

Abstract
The impact of retinoic acid (All Trans Retinoic Acid; ATRA) in the development of lung pathology and tissue remodeling are not well established in the literature. As well, the role of citral (inhibitor of retinoid function) in the improvement of lung pathology was not ascertained under an in vivo setting. Therefore, it is hypothesized that ATRA and ovalbumin exposure will sensitize lung tissues leading to lung tissue pathology and that citrals (C1 and C2) will reverse or ameliorate the related pathological damage to lung tissues. The study used an IACUC approved between-subject in vivo randomized split plot factorial design (F344 rat model; N=40). Animals were exposed to 8 different treatments including vehicle, OVA, ATRA, citrals (C1 and C2) and their ovalbumin combinations (OVA+ ATRA, OVA+ C1, and OVA+ C2) by intra-peritoneal route. Rat weight data and blood were collected on Days 1 and 21, all animals were sacrificed on day 21 and lung tissues were processed for histopathology. Results from weights and blood (ANOVA and Duncan) as well as from the histopatholgical analysis supported the findings that exposure of F344 rats to OVA combinations with ATRA and citrals showed various levels of lung tissue damage that was improved or worsened by either C1 or C2. This promising study showed variable responses on the interaction of ovalbumin, citrals, and ATRA as related to their damage/improvement of related lung tissue pathologies.
Keywords: ATRA, RP, Citral, F344, Ovalbumin, Chronic Lung Pathology, Hpervitaminosis A
INTRODUCTION
The impact of retinoic acid (All Trans Retinoic Acid; ATRA) in the development of lung pathology and tissue remodeling are not well established in the literature. As well, the role of citral (inhibitor of retinoid function) in the improvement of lung pathology was not ascertained under an in vivo setting. Retinoids represent the chemical derivatives of vitamin A or all-trans retinol. These include retinol, retinaldehyde, and all forms of the final oxidized product retinoic acid (RA).Vitamin A is generally obtained from the diet in the form of retinyl esters that are linked to fatty acids such as palmitic acid (retinylpalmitate; RP) or in the form of carotenoids which are dimmers of retinal; the oxidative aldehyde form of retinoid isomers [1, 2, 3 and 4]. The current known clinical uses of some selected retinoids include the treatment of dermatologic diseased such as acne, psoriasis, eczema, photo-damaged skin and specific forms of cancer [2, 4]. Biological effects of retinoids are generally exerted through a series of nuclear receptors that are ligand-inducible transcription factors belonging to the steroid/thyroid receptor superfamily such as RAR and RXR retinoid nuclear receptors (1, 2, 1nd 5).
Recent challenges in the treatment of chronic lung disease including restoration of alveolar surface area, respiratory and mechanical function of the lung parenchyma has lead to a focus on retinoids as therapeutic agents [6, 7, and 8].
It is known that alveolar architecture depends on the anatomy of prenatal airways in mice, rats and humans. Airway branching, elongation and cellular differentiation are influenced by retinoids, however, one of the important component of the alveolus is the septum which is composed of epithelial and endothelial cells, fibroblasts and some immune and neuro-endocrine cells. Retinoids are known alveolar morphogens from the fact that RA was shown to ameliorate emphysema in rats after the intra-tracheal instillation of elastase [9, 10, and 11].
Circulating retinoids as well as the endogenous stores furnish the required amounts of retinoids to body cells through the hydrolysis of RP [12, 13]. Retinoids are pleiotropic regulatory compounds that are capable of modulating the structure and function of a wide range of inflammatory, immune and structural body cells. They possess a hormone-like function that regulate epithelial cell proliferation, pattern formation in developing tissues, morphogenesis in the lung and cellular differentiation [14].
Citral has been reported to exhibit activity as a Vitamin A antagonist by inhibiting the oxidation of retinal to retinoic acid. This suggests that Citral is able to block the endogenous RA signaling pathway [15].
Hypervitaminosis A is a condition representing retinoid toxicity, which may reflect its effects on the lungs as a damaging agent. To this end and in reference to the literature where the findings on the responses to ATRA both in vitro and in vivo appeared to be contadicting [2, 3 and 16]. This study was undertaken to explore this contraversy.
This paradox in the function of retinoids [17-23] as curing or damaging agents prompted the execution of our study with the hypothesis that application of supraphysiologic levels of retinoids ATRA will cause lung pathologic damage similar to ovalbumin exposure. The objective of the study, however, was to assess the role of exposing the F344 rat model to supraphysiologic levels of OVA+ATRA, OVA+C1, OVA+C2, and their comparison to untreated control and single treatments including OVA, ATRA, C1 and C2, .and to provide some insights into the role of Citral in ameliorating such pathology as it relates to the treatment of chronic lung disease in an in vivo setting.
