

Abstract
Osseous choristoma is a normal bone tissue in an ectopic position. In the oral region lingual localization occurs more frequently and the mass is generally localized on the dorsum of the tongue. Definitive diagnosis is obtained only after histopathologic examination. The etiology remains already debatable. The treatment of choice is surgical excision. In this paper we present a case of tongue osseous choristoma and a review of the literature.
1. Introduction
The term choristoma is used to describe the growth of normal tissue in an abnormal position. Choristoma of the mouth may be composed of several different tissue types. These include bone, cartilage, gastric mucosa, glial tissue, and tumor-like masses of sebaceous glands. Osseous choristoma is a well circumscribed benign growth of normal, mature osseous tissue in ectopic sites.
Osseous choristoma of the tongue is an extremely rare condition, of which only 66 cases have been reported in the literature till now. The osseous histotype is the most frequently described among choristomas. In the oral region lingual localization occurs more frequently and the mass is generally localized on the dorsum of the tongue. The etiology remains already debatable. The treatment of choice is surgical excision.
2. Case Report
A 10-year-old girl was referred to our ENT unit for a whitish 1 cm sessile swelling of the paramedian dorsum of the tongue, near foramen caecum (Figure 1). Upon palpation this not ulcerated lesion was firm. The patient did not complain of any symptom for many years. In the last two months she complained of lump. The mother of the girl reported that she noticed the little swelling since first months of life. She underwent neck ultrasound that showed a normal thyroid gland in shape and position. Although she was paucisymptomatic we proposed and performed a surgical excision of the lesion in order to obtain a histological diagnosis. Histological examination described an osseous choristoma of the tongue. The specimen was totally included for histological examination. Histologically, it appeared as a polypoid nodule of cortical bone tissue (mm 10 in maximum diameter) beneath the mucous membrane of the tongue covered by orthokeratinised squamous epithelium. The bone tissue was lamellar type with well developed haversian systems. The bone tissue was with sharply demarcated edges and in the surrounding tissue there was no inflammation or scar tissue (Figure 2).
Figure 1.

Paramedian dorsum of the tongue choristoma.
Figure 2.
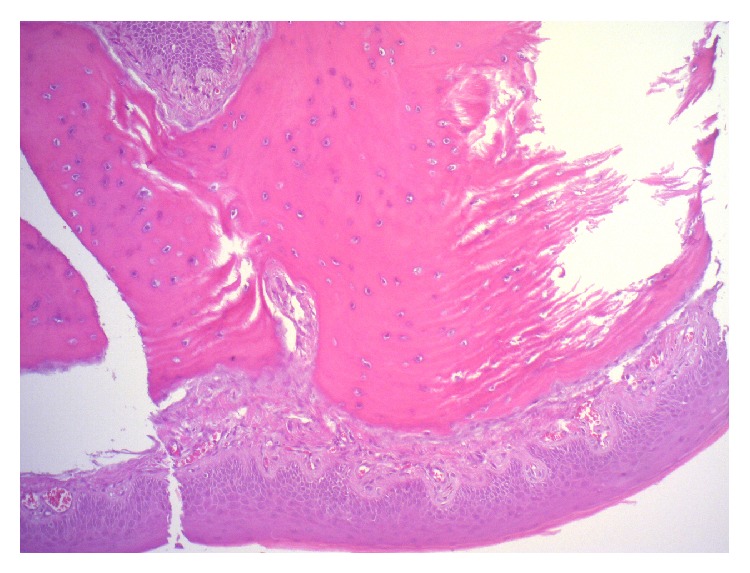
Histological examination shows mature lamella lined by mucous membrane of the tongue.
After 1-year follow-up there is no evidence of recurrence.
3. Discussion and Review of the Literature
The term osseous choristoma was introduced by Krolls et al. in 1971 [1]. By definition it is a growth of normal tissue in an abnormal position. Choristoma of the mouth may be composed of several different tissue types. These include bone, cartilage, gastric mucosa, glial tissue, and tumor-like masses of sebaceous glands [2, 3].
Osseous choristoma of the tongue is an extremely rare condition. In the literature 66 cases have been described (Table 1) [1–45]. In our review the patient age ranged from five to seventy-three years (mean age: 28,7 years), with the majority of the patients being in the second or third decades of life. Choristomas of the tongue occur more frequently in women (M:F 16:44).
