight resistance.
Walking is the most accessible and easily regulated exercise that can enhance health and CRF. The specific role of walking, the most common form of exercise among women, [14] has been addressed only minimally. Obese individuals expend more energy during walking as compared to nonobese. [15,16]
In the current study we compared circuit, treadmill (TM) walking and SN in weight management and associated physical fitness. For example, clinical observations suggest that TM training may improve cardiovascular endurance and reduce body fat, circuit training (CT) is commonly used for strength training, and SN training which is a traditional form of physical activity may improve flexibility. Nevertheless there is a dearth of data on role of SN in weight management. In various fitness and weight management centres, ‘aerobics’ involving high impact ballistic movements are incorporated. These forms of exercise are not suitable for obese females, especially those associated with musculoskeletal problems like arthritis and osteoporotic ones.
Thus, this study tries to search for an optimal approach in between these three types of training for management of obesity and enhancement of physical fitness parameters like cardio respiratory fitness, muscle endurance and flexibility.
SUBJECTS AND METHODS
The study was approved by the Institutional Ethical Committee and was conducted in accordance with the guidelines of Helsinki Declaration prior to beginning.
Subjects
Written informed consent was taken from all the 119 subjects prior to enrolment in the study. 103 women from various fitness and wellness centres in the city were recruited. These were of body mass index (BMI) between 25.1 and 34.9 kg/m2 (i.e. overweight and grade I obesity), aged 20-40 years were recruited from December 2011 to September 2013. Participants who did not participate in any form of physical activity over the last 3 months were selected. Females with asymptomatic musculoskeletal or cardiovascular condition were included. Women with acute trauma or uncontrolled metabolic or systemic disease, any orthopedic contraindication to physical activity, pregnant or lactating women or females on any anti-hypertensive, lipid lowering medications or any illness that would limit the ability to perform the necessary exercises were excluded from the study. All participants continued their present level of lifestyle and dietary habits.
Study design
This was an 8 week randomized controlled study design. All the participants were screened through Par Q and YOU questionnaire and AHA/ACSM Health/Fitness facility pre participation screening questionnaire (Modified from American College of Sports Medicine Position Stand and American Heart Association) prior to the onset of study.
The participants were randomly allocated to 4 groups as they were recruited with n in group 1, n + 1 in group 2, n + 2 in group 3, and n + 3 in group 4, n + 4 in group 1 again and so on.
Sample Size Formula = (Z-value)2 * P * (1- p)/c2
Where,
Z = Z value (e.g. 1.96 for 95% confidence level) P = percentage picking a choice, expressed as decimal (0.5 used for sample size needed) c = confidence interval, expressed as decimal. So your values for each of the groups are: Z-Value: 1.96 (for 95% confidence level) p: 0.5, c: 0.22, Sample size: 19.84298-20 (per group).
Assessments
The outcome measures were assessed at the baseline and after 8 weeks of training. All the outcome measures were parametric type of data except, BMI (weight in kg/height in metre2) and visceral fat ratings.
Weight and body composition
These were assessed using a bioelectric impedance analyzer (Inner Scan V, Segmental Body Composition Monitor, Model BC 601, Tanita, Japan). The readings were taken while maintaining appropriate hydration of the subjects. The post training measurements were taken after 8 weeks under similar conditions, that is, same time of the day with adequate hydration.
Cardiorespiratory fitness
Estimated VO2 max was assessed using Shuttle Walk and Run Test. It consists of 12 levels with speed gradually increasing with each level. Level 1 speed was set at 2.7 km/h. As the level advances, the speed increments by 15 m/min that is, the number of laps increases by 2 laps/min and so on.
Test procedure
The participants had to walk in the initial laps and run as the speed increases at each level. It results in lesser perceived exertion because of incremental stress with each level rather than by constant-rate stress. This method was chosen as it is less stressful and safer for overweight or obese individuals. [18]
Flexibility
Flexibility is the ability to move the joint through its complete range of motion. Complete body flexibility was assessed using sit and reach test. [19]
Test procedure
A 12 inches high box with a measuring scale placed on top of the box with 9-inch mark made at the starting point of the box was used. In this study, flexibility was measured on the dominant side, that is, right lower side. The left knee was bent. The arms were extended forward with palms down over the measuring scale. The participant reaches forward four times and holds the position at the fourth reach for at least 1 s at which readings were noted. A maximum score of 12 inches can be reached. [20]
Muscle endurance
It is the muscles ability to perform for successive exertions or many repetitions. [21] Upper limb muscle endurance was assessed by a modified push up test. The number of push ups completed in 1 min was noted. The lower limb muscle endurance was assessed by 1/4th squat test. Number of squats completed within 1 min was noted. The test was stopped before 1 min if more than two push ups or squats were not performed in the correct form or if the subject encountered muscular fatigue before 1 min.
Training protocols
All participants underwent warm up and cool down for 10 min. It included slow cycling/slow walking on TM and stretching.
Exercise intensity: Participants of all three exercise groups were given the respective training until the participants reached rate of perceived exertion (RPE) of 7 on a 10 scale, that is, ‘very hard’ on the modified Borg's scale.