METHODS
High purity All Trans Retinoic Acid (ATRA), Ovalbumin, Ova, Aluminum hydroxide, Citral 1 (C1; diethyl acetal and Citral 2 (C2; cis and Trans dimethyl), DMSO, Isoflurane and PBS were obtained from Sigma Aldrich Company, St. Louis, MO).
Animals and housing
Fisher rats (F344; 260-324 g) were obtained from Harlan Laboratories (Frederic, MD). The animals were housed at the Jackson State University (JSU) Animal Core Facilities (Olaw class 2 level). Animals were acclimatized for a week and all protocols including handling, husbandry, anesthesia, euthanasia, and experimental protocols were approved by JSU-IACUC (protocol # 08-13-08) and were performed according to Olaw recommendations. Animals were kept under controlled environment at 12/12 light /dark cycles and were allowed unrestricted access to water and rodent chow. Each animal was kept in a separate rat cage that is well maintained by a technical staff supervised by a veterinarian.
Experimental design
A total of 40 F344 rats were used in this study. Five animals were not treated and designated as negative control. The remaining 35 animals were divided into 7 different groups of 5 animals each and were exposed as based on treatment group through intra-peritoneal (iP) and intratracheal (iT) routes on day 1 using ovalbumin-Aluminum hydroxide (OVA), all trans retinoic acid (ATRA, citral 1 (C1), citral 2 (C2) by the intra-peritoneal route and mold (Mold) by iT route (treatment dosing is displayed on table 2.1). All animals were weighed on days 1 and 21 and were sacrificed (euthanized by inhalation of CO2 in special chamber) on day 21 following approved protocols and blood was collected for parameter analysis.. Dead animals were subjected to in-house post-mortem (Necropsy) procedures and entire lungs from all animals were collected in 10% formalin for histopathological analysis.
Tissue processing, slide preparation and digitizing
Formalized lung tissue was processed for histopathology following standard procedures. Tissues were embedded in paraffin blocks and were then sectioned using a Lecia Microtome to produce 5μm sections. Sections were floated in a water bath, adhered to standard glass slides and allowed to dry. Slides were then stained using standard Hematoxylin and Eosin staining procedure for further analysis. Slides were examined under the microscope and digitized into photos to document pathological changes from the impact of their exposure to these chemicals.
RESULTS
Data on the comparison of weight data and survival of F344 rats exposed to 8 different treatments is presented on table 1. Animal weights ranged between 229±9.5 and 305.6±3.0 g. As can be seen, addition of ATRA to Ova is synergistic (97.05, 91.55 vs 162.03* %) for weight gain. The addition of C1 to OVA reversed the negative effect for weight gain by C1 and produced non-significant effects as compared to the –, and OVA controls. The addition of C2 to OVA is, however, antagonistic to weight gain as compared to both controls (97.05, 91.55 vs 65.82* %). It is worth noting that, OVA+C2 combination produced a non-significant synergistic weight gain effect when compared to the C2 control (improved; 65.82* vs 27.50* %). All animals in this group survived to term.
Table 1.
Comparison of weight data and survival of F344 rats exposed to ATRA, OVA+ATRA, C1, OVA+C1, C2, OVA+C2, and OVA (n=40)
| # | Treatment Type |
N | Initial Weight (g) |
Final Weight (g) |
Weight Difference (g) |
Standard Difference (g) |
Weight Gain/Av Control % |
Survival to term |
|---|---|---|---|---|---|---|---|---|
| 1 | − Control | 5 | 264.0±8.0 | 287.7±2.6 | 23.7 | 0.00 | 100.00 | +++++ |
| 2 | + ATRA Cont. | 5 | 229.7±9.5 | 251.3±17.6 | 21.7 | −2.00 | 91.55 | +++++ |
| 7 | OVA + ATRA | 5 | 264.6±17.9 | 303.0±7.9 | 38.4* | +14.70 | 162.03 | +++++ |
| 3 | + C1 Control | 5 | 244.6±10.3 | 255.0±4.6 | 10.4* | −13.30 | 44.00 | +++++ |
| 8 | OVA + C1 | 5 | 255.7±13.2 | 278.0±11.9 | 22.3 | −1.40 | 94.09 | +++++ |
| 4 | + C2 Control | 5 | 261.4±8.4 | 267.9±9.8 | 6.5* | −17.12 | 27.50 | +++++ |
| 9 | OVA + C2 | 5 | 253.4±2.8 | 269.0±2.06 | 15.6* | −8.10 | 65.82 | +++++ |
| 5 | + OVA Control | 5 | 272.6±3.8 | 305.6±3.0 | 23.0 | −0.70 | 97.05 | +++++ |
Statistically significant at p<0.05.
In summary, ATRA and Ova are highly synergistic, OVA is antagonistic to the effects of C1and that is in contrast to its effects on the negative effects of C2 on weight gain (Table 1).