Table 1.
| Author | Age (y)/sex | Location | Size | Symptom | |
|---|---|---|---|---|---|
| 1 | Cataldo et al. [4] | 39/F | Posterior tongue | 1 cm Ø | None |
| 2 | Begel et al. [5] | 22/F | Area of CP | 1 × 0,5 cm | Dysphagia |
| 3 | Jahnke and Daly [6] | 22/F | Posterior to CP | 1,3 × 0,8 × 0,7 cm | Lump |
| 4 | Kaye [7] | 26/F | Base of the tongue | 1 × 1 cm | Lump |
| 5 | Goldberg et al. [8] | 65/M | Lateral border | 1 cm Ø | None |
| 6 | Krolls et al. [1] | 22/F | Anterior to CP | 0,75 cm Ø | None |
| 7 | 23/M | Area of FC | Un. | Un. | |
| 8 | 73/M | Posterior tongue | Un. | Gagging | |
| 9 | 9/F | Area of FC | Un. | Gagging | |
| 10 | 25/F | Posterior tongue | 0,5 cm Ø | Un. | |
| 11 | 11/F | Posterior tongue | 2 cm Ø | Un. | |
| 12 | 23/M | Area of CP | 0,5 × 0,5 × 0,5 cm | None | |
| 13 | 39/M | Area of CP | 0,6 × 0,6 cm | None | |
| 14 | Singh and Doyle [9] | 14/F | Left border | Un. | Un. |
| 15 | 22/F | Area of CP | 0,5 cm Ø | None | |
| 16 | McClendon [10] | 15/F | Area of FC | 1,4 × 0,6 × 0,5 cm | None |
| 17 | 20/M | Right border | 0,7 cm Ø | None | |
| 18 | 46/F | Area of FC | 0,6 cm Ø | None | |
| 19 | Patel and Dane [11] | 42/M | Lateral border | 1 cm Ø | None |
| 20 | Engel and Cherrick [12] | 31/M | Mid third right border | 2 cm Ø | Lump |
| 21 | Busuttil [13] | 8/F | Left border | Pea-sized | Lump |
| 22 | Ohno et al. [14] | Un. | Dorsum of the root of the tongue | Un. | Un. |
| 23 | Sugita et al. [15] | Un. | Un. | Un. | Un. |
| 24 | Sato et al. [16] | Un. | Un. | Un. | Un. |
| 25 | Esguep et al. [17] | 63/F | Right border | 0,5 cm Ø | Lump |
| 26 | Wasserstein et al. [18] | 50/F | Mid third | 1,5 × 0,75 cm | Lump |
| 27 | Shimono et al. [19] | 37/F | Area of FC | 1,5 × 1,5 × 0,7 cm | Lump |
| 28 | Main [20] | 54/F | Posterior to FC | 1,5 cm Ø | Lump |
| 29 | Sheridan [21] | 20/F | Anterior to CP | 1 cm Ø | Lump |
| 30 | Cabbabe et al. [22] | 5/F | Base of tongue | 0,6 × 0,5 × 0,3 cm | Lump |
| 31 | Nash et al. [23] | 31/M | Right border | 2,5 cm Ø | None |
| 32 | Weitzner [24] | 52/F | Mid third | Small nodule | None |
| 33 | 25/F | Posterior tongue | 0,8 × 0,4 × 0,4 cm | Lump | |
| 34 | 27/F | Posterior tongue | 0,8 × 0,7 × 0,3 cm | Lump | |
| 35 | Tohill et al. [25] | 31/F | Anterior to CP | 1 × 0,8 × 0,7 cm | None |
| 36 | Markaki et al. [26] | 25/F | Posterior to CP | 0,8 × 0,4 × 0,3 cm | Lump |
| 37 | Van Der Wal and van der Waal [27] | 31/F | Area of FC | 1 cm Ø | Lump |
| 38 | Cannon and Niparko [28] | 51/F | Posterior tongue | Un. | Lump |
| 39 | Bernard et al. [29] | 21/F | Area of FC | 2 cm Ø | Lump |
| 40 | Maqbool et al. [30] | 8/F | Right vallecula | 5 × 4 cm | Dysphagia, distress |
| 41 | Lutcavage and Fulbright [31] | 11/F | Posterior to FC | 1 cm Ø | Lump |
| 42 | Ishikawa et al. [32] | 53/F | Area of FC | 0,8 cm Ø | Foreign body sensation |
| 43 | 5/F | Anterior to CP | 3 mm Ø | Lump | |
| 44 | Lee et al. [33] | 35/M | Lateral border | Un. | Lump |
| 45 | Ngeow et al. [34] | Un. | Un. | Un. | Un. |