Group 1: CT group performed 3 sets of 10 repetitions of each of the following circuits: Push ups, pull down, knee extension on quadriceps table, leg press, resisted hip abduction/adduction, resisted back flexion/extension, hamstring curls, bicep curls. Each circuit was performed at a resistance of 40% of 1 RM. As the strength increased, new 1 RM was assessed every 2 weeks. The circuits were continued till the participant reaches score of 7 on RPE scale
Group 2: TM training group performed TM training at a speed of 4 mph with 0% grade till RPE of 7
Group 3: SN training group performed modified SN (with a chair). The participants were demonstrated the steps before starting the training. SN was performed at a speed of approximately 1 step/second. They were asked to perform as many SN till they reach RPE of 7.
It consisted of a total of 12 steps/asanas:
Step 1: Pranamasan: Stand straight. Look straight. Place the feet together. Pull in knees, thigh muscles and belly. Expand the chest. Fold hands. Palms pressed against each other to perform namaskar
Step 2: Hastauttanasan: Raise arms above head. Grow taller. Then bend back. Stretch abdomen
Step 3: Hastapadasana: Bend forward. Don’t bend knees. Go down and place your hands on the arm rests of the chair
Step 4: Ashwasanchalanasan: Take right leg back and stretch it while balancing it on the toe and keep left leg in front of your body aligned with the front legs of the chair. Keep palms straight on both sides of the arms rests of the chair and look upwards
Step 5: Parvatasan: Take back the left leg as well and keep both the feet together while raising hip from the ground and balancing on all fours (Hands on chair arm rest and feet on the floor)
Step 6: Chaturnamaskar: Slowly come down and bring your shoulders near your hands, chest sinking on the chair. Knees should not touch the ground and waist and hip slightly raised above so that they don’t touch the chair
Step 7: Bhujangasan: Lower waist and raise torso, make arms straight and balance. Feel bend of spine and stretch of abdomen
Step 8: Parvatasan: Same as position 5
Step 9: Ashwasanchalanasana: Same as position 4
Step 10: Hastapadasana: Same as position 3
Step 11: Hastauttanasan: Same as position 2
Step 12: Pranamasan: Same as position 1
Group 4: Control (CNT) group did not participate in any form of exercise training. They were asked not to involve in any form of physical activity or dietary change.
Exercise compliance and supervision
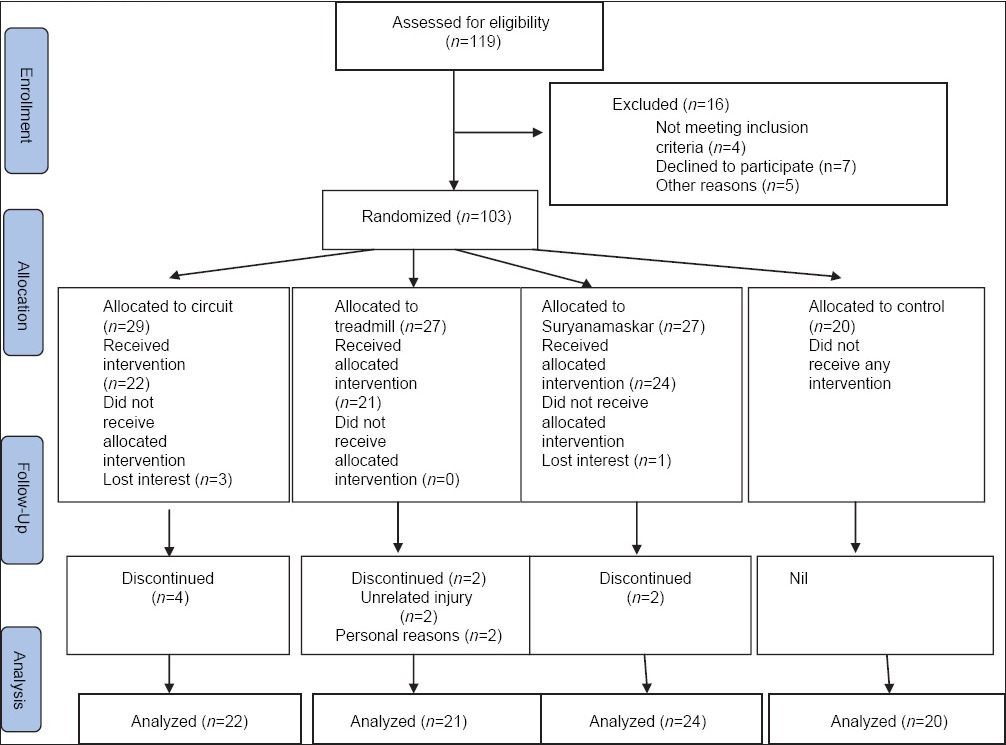
Exercise was supervised by a therapist. Compliance was considered as successfully completing >80% of exercise sessions. Noncompliant participants were considered as dropouts [Table 1].
Table 1.