Data on the comparison of RBC parameters for the F344 rat model exposed to 8 different treatments is presented in table 2. As can be seen only C1showed significant difference for RBCs (−2.20±1.90* M/μL). HCT showed significance for both ATRA and OVA controls (−4.35±10.50* and 4.38±2.28* %). The MCV parameter did not show significance for any of the 8 treatments and HB showed significance for C1 control only (−3.10±2.70* g/dl). MCH showed significance for OVA+C1 (−2.08±0.10* pg) and MCHC showed significance for both ATRA (−4.03±2.43* g/dl) and C2 (−3.93±3.53* g/dl) controls. All changes are negative except for C1 on RBCs. Means for these parameters were within the reference mean range for this model.
Table 2.
Comparison of RBC parameters (centered**) of F344 rats exposed to ATRA, OVA+ATRA, C1, OVA+C1, C2, OVA+C2, and OVA (n=40)
| # | Treatment Type |
N | RBCs (M/μL) |
HCT (%) |
MCV (fl) |
Hb (g/dl) |
MCH (pg) |
MCHC (g/dl) |
|---|---|---|---|---|---|---|---|---|
| 1 | −Control | 5 | 1.11±0.69 | 12.84±3.92 | 2.48±0.95 | 0.72±0.97 | −1.46±0.38 | −5.20±1.07 |
| 2 | + ATRA Cont. | 5 | −0.96±0.50 | −4.35±10.5* | −2.80±1.00 | −2.03±0.85 | −0.43±0.21 | −4.03±2.43* |
| 7 | OVA + ATRA | 5 | 0.52±0.70 | −2.55±4.86 | 2.12±1.55 | −2.23±0.85 | −1.37±0.73 | −4.45±0.828 |
| 3 | + C1 Control | 5 | −2.20±1.9* | −0.63±2.02 | 1.68±0.43 | −5.10±2.7* | −1.10±1.21 | −3.98±0.618 |
| 8 | OVA + C1 | 5 | −0.68±0.41 | −2.32±4.31 | 0.44±0.93 | −3.03±0.69 | −2.08±0.1* | −2.95±1.81 |
| 4 | + C2 Control | 5 | −0.39±0.37 | −2.57±2.72 | 0.50±0.40 | −2.18±0.54 | −1.63±0.29 | −3.93±3.53* |
| 9 | OVA + C2 | 5 | ND | ND | ND | ND | ND | ND |
| 5 | + OVA Cont. | 5 | 0.04±0.26 | 4.38±2.28* | 0.80±1.06 | −0.85±0.54 | −1.00±0.14 | −3.00±0.67 |
| Ref. Mean* | 8.95±1.69 | 52.24±3.90 | 54.48±2.95 | 15.72±2.80 | 18.36±1.38 | 35.20±1.07 |
Statistically significant at p<0.05.
Data centered on mean of pretreatment group.
In summary, ATRA alone showed negative effects on both HCT and MCHC, while OVA control showed negative effects on only HCT, however, the combination of OVA and ATRA abolished both negative effects confirming the synergistic positive effects on RBC parameters. The C1 control produced negative effects on RBCs and its combination with OVA removed the negative effects of both on RBC parameters but produced a negative effect on the MCH parameter and is showing a synergistic effect of the combination on RBC parameters; in contrast the their antagonistic relationship for weight gain. OVA and C2 combination is inconclusive because of unavailable data on this parameter (Table 2).
Data on lymph and WBC parameters upon exposure to 8 different treatments is presented in table 3. All 8 treatments did not show significant differences from control means for Lymph and monocytes. As can be seen, WBCs showed significance for OVA+ ATRA only (−12.50±9.20* k/μL). Eosinophils showed significance for C1 control (3.00±2.00* %), OVA+C1 (−3.00±0.82* %) and C2 control (−1.50±1.00* %). The Segs parameter showed significance for ATRA control (−9.00±6.53* %) and OVA+C1 (6.16±13.8* %). All changes are negative except for Segs and OVA+C1. Means for these parameters were within the reference mean range for this model.
Table 3.
Comparison of Lymph and WBC parameters (centered**) of F344 rats exposed to ATRA, OVA+ATRA, C1, OVA+C1, C2, OVA+C2, and OVA (n=40)
| # | Treatment Type |
N | Lymph (%) |
WBC (k/μL) |
Monocytes (%) |
Eosinophils (%) |
Segs (%) |
|---|---|---|---|---|---|---|---|
| 1 | −Control | 5 | 0.00±0.00 | 2.01±3.70 | 0.70±1.79 | −1.00±0.00 | −16.15±3.85 |
| 2 | + ATRA Cont. | 5 | 0.00±0.00 | −0.33±2.80 | 0.00±0.00 | −0.50±1.00 | −9.00±6.53* |
| 7 | OVA + ATRA | 5 | 0.00±0.00 | −12.50±9.2* | 0.00±0.00 | 0.00±1.03 | 2.13±3.37 |
| 3 | + C1 Control | 5 | 0.00±0.00 | −1.58±2.85 | 0.00±0.00 | 3.00±2.00* | −0.25±10.84 |
| 8 | OVA + C1 | 5 | 0.00±0.00 | −1.98±1.72 | 0.00±0.00 | −3.00±0.82* | 6.16±13.8* |
| 4 | + C2 Control | 5 | 0.00±0.00 | 0.35±1.08 | 0.00±0.00 | −1.50±1.00* | −1.50±7.33 |
| 9 | OVA + C2 | 5 | ND | ND | ND | ND | ND |
| 5 | + OVA Cont. | 5 | 0.00±0.00 | −1.83±2.43 | 0.00±0.00 | 1.00±0.00 | −4.50±3.42 |
| Ref. Mean* | 82.20±5.12 | 8.80±1.97 | 2.00±0.67 | 0.00±0.00 | 33.10±2.34 |
Statistically significant at p<0.05.