| 46 | Manganaro [35] | Un. | Un. | Un. | Un. |
| 47 | Vered et al. [36] | 44/M | Left border | 0,7 × 0,7 × 0,6 cm | Gagging, nausea, and dysphagia |
| 48 | 27/M | Posterior to CP | 1 × 0,5 cm | Pain, gagging | |
| 49 | Supiyaphun et al. [3] | 28/F | Area of FC | 1 × 0,8 × 0,6 cm | Throat irritation |
| 50 | 25/F | Area of FC | 0,7 × 0,5 × 0,4 cm | Lump | |
| 51 | 9/F | Area of FC | 0,7 × 0,6 × 0,5 cm | None | |
| 52 | 35/F | Area of FC | 0,7 × 0,5 × 0,5 cm | None | |
| 53 | 27/F | Area of FC | 1,2 × 0,9 × 0,6 cm | None | |
| 54 | 21/F | Area of FC | 1,5 × 1,3 × 0,8 cm | Lump | |
| 55 | 22/M | Area of FC | 0,9 × 0,8 × 0,6 cm | None | |
| 56 | 19/F | Area of FC | 1,1 × 0,7 × 0,7 cm | None | |
| 57 | Lin et al. [37] | Un. | Posterior tongue | Un. | Un. |
| 58 | Horn et al. [38] | 11/F | Posterior tongue | Un. | Lump |
| 59 | Benamer and Elmangoush [39] | 14/F | Mid third | 1 cm Ø | Lump |
| 60 | Carvalho et al. [40] | 22/F | Posterior tongue | 1 cm Ø | None |
| 61 | Andressakis et al. [2] | 72/M | Anterior to CP | 1,5 × 1 cm | Pain dysphagia |
| 62 | Naik et al. [41] | 25/F | Posterior tongue | 1,2 × 1,1 × 0,5 cm | Lump |
| 63 | Chen et al. [42] | 57/F | Posterior tongue | 1 cm Ø | Lump, dysphagia, and odynophagia |
| 64 | Spencer and Reed [43] | 11/M | Posterior tongue | 1,1 × 0,9 × 0,6 cm | None |
| 65 | Lin et al. [44] | 15/M | Area of FC | 0,5 × 0,5 cm | Lump |
| 66 | Qin et al. [45] | Un. | Un. | Un. | Un. |
| 67 | Present case | 10/F | Anterior to FC | 1 cm Ø | Lump |
(CP: circumvallate papillae, FC: foramen caecum, and Un.: unknown).
The most frequent affected region is the posterior third of the tongue dorsum near to the foramen caecum and circumvallate papillae. Pathogenesis of choristoma is still unknown and remains already debatable. Several theories tried to explain the pathogenesis of this disease. Some authors suggested that remnants of the undescended thyroid tissue might produce an osseous lesion but in some rare case choristoma is localized not in midline but on the border of the tongue [46]. In these cases some authors [36, 47] suggested a traumatic pathogenesis. They consider that the posterior third of the tongue is site of traumatic irritation by different lingual movement during swallowing and articulation and that frequent trauma leads to local inflammation with deposit of calcium. This theory cannot explain the formation of osseous choristoma, because this lesion contains fully developed bone with haversian system and not just calcifications.
In our opinion embryologic theory sounds true. Embryologically the tongue is a very complex structure. First and third branchial arches give rise, respectively, to the anterior two-thirds and posterior third of the tongue. It was suggested that pluripotential cells from these arches give origin to the osseous choristoma [5, 12].
Choristoma appears as a sessile or pedunculated mass usually covered by normal mucosa. The sizes of the lesions vary from 3 mm to 50 mm at their largest diameter.