Participant flowchart
Statistical analysis
All data are presented as mean ± standard deviation. Within-group data to compare the difference between pre- and post-intervention was analyzed with the paired t-test. Differences were considered statistically significant at P < 0.05. Analysis between the groups was done using ANCOVA test controlling for baseline differences only for those variables that have significant differences at baseline. For those which do not have significant difference at baseline, RMANOVA was done at end of 8 weeks. All the statistical tests were done using SPSS 12.0 for windows (Release date 4 September 2003) Standard License developed by The Apache Software foundation licensed as ‘AS-Is’ to the Physiotherapy Department, Sancheti Institute for Orthopedics and Rehabilitation, Pune, India.
RESULTS
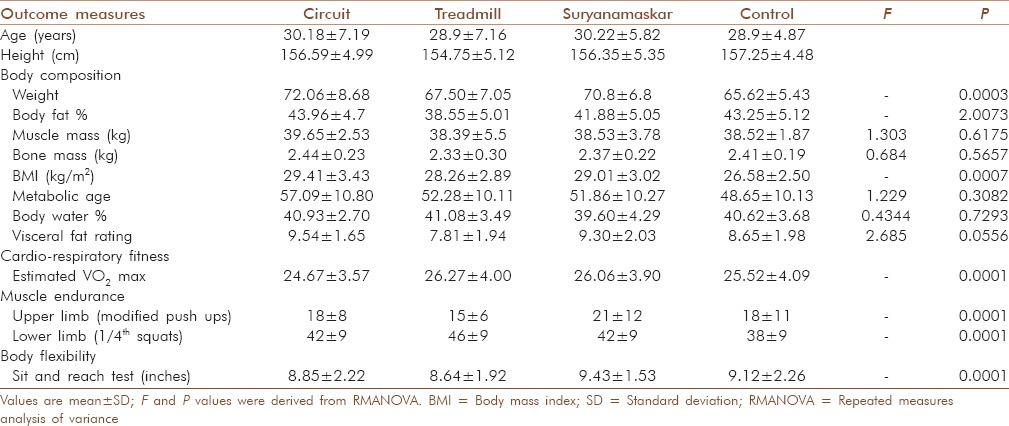
The baseline values of all the participants are represented in Table 2.
Table 2.
Participant's baseline parameters
Body composition outcomes
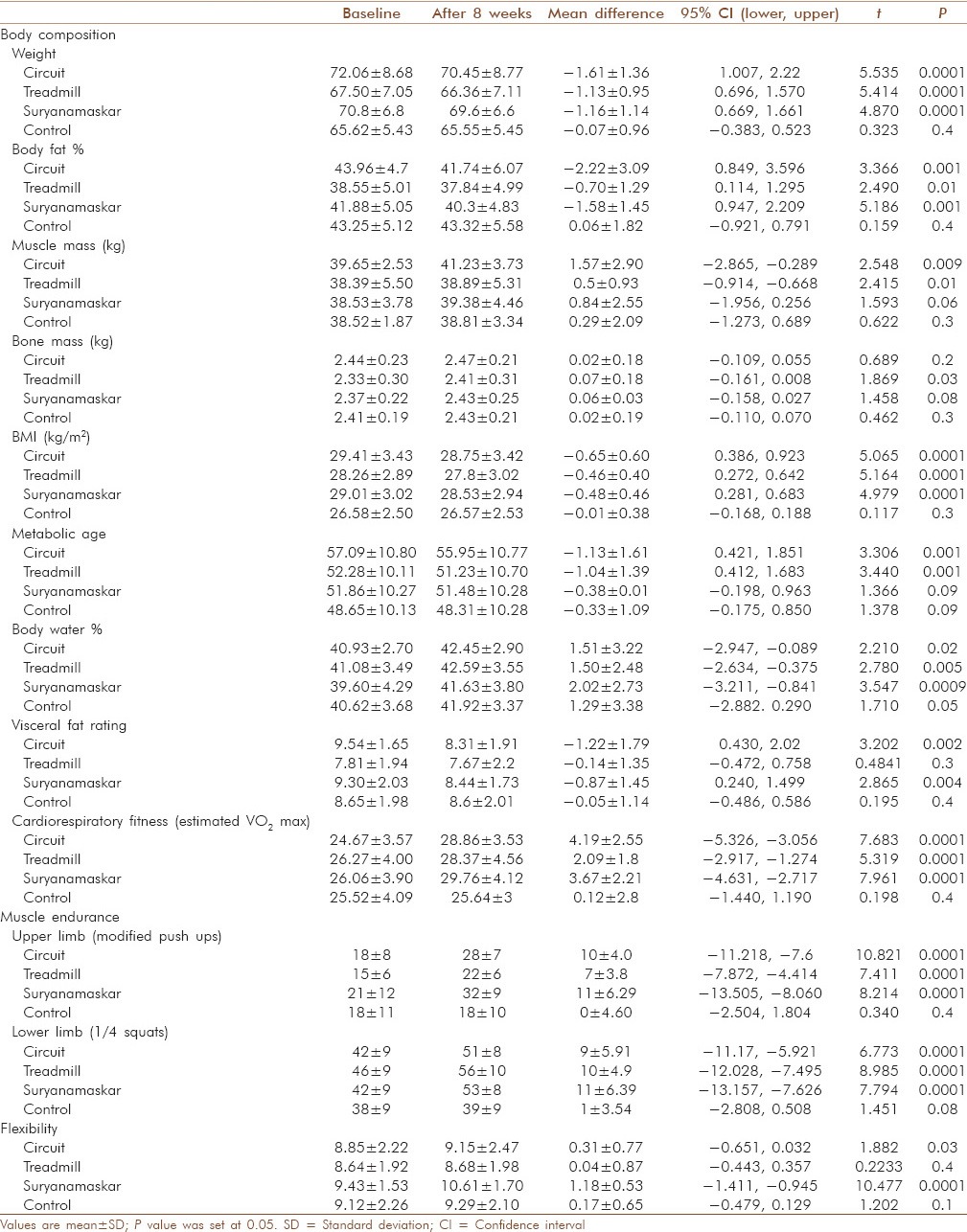
Post 8 weeks of training intervention, significant reduction was observed in mean body weight in CT group (2.2%, P < 0.001) as compared to control (0.1%, P = 0.3). Modest decrease were also observed in TM and SN group by (1.7% and 1.6%, [P < 0.05]) respectively. The change in BMI was significant in all the three groups (P < 0.01) as compared to control (P = 0.3). Between groups comparison was not significant. The total body fat % lowered significantly in the CT (5%, P < 0.01) and SN (3.7%, P < 0.01) groups as compared to control (−0.1%, P = 0.4). No significant change in fat % was noted