Data centered on mean of pretreatment group.
ND=no data
In summary, OVA and ATRA confirmed their positive synergism on WBC parameters. However, OVA did not reverse the negative effects of C1 on the WBC parameters and the C2 data is inconclusive (Table 3).
In Fig 1 and fig 4 the Ova+ATRA (7) combined treatment shows that the bronchial epithelium is columnar, congestion is very evident, papillary projections are prevalent in the alveoli, alveoli and vessels are constricted, alveolar walls are thick and showing areas of significant inflammation (synergistic and consistent with hypersensitivity). As can be seen in Figure 3.2.2 and fig 3.2.3 (400x magnifications): (7 and 7A) Ova+C1 treatment of the F344 rat lung is portraying thick alveolar walls, evident congestion, prevalent papillary projections but their appearance changes with decreased surface area, cuboidal shaped epithelium instead of columnar shaped, constricted vessels and dilated alveoli (consistent with lung damage). (9 and 9A) Ova+C2 treatment of the F344 rat lung illustrating various thick and thin alveolar walls, apparent congestion, red blood cells within alveoli and thick walled and narrow vessels. Further details show (9A) Ova+C2 treatment to F344 rat lung illustrating evident congestion and thin and thick alveoli at a high magnification.
Fig 1.

Comparison of lung pathology of F344 rats exposed to OVA + C1 (8), OVA + ATRA (7) and OVA + C2 (9). In comparison to relative controls, OVA + C1 show loss of alveolar boarders as well as loss of alveolar projections. OVA + ATRA show constriction of alveoli and loss of lung space. OVA + C2 showed eosinophilia changes and lung structure destruction.
Figure 4.
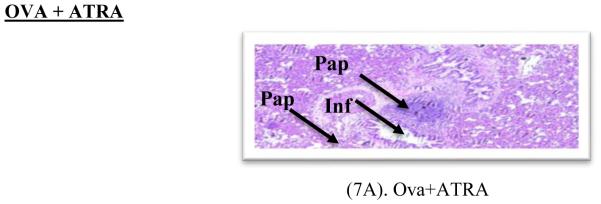
Ovalbumin sensitized lung histopathological display of Fischer 344 rat model. As seen in Figure 4: (7A) OVA+ A1RA treatment of the F344 rat lung illustrating the presence of a columnar epithelium, evident congestion; presence of papillary projections in the alveoli, constricted alveoli and vessels, alveolar walls that are thick and area evidence of significant inflammation; 400x.
Additionally (9) Ova+C2 treatment to F344 rat lung illustrates congestion in alveoli and vessel, thin and thick walled alveoli and the presence of papillary projections. Furthermore, Ova+C2 treatment to F344 rat lung illustrates bronchi with papillary projection, thick walled alveoli and congestion, congestion with red blood cells in alveoli, thick wall alveoli, presence of papillary projections lined by columnar epithelium, congestion, thick walled alveoli, presence of papillary projections lined by columnar epithelium and thick walled and thin vessels, congestion and thick walled alveoli, presence of papillary projections lined by columnar epithelium, apparent vein present and thick walled and thin vessels. (9B) Ova+C2 treatment to F344 rat lung illustrating thin walled alveoli. Ova+C2 treatment to F344 rat lung also illustrates evident congestion and thin and thick alveoli at a different slide position. (9C) Ova+C2 treatment to F344 rat lung illustrating thin walled alveoli at a higher magnification. Ova+C2 treatment to F344 rat lung also illustrates papillary projections with thick and thin alveolar walls but mostly thin, congestion and the presence of red blood cells. (9D) Ova+C2 treatment to F344 rat lung illustrating thin walled alveoli within a different position of slide.