Most of osseous choristoma of the tongue presents as a frequently asymptomatic swelling. The most frequent symptom is lump (46% of cases). Rarely patient complains of dysphagia (5 cases), gagging (4 cases), pain (4 cases), and nausea (1 case). Symptoms are correlated to lesion size, tumour localization, and surrounding tissues flogosis. The differential clinical diagnosis can be also based on the tumor location. When the lesion is located on the dorsal tongue near the foramen caecum we should consider in differential diagnosis benign tumours (hemangioma, lymphangioma, teratoma, hamartoma, and leiomyoma), thyroglossal duct cyst, lingual thyroid, mucocele, pyogenic granuloma, and malignant tumours (rhabdomyosarcoma, other sarcomas, and epidermoid carcinoma) [25]. Traumatic neuroma, neurofibroma, schwannoma, fibroma, and cartilaginous choristoma usually are located on the tongue margin. Pyogenic granuloma, mucocele, and cartilaginous choristoma frequently involve the anterior portion of the tongue. Nevertheless definitive diagnosis is obtained only after histopathologic examination.
The treatment of choice is surgical excision. Recurrence or malignant evolution has not been described.
Conflict of Interests
There are not present facts which may be considered as potential conflict of interests and significant financial contributions to this work. The authors wish to confirm that there is no known conflict of interests associated with this paper and there has been no significant financial support for this work that could have influenced its outcome.
References
- 1.Krolls S. O., Jacoway J. R., Alexander W. N. Osseous choristomas (osteomas) of intraoral soft tissues. Oral Surgery, Oral Medicine, Oral Pathology. 1971;32(4):588–595. doi: 10.1016/0030-4220(71)90324-0. [DOI] [PubMed] [Google Scholar]
- 2.Andressakis D. D., Pavlakis A. G., Chrysomali E., Rapidis A. D. Infected lingual osseous choristoma. Report of a case and review of the literature. Medicina Oral, Patologia Oral y Cirugia Bucal. 2008;13(10):E627–E632. [PubMed] [Google Scholar]
- 3.Supiyaphun P., Sampatanakul P., Kerekhanjanarong V., Chawakitchareon P., Sastarasadhit V. Lingual osseous choristoma: a study of eight cases and review of the literature. Ear, Nose and Throat Journal. 1998;77(4):316–325. [PubMed] [Google Scholar]
- 4.Cataldo E., Shklar G., Meyer I. Osteoma of the tongue. Archives of Otolaryngology. 1967;85(2):202–206. doi: 10.1001/archotol.1967.00760040204013. [DOI] [PubMed] [Google Scholar]
- 5.Begel H., Wilson H., Stratigos G., Zambito R. F. Osteoma of the tongue: report of case. Journal of Oral Surgery. 1968;26(10):662–664. [PubMed] [Google Scholar]
- 6.Jahnke V., Daly J. F. Osteoma of the tongue. Journal of Laryngology and Otology. 1968;82(3):273–275. doi: 10.1017/s0022215100068766. [DOI] [PubMed] [Google Scholar]
- 7.Kaye W. H. Osteoma of the tongue. Journal of Laryngology and Otology. 1968;82(3):269–271. doi: 10.1017/s0022215100068754. [DOI] [PubMed] [Google Scholar]
- 8.Goldberg A. F., Skuble D. F., Latronica R. J. Osteoma of the tongue: report of case. Journal of Oral Surgery. 1970;28(6, article 457) [PubMed] [Google Scholar]
- 9.Singh S. M., Doyle J. L. Osteoma of the tongue. Two case reports. The New York State Dental Journal. 1972;38(10):599–600. [PubMed] [Google Scholar]
- 10.McClendon E. H. Lingual osseous choristoma: report of two cases. Oral Surgery Oral Medicine and Oral Pathology. 1975;39(1):39–44. doi: 10.1016/0030-4220(75)90393-x. [DOI] [PubMed] [Google Scholar]