with TM. No significant change was noted in muscle and bone mass between the groups. Within group analysis revealed significant improvement in muscle mass in CT (4%, P = 0.009). The metabolic age showed significant change with CT (2%, P = 0.001) and TM (2%, P = 0.001) as compared to control. Body water % improved by (3%, P = 0.02; 3.6%, P = 0.005; 5.1%, P = 0.0005) with CT, TM and SN training respectively. Inter group analysis was not significant. Visceral fat rating improved by (12.8%, P = 0.002) and (9.3%, P = 0.01) with CT and SN as compared to TM [Table 3].
Table 3.
Changes in body composition parameters
Cardiorespiratory fitness
VO2max significantly increased in the CT group by (17.2%, P = 0.0001) and (14%, P = 0.0001) with SN as compared to (8%, P = 0.0001) in TM group.
Muscle endurance
Modified push ups increased remarkably in CT and SN groups by 51.3% and 51.24%, P = 0.0001) and in TM group by (40%, P = 0.0001). 1/4th squat test showed increase with TM and SN (P = 0.001) by 21.2% and 24.5% as compared to control. Inter group results were insignificant.
Flexibility
Sit and reach test improved in SN by (12.4%, P = 0.0001) as compared to all other groups. A mild improvement in the CT group by (3.5%, P = 0.03) as compared to TM by only 0.5%.
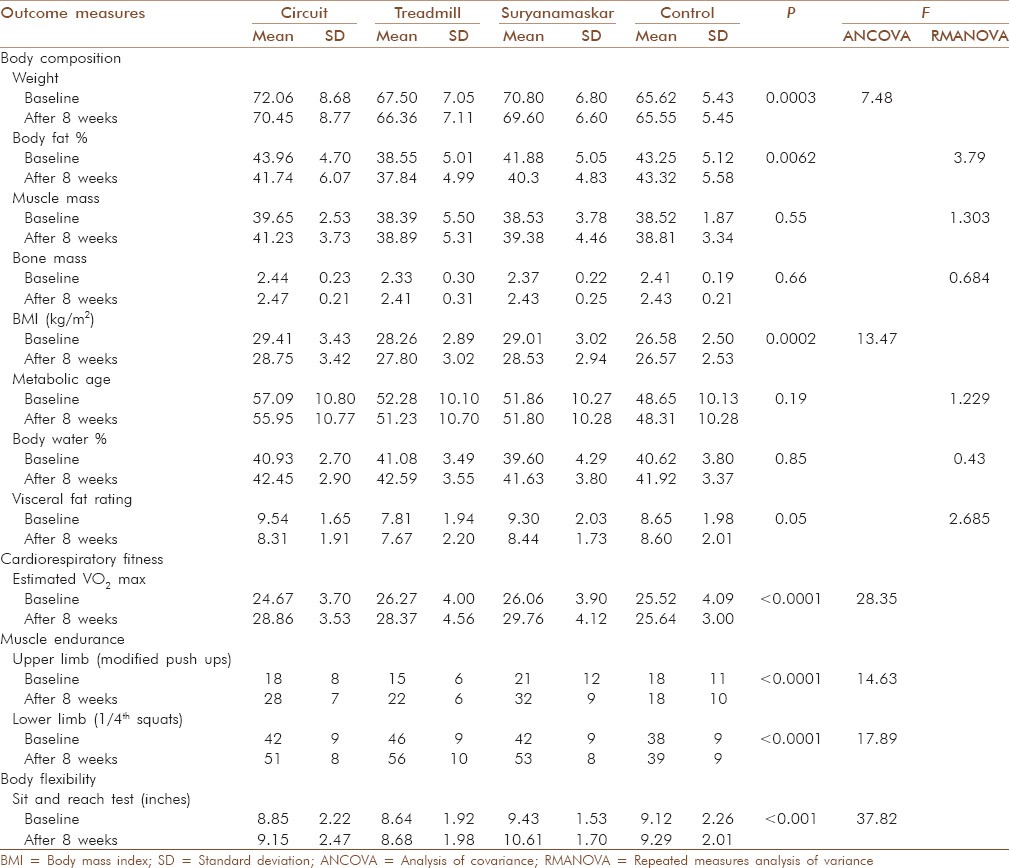
The study showed significant differences on ANCOVA (at 8 weeks after controlling for baseline) and RMANOVA (interaction effect) between groups in weight, fat %, BMI, CRF, muscle endurance and flexibility. There were no significant differences in muscle mass, bone mass, metabolic age, body water % and visceral fat ratings [Table 4].