Ova+C2 treatment to F344 rat lung also illustrates papillary projections, thin and thick walled alveoli, inflammatory cells and congestion. In comparison, the single treatment controls are showing as seen in figure 1 (1) depicts negative or no treatment control of the F344 rat lung illustrating normal lung tissue of with bronchial walls as well as variable sized bronchioles made up of ciliated pseudostratified columnar epithelium and smooth muscles. (5) is OVA control treatment of the F344 rat lung showing hypersensitivity, congestion of blood vessels and damaged bronchi (2) Depicts the ATRA control treatment of the F344 rat lung showing thickening and constriction of alveoli, congestion, constricted vessels and appearance of papillary projections into lumen bronchioles. (3) The C1 control treatment of the F344 rat lung illustrating an abundance of papillary projections, very thick alveolar walls, more basophilic condition, normal columnar epithelium, evident congestion and constricted vessels and alveoli. (4) The C2 Control treatment of the F344 rat lung illustrating thick alveolar walls but no inflammation, eosinophilic appearance, thick walled and dilated blood vessels with numerous red blood cells, vessel congestion and major constriction of the alveoli.
In summary, OVA+ATRA caused synergistic hypersensitivity, bronchoconstriction and lung congestion as compared to both controls. OVA+C1 should an antagonistic interaction consistent with the improvement of lung pathology. OVA+C2 caused a synergistic effect of the combination in causing more lung damage and impairment as compared to the two individual controls (Fig 5).
Figure 5.
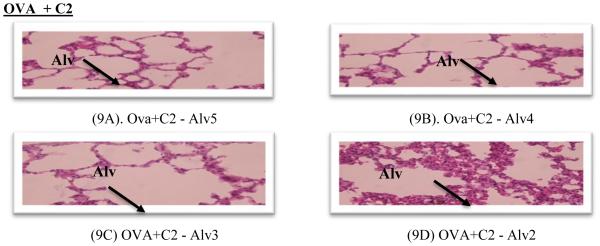
Ovalbumin sensitized lung histopathological display of Fischer 344 rat model. As seen in Figure 5: (9A) OVA+C2 treatment to F344 rat lung illustrating thin walled alveoli. (9B) OVA+C2 treatment to F344 rat lung illustrating thin walled alveoli at a higher magnification. (9C) OVA+C2 treatment to F344 rat lung illustrating thin walled alveoli within a different position of slide. (9D) OVA+C2 treatment to F344 rat lung illustrating evident congestion and thin and thick alveoli at a high magnification; 400 xs.
DISCUSSION
In regards to ATRA (94.05; no effect) and OVA (91.55; no effect), the combination treatment had a highly synergistic positive impact on weight gain (162.03%), while OVA (97.05; no effect) and C1 (44.0; low weight gain) combination treatment reversed the negative impact of C1 (44.0); the combination treatment had an antagonistic positive impact on weight gain (94.09; no effect), which is in contrast to the effects of OVA (no effect) and C2 (low weight gain; 27.50%) combination treatment that has not fully reversed the negative impact of C2 treatment on weight gain producing a lower (weaker reversal) antagonistic positive impact on weight gain; 65.82%, statistically signifi cant difference from -control (Table 1). Hence, OVA in combination with citral have strongly reversed the negative impact on weight gain by C1; however, the reversal impact was lower for C2 treatment though not statistically significant from any effect by OVA or –control treatments. Citral in a dose of 300mg/kg body weight in 1 ml of olive oil, by single intraperitoneal injection for 14 consecutive days in rats led to reduction in weights of the testes, epididymis, seminal vesicles, prostate and plasma testosterone levels [24, 25].
In reference to their effects on blood parameters, all tra ns-retinoic acid (ATRA) treatment alone showed negative effects on both HCT and MCHC, while OVA control showed negative effects on only HCT, however, the combination of OVA and ATRA abolished both negative effects confirming their synergistic positive effe cts on the RBC parameters. The C1 control produced negative effects on RBCs and its combination with OVA removed the negative effects of both on RBC parameter but produced a negative effect on the MCH parameter showing an antagonistic positive effect of the combination on the RBC parameters and eventually supports their antagonistic relationship for weight gain. OVA and C2 combination is inconclusive because of unavailable data on this combination treatment (table 2). DiRenzo et al. [26] demonstrated that citral inhibits the synthesis of retinoic acid but the mechanism still remains unknown. Menegola et al. [27] demonstrated the inhibitory effects of citral on retinoic acid synthesis. Beeman et al. [28] showed the blockage of initiation of murine odontogenesis in vitro by citral. Travlos et al. [29] studied the role of citral in carcinogenesis of microencapsulated citral in rats and mice. Overall, the descriptive statistics have demonstrated that increase in levels of standard complete blood count was attributed to treatment of the animals with citral. Analysis of variance statistics have shown that variability in changes of levels of standard complete blood count was also attributed to the treatment of the animals with citral.
OVA in combination with citral have strongly reversed the negative impact on weight gain by C1; however, the impact was to a lesser extent for C2 treatment; though not statistically significant. OVA and ATRA confirmed their posit ive synergism on WBC parameters. OVA reversed the negative effects of C1 on the RBC but his effect was not shown for the WBC parameter. However, C2 combination data is inconclusive due to unavailability (Table 3).