- 11.Patel R. M., Dane A. Pathologic quiz case 1. Osteoma of the tongue. Archives of Otolaryngology. 1975;101(4):266–268. [PubMed] [Google Scholar]
- 12.Engel P., Cherrick H. M. Extraosseous osteomas of the tongue. Journal of Oral Medicine. 1976;31(4):99–103. [PubMed] [Google Scholar]
- 13.Busuttil A. Clinical records. An osteoma of the tongue. Journal of Laryngology and Otology. 1977;91(3):259–261. doi: 10.1017/s0022215100083638. [DOI] [PubMed] [Google Scholar]
- 14.Ohno T., Yanbe H., Morii E., et al. Osseous choristoma situated on the dorusum of the root of the tongue: report of a case. Japanese Journal of Oral and Maxillofacial Surgery. 1981;27:1106–1109. [Google Scholar]
- 15.Sugita H., Yamamoto E., Sunakawa H., et al. Lingual osseous choristoma: report of a case. Japanese Journal of Oral and Maxillofacial Surgery. 1979;25:165–169. [Google Scholar]
- 16.Sato Y., Ozawa S., Aria N., Toguchi I., et al. Choristoma of the tongue: report of a case. Japanese Journal of Oral and Maxillofacial Surgery. 1981;27:93–95. [Google Scholar]
- 17.Esguep A., Espinoza E., Diaz G. Lingual osteoma. Journal of Oral Medicine. 1982;37(1):27–29. [PubMed] [Google Scholar]
- 18.Wasserstein M. H., SunderRaj M., Jain R., Yamane G., Chaudhry A. P. Lingual osseous choristoma. Journal of Oral Medicine. 1983;38(3):87–89. [PubMed] [Google Scholar]
- 19.Shimono M., Tsuji T., Iguchi Y., Yamamura T., Ogasawara M., Honda T., Nagai T. Lingual osseous choristoma. Report of 2 cases. International Journal of Oral Surgery. 1984;13(4):355–359. doi: 10.1016/S0300-9785(84)80045-9. [DOI] [PubMed] [Google Scholar]
- 20.Main D. M. Osseous polyp of the tongue: osteoma or choristoma? British Dental Journal. 1984;156(8):285–286. doi: 10.1038/sj.bdj.4805345. [DOI] [PubMed] [Google Scholar]
- 21.Sheridan S. M. Osseous choristoma: a report of two cases. British Journal of Oral and Maxillofacial Surgery. 1984;22(2):99–102. doi: 10.1016/0266-4356(84)90021-4. [DOI] [PubMed] [Google Scholar]
- 22.Cabbabe E. B., Sotelo-Avila C., Moloney S. T., Makhlouf M. V. Osseous choristoma of the tongue. Annals of Plastic Surgery. 1986;16(2):150–152. doi: 10.1097/00000637-198602000-00013. [DOI] [PubMed] [Google Scholar]
- 23.Nash M., Harrison T., Lin P.-T., Lucente F. E. Osteoma of the tongue. Ear, Nose and Throat Journal. 1989;68(1):63–65. [PubMed] [Google Scholar]
- 24.Weitzner S. Osseous choristoma of the tongue. Southern Medical Journal. 1986;79(1):69–70. doi: 10.1097/00007611-198601000-00020. [DOI] [PubMed] [Google Scholar]
- 25.Tohill M. J., Green J. G., Cohen D. M. Intraoral osseous and cartilaginous choristomas: report of three cases and review of the literature. Oral Surgery, Oral Medicine, Oral Pathology. 1987;63(4):506–510. doi: 10.1016/0030-4220(87)90268-4. [DOI] [PubMed] [Google Scholar]
- 26.Markaki S., Gearty J., Markakis P. Osteoma of the tongue. British Journal of Oral and Maxillofacial Surgery. 1987;25(1):79–82. doi: 10.1016/0266-4356(87)90161-6. [DOI] [PubMed] [Google Scholar]
- 27.van der Wal N., van der Waal I. Osteoma or chondroma of the tongue; A clinical and postmortem study. International Journal of Oral and Maxillofacial Surgery. 1987;16(6):713–717. doi: 10.1016/s0901-5027(87)80058-9. [DOI] [PubMed] [Google Scholar]
- 28.Cannon S. C., Niparko J. K. Pathologic quiz case 1. Lingual osteoma. Archives of Otolaryngology—Head & Neck Surgery. 1988;114(1):92–94. [PubMed] [Google Scholar]