Table 4.
ANCOVA test results
DISCUSSION
Circuit training produced greater reduction of weight followed by SN and TM training. BMI lowered equally in all groups as compared to control. However, on comparison between the groups, both of these parameters showed no change. This suggests that all 3 types of exercise training were equally effective in weight management. BMI calculation cannot differentiate lean body mass and fat mass and thus may be imprecise outcome to gauge obesity.
Lipids are major fuel source to the exercising muscles. Adding resistance to exercise may increase the energy expenditure leading to further fat oxidation. [22] Total body fat% lowered significantly with CT followed by SN by 5% and 3.8% respectively. Increase in visceral fat is associated with high risk of cardiovascular diseases and type II diabetes. Visceral fat ratings showed maximal reduction by 12.5% in CT followed by 9.3% in SN and barely in TM group (1.8%) as compared to control. Nevertheless no significant difference was noted on comparing between the groups.
Aerobic training when combined with resistance training was more effective in stimulating increase in the lean body mass as seen with CT by 4%, SN 2.2% and minimal change with TM of 1.2%. The change in muscle mass was significant, but difference between the groups was not. Increase in lean body mass caused by exercise may be associated with less reduction in total body weight. Study by Catenacci and Wyatt [23] showed that exercise training improves body composition often independent of weight loss. Hence change in body weight is less reliable as an only outcome.
In sedentary adults, there is decline in muscle tissue by 4-6 lbs per decade [24] and muscle efficiency also reduces. [25] This often leads to a drop in the resting metabolic rate and an increase in body fat. [26,27,28] Even 2-3% increase in resting metabolic rate could have the effect of reversing age-related weight and fat gain. [29] Aerobic exercise improves metabolic functions, especially enzymes in the muscles whereas, resistance training improves muscle protein synthesis and hence muscle mass. Aerobic exercise training also helps to maintain or slows down the loss of bone mass [30] whereas resistance training improves bone mass. [31] But no noteworthy change was observed in bone mass in any of the groups in the current study.
The metabolic age is calculated by comparing the basal metabolic rate of that chronological age group. Increase in lean body mass increases basal metabolic rate and thus lowers metabolic age. The metabolic age reduced appreciably by 1 year in CT and TM groups with no notable change in SN group. Any enhancement of fitness comes from alteration in several metabolic processes. [32] Regular exercise is also associated with changes in muscle morphology and metabolism that correspond to a marked decrease in metabolic risk [33] and increased life expectancy. [34]
The body mechanisms to regulate water content are compromised with increasing age which are further exacerbated with hormonal changes in menopause, medical conditions like hypertension and use of certain medications, e.g. diuretics. [35] Body water percentage is an imperative marker of ageing. Equivalent rise in body water % with SN, CT and TM training by 5.1%, 3.7% and 3.6% was noted in the present study.
Physical inactivity coupled with obesity increases the risk of cardiovascular and other obesity related diseases. [36] When assessing the impact of obesity on health status, CRF evaluation is fundamental part. Large observational studies [37,38] recommend that CRF is inversely related to morbidity and mortality in obesity. So, improvement in CRF may be more essential than changes in body weight or BMI in reducing the risk factors for obesity co-morbidities.
Cardiorespiratory fitness is best designated by maximal aerobic capacity, that is, VO2max. It reflects the oxygen delivery to the exercising muscles by the cardiovascular and respiratory system. CRF depends on maximal cardiac output and the ability of skeletal muscle to extract oxygen. Hence it enhances the ability to exercise for prolonged duration. VO2max based on the SWRT performance showed maximal improvement with CT (17%) followed by SN (14.1%) and modest increase with TM training (8%). Increase in CRF in all 3 groups was statistically significant. When comparing between the groups, CT and SN were equally effective while, CT was more effective as compared to TM training in improving CRF.
There are tall claims in weight management, but may not offer management of factors like endurance and flexibility which are impaired in obese people in such weight management programs.
Increase in mitochondrial size and number and mitochondrial enzymes is mediated by the repetitive contractile activity of the muscle. Also these adaptations are very specific to the type of muscle fibres recruited. Increase in muscle endurance would be because of the metabolic adaptations occurring with training are lower blood lactate levels which delays the development of fatigue and increased fat oxidation. [39] The upper limb muscle endurance improved equally in CT and SN group (51.4% and 51.2%) respectively. CT group involved loading of the upper limb specifically in push-up, pull down and biceps curls. In the CT group, the increased muscle endurance can be attributed to the low intensity training with higher number of repetitions (40% of 1 RM × 3 sets of 10 repetitions).