OVA+ATRA caused synergistic hypersensitivity, bronchoconstriction and lung congestion as compared to both controls. OVA+C1 showed an antagonistic interaction consistent with the improvement of lung pathology. OVA+C2 caused a synergistic damaging effect according to which the combination has inflicted more lung damage and impairment as compared to the two individual controls [30-38; Figures 1-5].
CONCLUSIONS
The study wass attempting to answer questions related to the paradox of retinoid-mediated therapy and the use of supraphysiologic exposure to ovalbumin, retinoids and Citrals as natural bioactive nutraceutical agents in supplementation or therapy. The study showed that there are variable pathologic responses from the interaction of ovalbumin, Citrals and retinoids and also showed that Citrals succeeded in reversing related tissue pathologies. OVA in combination with citral have strongly reversed the negative impact on weight gain by C1; however, the reversal impact was lower for C2 treatment though not statistically significant from effects by OVA or –control treatments. OVA and ATRA confirmed their positive synergism on WBC parameters. OVA reversed the negative effects of C1 on the RBC but this effect was not shown for the WBC parameter. However, C2 combination data is inconclusive due to unav ailability. OVA+ATRA caused synergistic hypersensitivity, bronchoconstriction and lung congestion as compared to both controls. OVA+C1 showed an antagonistic interaction consistent with the improvement of lung pathology. OVA+C2 caused a synergistic damaging effect according to which the combination has inflicted more lung damage and impairment as compared to the two as individual treatments. These findings warrants further investigation as to the actual role of these interactions in relation to chronic lung disease and the possibility of reversing retinoid-mediated pathologies in the Fisher rat model.
Figure 2.
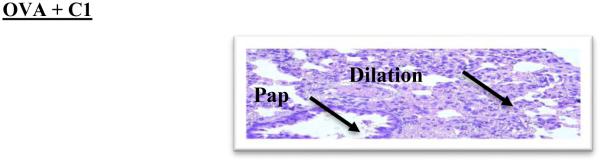
Ovalbumin Sensitized Lung Histopathological Display of Fischer 344 Rat Model.400x. As seen in Figure 2 (400x magnifications): (8A) OVA+Cl treatment to F344 rat lung portraying alveoli walls that appear thick, evident congestion, prevalent papillary projections but appearance change with decrease in surface area, cuboidal shaped epithelium instead of columnar shaped, constricted vessels and somewhat dilated alveoli; 400 x. OVA+ Cl
Figure 3.
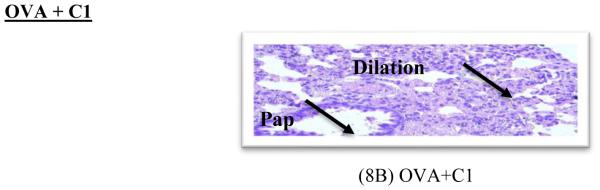
Ovalbumin Sensitized Lung Histopathological Display of Fischer 344 Rat Model. As seen in Figure 3 (400x magnifications): (8B) OVA+Cl treatment of the F344 rat lung portraying thick alveolar walls, evident congestion, prevalent papillary projections but appearance changes with decreased surface area, cuboidal shapes are presenting instead of columnar shaped epithelia, presence of constricted vessels and somewhat dilated alveoli. OVA+ATRA
ACKNOWLEDGMENTS
This research is supported by NIH/NCRR RCMI grant # G12-MD007581.