- 29.Bernard P. J., Shugar J. M. A., Mitnick R., Som P. M., Meyer R. Lingual osteoma. Archives of Otolaryngology—Head and Neck Surgery. 1989;115(8):989–990. doi: 10.1001/archotol.1989.01860320099027. [DOI] [PubMed] [Google Scholar]
- 30.Maqbool M., Ahmad R., Ahmad R. Osteoma of the tongue: a rare cause of upper airway obstruction. Indian Pediatrics. 1992;29(11):1429–1431. [PubMed] [Google Scholar]
- 31.Lutcavage G. J., Fulbright D. K. Osteoma of the tongue. Journal of Oral and Maxillofacial Surgery. 1993;51(6):697–699. doi: 10.1016/s0278-2391(10)80274-5. [DOI] [PubMed] [Google Scholar]
- 32.Ishikawa M., Mizukoshi T., Notani K.-I., Iizuka T., Amemiya A., Fukuda H. Osseous choristoma of the tongue. Report of two cases. Oral Surgery, Oral Medicine, Oral Pathology. 1993;76(5):561–563. doi: 10.1016/0030-4220(93)90062-9. [DOI] [PubMed] [Google Scholar]
- 33.Lee B. J., Ahn S. K., Lee S. H., Lee W. S. Osteoma of the tongue. International Journal of Dermatology. 1994;33(8):602–603. [PubMed] [Google Scholar]
- 34.Ngeow W. C., Lian C. B., Shanmahasuntharam P. Osseous choristoma of the tongue. The Journal of Nihon University School of Dentistry. 1996;38(1):49–51. doi: 10.2334/josnusd1959.38.49. [DOI] [PubMed] [Google Scholar]
- 35.Manganaro A. M. Lingual osseous choristoma. General Dentistry. 1996;44(5):430–431. [PubMed] [Google Scholar]
- 36.Vered M., Lustig J. P., Buchner A. Lingual osteoma: a debatable entity. Journal of Oral and Maxillofacial Surgery. 1998;56(1):9–14. doi: 10.1016/S0278-2391(98)90906-5. [DOI] [PubMed] [Google Scholar]
- 37.Lin C. C., Chen C. H., Chen Y. K., Shen Y. H., Lin L. M. Osseous choristoma of oral cavity—report of two cases and review of the literature. The Kaohsiung Journal of Medical Sciences. 1998;14(11):727–733. [PubMed] [Google Scholar]
- 38.Horn C., Thaker H. M., Tampakopoulou D. A., De Serres L. M., Keller J. L., Haddad J., Jr. Tongue lesions in the pediatric population. Otolaryngology—Head and Neck Surgery. 2001;124(2):164–169. doi: 10.1067/mhn.2001.112304. [DOI] [PubMed] [Google Scholar]
- 39.Benamer M. H., Elmangoush A. M. Lingual osseous choristoma case report and review of literature. Libyan Journal of Medicine. 2007;2:46–48. doi: 10.4176/061211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Carvalho L., Aurora L., Rabello M. Coristoma osseo lingual. A. Apresentacao de caso. Revista Brasileira de Odontologia. 2008;65:152–154. [Google Scholar]
- 41.Naik V., Wan Faiziah W. A. R., Musa M. Choristoma of the base of the tongue. Indian Journal of Pathology and Microbiology. 2009;52(1):86–87. doi: 10.4103/0377-4929.44975. [DOI] [PubMed] [Google Scholar]
- 42.Chen Y.-K., Shen Y.-H., Lin Y.-J., Li Y.-T., Tsai K.-B., Lin L.-M. Buccal osseous choristoma in a 5-year-old boy. Oral Oncology Extra. 2005;41(9):198–201. doi: 10.1016/j.ooe.2005.05.006. [DOI] [Google Scholar]
- 43.Spencer J. C., Reed J. M. Lingual osseous choristoma. Proceedings of the Otorhinolaringology Annual Meeting; 2012. [Google Scholar]
- 44.Lin Y.-Z., Hung C.-H., Hung S.-H. Lingual osseous choristoma. Journal of Dental Sciences. 2013;8(1):94–95. doi: 10.1016/j.jds.2012.12.006. [DOI] [Google Scholar]
- 45.Qin D., Tang Y., Ren D., et al. Tongue osteocartilaginous choristoma: a case report. Hua Xi Kou Qiang Yi Xue Za Zhi. 2014;32:96–98. doi: 10.7518/hxkq.2014.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Monsarrat M. Osteome de la langue. Bulletin de la Société D’Anatomie. 1913;88:282–283. [Google Scholar]
- 47.Roy J. J., Klein H. Z., Tipton D. L. Osteochondroma of the tongue. Archives of Pathology. 1970;89(6):565–568. [PubMed] [Google Scholar]