Also in SN with repetitive upper limb loading with body weight in specific aasanas of SN like Ashwanasanchalanasana, Chaturnamaskara and Bhujangasana would activate various upper limb muscles to maintain the posture in that particular aasana. Unlike this, there was no upper limb activity in TM training. An unexpected increase in TM group of (40%) was detected which further needs to be investigated. The lower limb muscle endurance demonstrated significant improvements in all exercise groups. Equal improvement was observed with SN and TM by 24.5% and 21.2% and 20.3% with CT.
Flexibility is the ability to move the joint through its complete ROM. [40] Insufficient ROM increases the risk of injury to the adjacent muscles and joints. Reduced flexibility may be because of various reasons like deskbound lifestyle, physical inactivity or deposition of fat around the joints restricting complete ROM. Alterations in flexibility can lead to various biomechanical changes in joints and altered postures. Hence, flexibility is needed to perform daily activities with ease. Significant increase in flexibility was seen in the CT and SN groups by 3.5% and 12.5%. Remarkable increase in flexibility by 12.5% in the SN group was observed as compared to 3.5% in CT group. The different postures in SN demanded movement till the end ROM which would be the reason of noteworthy change with SN training. Nonsignificant improvement was noted of 0.5% with TM training. Compared to the SN and CT, there is minimal motion at the hip, knee and the lumbar spine during TM walking thus resulting in reduced flexibility.
Thus, employing exercise leads to measurable improvements in overall health status. This improvement is as a result of improvement in metabolic status, more efficient musculoskeletal and the cardiorespiratory system that can lead to a parallel increase in lean tissue and reduction in fat mass. [41,42] It appears that as long as the increase in energy expenditure is sufficient, low to moderate-intensity endurance exercise is likely to generate beneficial metabolic effects similar to high-intensity exercise. [43]
Clinical implications
The present study suggests that any of these forms of exercise is beneficial for fitness and can be implemented for obesity management. Also, there are different types of benefits by different forms of exercise and no one method is superior to other, barring a few factors like flexibility. As far as time factor for exercise prescription was concerned, all three modes took an equal time of approximately 45-60 min, although a lesser time requirement has been documented in literature for SN. Thus, the authors recommend using SN is a better method as it has an added advantage of not requiring any instruments as in circuit and requires less space unlike walking. Hence, SN provides economic and time factor advantages and provides complete provision of fitness enhancement, including flexibility. This was not part of the research objectives though.
Limitations
Diet factor control or modification was not considered in the present study. More objective method for exercise intensity calculation was not used and only RPE was considered.
Although there are many literatures available on SN technique, no known documented evidence was obtained for the modified SN chair technique used in the study and establishing the reliability of this procedure itself is an important aspect. Workers in the field of SN suggest that more than 1400 different modifications can be possible in SN itself. This modified technique, in the present study, may be considered as the authors’ innovation to match the needs of the population under investigation.
CONCLUSION
All the three training methods, viz. SN training, CT and TM training are effective in weight management and improvisation of physical fitness parameters in over weight and obese females.
Of these, circuit and SN training was more effective in improving cardio-respiratory fitness and upper limb muscle endurance while only SN was effective in improving body flexibility.
ACKNOWLEDGEMENTS
The authors would like to thank all participants participating in the study. We would additionally like to thank Mr. Vishwas Shende of Laxmi Vyankatesh Charitable and Educational Trust and International Suryanamaskar Academy for helping us with literatures related to Suryanamaskar.
Footnotes
Source of Support: Institution: Sancheti Healthcare Academy, Sancheti Institute College of Physiotherapy, Thube Park, Shivajinagar, Pune. and Sancheti Institute of Orthopaedics and Rehabilitation Shivaji Nagar, Pune
Conflict of Interest: None declared.
REFERENCES
- 1.World Health Organization. Report of a WHO Consultation Presented at: The World Health Organization. Geneva, Switzerland: Publication WHO/NUT/NCD/98.1; 1997. Obesity: Preventing and Managing the Global Epidemic. [PubMed] [Google Scholar]
- 2.Singh RB, Pella D, Mechirova V, Kartikey K, Demeester F, Tomar RS, et al. Prevalence of obesity, physical inactivity and undernutrition, a triple burden of diseases during transition in a developing economy. The Five City Study Group. Acta Cardiol. 2007;62:119–27. doi: 10.2143/AC.62.2.2020231. [DOI] [PubMed] [Google Scholar]
- 3.Chopra SM, Misra A, Gulati S, Gupta R. Overweight, obesity and related non-communicable diseases in Asian Indian girls and women. Eur J Clin Nutr. 2013;67:688–96. doi: 10.1038/ejcn.2013.70. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. Report of a Joint WHO/FAO Expert. Consultation. Diet, Nutrition and the Prevention of Chronic Diseases. WHO Technical Report Series No. 916. [Last viewed on 2014 Oct 16]. Available from: http://www.whqlibdoc.who.int/trs/who_trs_916.pdf .