REFERENCES
- 1.McGowan SE. Contributions of Retinoids to the Generation and Repair of the Pulmonary alveolus. Chest. 2002;121:206S–208S. doi: 10.1378/chest.121.5_suppl.206s. [DOI] [PubMed] [Google Scholar]
- 2.Belloni PN, Garvin L, C-Ping Mao, Bailey-Healy I, Leaffer D. Effects of All-Trans-Retinoic Acid in Promoting Alveolar Repair. Chest. 2000;117:235S–241S. doi: 10.1378/chest.117.5_suppl_1.235s. [DOI] [PubMed] [Google Scholar]
- 3.Massaro GD, Massaro D. Retinoic Acid Treatment Abrogates Elastase-induced Pulmonary Emphysema. Nature Med. 1997;3:675–703. doi: 10.1038/nm0697-675. [DOI] [PubMed] [Google Scholar]
- 4.Chambone PA. A Decade of Molecular Biology of Retinoic Acid Receptors. FASEB J. 1996;10:940–954. [PubMed] [Google Scholar]
- 5.Chytil F. Retinoids in Lung Development. FASEB J. 1996;10:986–992. doi: 10.1096/fasebj.10.9.8801181. [DOI] [PubMed] [Google Scholar]
- 6.MMcGowan SE, Doro MM, Jackson SK. Endogenous Retinoids Increase Perinatal Elastin Gene Expression in Rat Lung Fibroblasts and Fetal Explants. Am. J.Physiol. Lung Cell Mol. Physiol. 1997;273:L410–L416. doi: 10.1152/ajplung.1997.273.2.L410. [DOI] [PubMed] [Google Scholar]
- 7.Massaro GD, Massaro D. Retinoic Acid Treatment Partially reverses Failed Septation in Rats and Mice. AM. J. Physiol. 2000;278:L955–L960. doi: 10.1152/ajplung.2000.278.5.L955. [DOI] [PubMed] [Google Scholar]
- 8.Morabia A, Menkes M, Comstock G, et al. Serum Retinol and Airway Obstruction. AM. J. Epidemiol. 1990;132:77–82. doi: 10.1093/oxfordjournals.aje.a115645. [DOI] [PubMed] [Google Scholar]
- 9.Paiva S, Goday I, Vannucchi H, et al. Assessment of Vitamin A Status in Chronic Obstructive Pulmonary Disease Patients and Healty Smokers. Am. J. Clin. Nutr. 1996;64:929–934. doi: 10.1093/ajcn/64.6.928. [DOI] [PubMed] [Google Scholar]
- 10.Napoli J. Retinoic Acid Biosynthesis and Metabolism. FASEB J. 1996;10:993–1001. doi: 10.1096/fasebj.10.9.8801182. [DOI] [PubMed] [Google Scholar]
- 11.Haq R, Pfahl M, Chytil F. Retinoic Acid Affects the E xpression of Nuclear Retinoic Acid Recptors in Tissues of Retinol Deficient Rats. Proc Natl Acad Sci USA. 1991;88:8272–8276. doi: 10.1073/pnas.88.18.8272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zachman R. Role of Vitamin A in Lung Developent. J Nutr. 1995;125:1934 S–1638S. doi: 10.1093/jn/125.suppl_6.1634S. Suppl. [DOI] [PubMed] [Google Scholar]
- 13.Liu R, Harvey C, McGowan S. Retinoic Acid increase Elastin in Rat Lung Fibroblasts Cultures. Am J Physiol. 1993;265:L430–L437. doi: 10.1152/ajplung.1993.265.5.L430. [DOI] [PubMed] [Google Scholar]
- 14.Okabe T, Yorifuji H, Yamada E, et al. Isolation and characterization of Vitamin A Storing Lung Cells. Exp Cell Res. 1984;154:125–135. doi: 10.1016/0014-4827(84)90673-6. [DOI] [PubMed] [Google Scholar]
- 15.Schuh TJ, Kraft J, Hall BL. v-erbA and Citral Reduce The Teratogenic Effects of all-trans Retinoic Acid and Retinol, Respectively, in Xenopus Embryogenesis. Development. 1993;119:785–798. doi: 10.1242/dev.119.3.785. [DOI] [PubMed] [Google Scholar]
- 16.Tanumihardjo SA, Penniston KL. The Acute and Chronic Toxic Effects of Vitamin A. American Journal of Clinical Nutrition. 2006;83:191–201. doi: 10.1093/ajcn/83.2.191. [DOI] [PubMed] [Google Scholar]
- 17.Massaro GD, Massaro D. Postnatal Treatment with Retinoic Acid Increases the Number of Pulmonary Alveoli in Rats. Am J Physiol. 1996;270:L305–L310. doi: 10.1152/ajplung.1996.270.2.L305. [DOI] [PubMed] [Google Scholar]
- 18.Swee M, Parks W, Pierce R. Developmental regulation of Elastin Production. J Biol Chem. 1995;270:14899–14906. doi: 10.1074/jbc.270.25.14899. [DOI] [PubMed] [Google Scholar]
- 19.Austead G. Steroids, Retinoids and Wound Healing. Adv Wound Care. 1998;11:277–285. [PubMed] [Google Scholar]
- 20.Hunt T. Vitamin A and Wound Healing. J Am Acad Dermatol. 1986;15:817–821. doi: 10.1016/s0190-9622(86)70238-7. [DOI] [PubMed] [Google Scholar]
- 21.Tepper J, Pfeiffer J, Aldrich M, et al. Can Retinoic Acid Ameliorate the Physiologic and Morphologiceffects of elastase instillation in the Rat. Chest. 117(suppl 1):242S–244S. doi: 10.1378/chest.117.5_suppl_1.242s. [DOI] [PubMed] [Google Scholar]