- 5.Parizkova J, Chin MK, Chia M, Yang J. An international perspective on obesity, health and physical activity: Current trends and challenges in China and Asia. J Exerc Sci Fit. 2007;5:7–23. [Google Scholar]
- 6.WHO Report. 2007. [Last viewed on 2011 Feb 14]. Available from: http://www.who.int/mediacentre/factsheets/fs311/en/
- 7.Ross A, Thomas S. The health benefits of yoga and exercise: A review of comparison studies. J Altern Complement Med. 2010;16:3–12. doi: 10.1089/acm.2009.0044. [DOI] [PubMed] [Google Scholar]
- 8.Bhavanani AB, Udupa K, Madanmohan, Ravindra P. A comparative study of slow and fast suryanamaskar on physiological function. Int J Yoga. 2011;4:71–6. doi: 10.4103/0973-6131.85489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kaikkonen H, Yrjämä M, Siljander E, Byman P, Laukkanen R. The effect of heart rate controlled low resistance circuit weight training and endurance training on maximal aerobic power in sedentary adults. Scand J Med Sci Sports. 2000;10:211–5. doi: 10.1034/j.1600-0838.2000.010004211.x. [DOI] [PubMed] [Google Scholar]
- 10.Paoli A, Pacelli F, Bargossi AM, Marcolin G, Guzzinati S, Neri M, et al. Effects of three distinct protocols of fitness training on body composition, strength and blood lactate. J Sports Med Phys Fitness. 2010;50:43–51. [PubMed] [Google Scholar]
- 11.Wilmore JH, Parr RB, Girandola RN, Ward P, Vodak PA, Barstow TJ, et al. Physiological alterations consequent to circuit weight training. Med Sci Sports. 1978;10:79–84. [PubMed] [Google Scholar]
- 12.Mayorga-Vega D, Viciana J, Cocca A. Effects of a Circuit Training Program on Muscular and Cardiovascular Endurance and their Maintenance in Schoolchildren. J Hum Kinet. 2013;37:153–60. doi: 10.2478/hukin-2013-0036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Romero-Arenas S, Martínez-Pascual M, Alcaraz PE. Impact of resistance circuit training on neuromuscular, cardiorespiratory and body composition adaptations in the elderly. Aging Dis. 2013;4:256–63. doi: 10.14336/AD.2013.0400256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Physical Activity and Health: A Report of the Surgeon General. Atlanta: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996. Department of Health and Human Services. [Google Scholar]
- 15.Browning RC, Kram R. Effects of obesity on the biomechanics of walking at different speeds. Med Sci Sports Exerc. 2007;39:1632–41. doi: 10.1249/mss.0b013e318076b54b. [DOI] [PubMed] [Google Scholar]
- 16.Browning RC, Kram R. Energetic cost and preferred speed of walking in obese vs. normal weight women. Obes Res. 2005;13:891–9. doi: 10.1038/oby.2005.103. [DOI] [PubMed] [Google Scholar]
- 17.Cochrane WG. Sampling Techniques. 2nd ed. New York: John Wiley and Sons, Inc; 1967. [Google Scholar]
- 18.Mikawa K, Senjyu H. Development of a field test for evaluating aerobic fitness in middle-aged adults: Validity of a 15-m incremental shuttle walk and run test. J Sports Sci Med. 2011;10:712–7. [PMC free article] [PubMed] [Google Scholar]
- 19.López-Miñarro PA, Andújar PS, Rodrñguez-Garcña PL. A comparison of the sit-and-reach test and the back-saver sit-and-reach test in university students. J Sports Sci Med. 2009;8:116–22. [PMC free article] [PubMed] [Google Scholar]
- 20.FITNESSGRAM/ACTIVITYGRAM Test Administration Manual. 4th ed. Champaign, IL: Human Kinetics; 2007. [Last viewed on 2014 Oct 16]. The Cooper Institute. Available from: http://www.humankinetics.com/products/all-products/the-fitnessgramactivitygramtest-administration-manual-updated-4th-edition. and http://www.cooperinstitute.org/vault/2440/web/files/662.pdf . [Google Scholar]
- 21.The President's Council on Physical Fitness and Sports: Department of Health and Human Services. “Definitions: Health, Fitness and Physical Activity”. [Last viewed on 2014 Oct 16]. Available from: https://www.presidentschallenge.org/informed/digest/docs/200003digest.pdf .
- 22.Smekal G, von Duvillard SP, Pokan R, Tschan H, Baron R, Hofmann P, et al. Effect of endurance training on muscle fat metabolism during prolonged exercise: Agreements and disagreements. Nutrition. 2003;19:891–900. doi: 10.1016/s0899-9007(03)00171-0. [DOI] [PubMed] [Google Scholar]
- 23.Catenacci VA, Wyatt HR. The role of physical activity in producing and maintaining weight loss. Nat Clin Pract Endocrinol Metab. 2007;3:518–29. doi: 10.1038/ncpendmet0554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Forbes GB, Halloran E. The adult decline in lean body mass. Hum Biol. 1976;48:161–73. [PubMed] [Google Scholar]
- 25.Nair KS. Aging muscle. Am J Clin Nutr. 2005;81:953–63. doi: 10.1093/ajcn/81.5.953. [DOI] [PubMed] [Google Scholar]
- 26.Wolfe RR. The underappreciated role of muscle in health and disease. Am J Clin Nutr. 2006;84:475–82. doi: 10.1093/ajcn/84.3.475. [DOI] [PubMed] [Google Scholar]
- 27.Kyle UG, Genton L, Hans D, Karsegard L, Slosman DO, Pichard C. Age-related differences in fat-free mass, skeletal muscle, body cell mass and fat mass between 18 and 94 years. Eur J Clin Nutr. 2001;55:663–72. doi: 10.1038/sj.ejcn.1601198. [DOI] [PubMed] [Google Scholar]
- 28.Mazariegos M, Wang ZM, Gallagher D, Baumgartner RN, Allison DB, Wang J, et al. Differences between young and old females in the five levels of body composition and their relevance to the two-compartment chemical model. J Gerontol. 1994;49:M201–8. doi: 10.1093/geronj/49.5.m201. [DOI] [PubMed] [Google Scholar]
- 29.Astrup A. Thermogenic drugs as a strategy for treatment of obesity. Endocrine. 2000;13:207–12. doi: 10.1385/ENDO:13:2:207. [DOI] [PubMed] [Google Scholar]
- 30.Ryan AS, Nicklas BJ, Dennis KE. Aerobic exercise maintains regional bone mineral density during weight loss in postmenopausal women. J Appl Physiol (1985) 1998;84:1305–10. doi: 10.1152/jappl.1998.84.4.1305. [DOI] [PubMed] [Google Scholar]
- 31.Iwamoto J, Sato Y, Takeda T, Matsumoto H. Effectiveness of exercise in the treatment of lumbar spinal stenosis, knee osteoarthritis, and osteoporosis. Aging Clin Exp Res. 2010;22:116–22. doi: 10.1007/BF03324783. [DOI] [PubMed] [Google Scholar]
- 32.Clark JE. An overview of the contribution of fatness and fitness factors, and the role of exercise, in the formation of health status for individuals who are overweight. J Diabetes Metab Disord. 2012;11:19. doi: 10.1186/2251-6581-11-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kelley DE, Goodpaster BH. Skeletal muscle triglyceride. An aspect of regional adiposity and insulin resistance. Diabetes Care. 2001;24:933–41. doi: 10.2337/diacare.24.5.933. [DOI] [PubMed] [Google Scholar]
- 34.Berrington de Gonzalez A, Hartge P, Cerhan JR, Flint AJ, Hannan L, MacInnis RJ, et al. Body-mass index and mortality among 1.46 million white adults. N Engl J Med. 2010;363:2211–9. doi: 10.1056/NEJMoa1000367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mack Gary W. ACSM Current Comment: Dehydration and Aging. [Last viewed on 2014 Oct 16]. Available from: http://www.acsm.org/docs/current.comments/dehydrationandaging.pdf .
- 36.Krauss RM, Winston M, Fletcher BJ, Grundy SM. Obesity: Impact on cardiovascular disease Circulation. 1998;98:1472–6. [PubMed] [Google Scholar]
- 37.Barlow CE, Kohl HW, 3rd, Gibbons LW, Blair SN. Physical fitness, mortality and obesity. Int J Obes Relat Metab Disord. 1995;19(Suppl 4):S41–4. [PubMed] [Google Scholar]
- 38.Lee CD, Jackson AS, Blair SN. US weight guidelines: Is it also important to consider cardiorespiratory fitness? Int J Obes Relat Metab Disord. 1998;22(Suppl 2):S2–7. [PubMed] [Google Scholar]
- 39.Holloszy JO, Coyle EF. Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J Appl Physiol Respir Environ Exerc Physiol. 1984;56:831–8. doi: 10.1152/jappl.1984.56.4.831. [DOI] [PubMed] [Google Scholar]
- 40.Fatouros IG, Taxildaris K, Tokmakidis SP, Kalapotharakos V, Aggelousis N, Athanasopoulos S, et al. The effects of strength training, cardiovascular training and their combination on flexibility of inactive older adults. Int J Sports Med. 2002;23:112–9. doi: 10.1055/s-2002-20130. [DOI] [PubMed] [Google Scholar]
- 41.Farrell SW, Fitzgerald SJ, McAuley PA, Barlow CE. Cardiorespiratory fitness, adiposity, and all-cause mortality in women. Med Sci Sports Exerc. 2010;42:2006–12. doi: 10.1249/MSS.0b013e3181df12bf. [DOI] [PubMed] [Google Scholar]
- 42.Balducci S, Zanuso S, Nicolucci A, Fernando F, Cavallo S, Cardelli P, et al. Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the metabolic syndrome is dependent on exercise modalities and independent of weight loss. Nutr Metab Cardiovasc Dis. 2010;20:608–17. doi: 10.1016/j.numecd.2009.04.015. [DOI] [PubMed] [Google Scholar]
- 43.Poirier P, Després JP. Exercise in weight management of obesity. Cardiol Clin. 2001;19:459–70. doi: 10.1016/s0733-8651(05)70229-0. [DOI] [PubMed] [Google Scholar]