- 22.Maple S, Mendelssohn C, Cardoso WV. Regulation of retinoic acid signaling during lung morphogenesis. Development. 2000;127:3057–3067. doi: 10.1242/dev.127.14.3057. [DOI] [PubMed] [Google Scholar]
- 23.Mao JT, Goldin JG, Ermand J, et al. A pilot study of all-trans retinoic acid for the treatment of human emphysema. Am .J Respir. Crit Care Med. 2002;165:718–723. doi: 10.1164/ajrccm.165.5.2106123. [DOI] [PubMed] [Google Scholar]
- 24.Farah I, Holt-Gray C, Brown R. Impact of supra-physiologic retinoids on ovalbumin-sensit26. ized F344 lung tissue and reversal of related pathology by citral. Biomed. Sci. Instrum. 2011;47:195–200. [PMC free article] [PubMed] [Google Scholar]
- 25.Ilayperuma I. Effects of Intraperitoneal Administration of Citral on Male Reproductive Organs in the Rat. Galle Medical Journal. 2008;13(1):29–32. [Google Scholar]
- 26.Di Renzo F, Broccia ML, Giavini E, Menegola E. Citral, an inhibitor of retinoic acid synthesis, attenuates the frequency and severity of bronchial arch abnormalities induced by triazole-derivative fluconazole in rat embryos cultured in vitro. Reproductive Toxicology. 2007;24(3-4):326–32. doi: 10.1016/j.reprotox.2007.07.012. [DOI] [PubMed] [Google Scholar]
- 27.Nenegola E, Giavini E, DiRenzo F, Broccia MI. Citral, an inhibitor of retinoic acid synthesis, attenuates the frequency and severity of bronchial arch abnormalities induced by triazole-derivative fluconazole in rat’s embryos culture in vitro. Reproductive Toxicology. 2007;24(3):326–332. doi: 10.1016/j.reprotox.2007.07.012. Y. [DOI] [PubMed] [Google Scholar]
- 28.Beeman CS, Berndt W, Kronmillera JE, Nguyen T. Blockade of the initiation of murine odontogeness in vitro by citral, an inhibitor of endogenous retinoic acid synthesis. Archives of Oral Biology. 1995;4:7. doi: 10.1016/0003-9969(95)00015-h. [DOI] [PubMed] [Google Scholar]
- 29.Travlos GS, Ress NB, Orzech DP, Maronpot RR, Johnson JD, Hejtmancik MR, Haseman JK, Hailry JR, Bucher JR. Carcinogenesis studies of microencapsulated citral in rats and mice. Society of Toxicology. 2003;71:198–206. doi: 10.1093/toxsci/71.2.198. [DOI] [PubMed] [Google Scholar]
- 30.McGowan S, Holmes A, Smith J. Retinoic acid reverses the airway hyperresponsiveness but not the parenchymal defect that is associated with vitamin A deficiency. American Journal of Physiology: Lung Cellular & Molecular Physiology. 2004;30(2):L437–L444. doi: 10.1152/ajplung.00158.2003. [DOI] [PubMed] [Google Scholar]
- 31.Belloni PN, Garvin L, Ping C, Mao I, Bailey-Healy, Leaffer D. Effects of All-Trans-Retinoic Acid in Promoting Alveolar Repair. Chest. 2000;117:235S–241S. doi: 10.1378/chest.117.5_suppl_1.235s. [DOI] [PubMed] [Google Scholar]
- 32.Massaro GD, Massaro D. Retinoic Acid Treatment Abrogates Elastase-induced Pulmonary Emphysema. Nature Med. 1997;3:675–703. doi: 10.1038/nm0697-675. [DOI] [PubMed] [Google Scholar]
- 33.Chytil F. The lungs and vitamin A. American Journal of Physiology. 1992;262:L517–L527. doi: 10.1152/ajplung.1992.262.5.L517. [DOI] [PubMed] [Google Scholar]
- 34.Tanumihardjo SA, Penniston KL. The Acute and Chronic Toxic Effects of Vitamin A. American Journal of Clinical Nutrition. 2006;83:191–201. doi: 10.1093/ajcn/83.2.191. [DOI] [PubMed] [Google Scholar]
- 35.Hunt T. Vitamin A and Wound Healing. J Am Acad Dermatol. 1986;15:817–821. doi: 10.1016/s0190-9622(86)70238-7. [DOI] [PubMed] [Google Scholar]
- 36.Tepper J, Pfeiffer J, Aldrich M, et al. Can Retinoic Acid Ameliorate the Physiologic and Morphologic effects of elastase instillation in the Rat. Chest. 2000;117(suppl 1):242S–244S. doi: 10.1378/chest.117.5_suppl_1.242s. [DOI] [PubMed] [Google Scholar]
- 37.Malpe S, Mendelssohn C, Cardoso WV. Regulation of retinoic acid signaling during lung morphogenesis. Development. 2000;127:3057–3067. doi: 10.1242/dev.127.14.3057. [DOI] [PubMed] [Google Scholar]
- 38.Mao JT, Goldin JG, Ermand J, et al. A pilot study of all-trans retinoic acid for the treatment of human emphysema. Am. J Respir. Crit Care Med. 2002;165:718–723. doi: 10.1164/ajrccm.165.5.2106123. [DOI] [PubMed] [Google Scholar]