

Abstract
Background:
Multiple sclerosis (MS) is a complex inflammatory disease of the central nervous system. Despite extensive research, its exact cause is unknown. One of the roles of nurses is discovery and prevention of factors related to the disease. This study aimed to investigate several food items concerning the etiology of MS in a population of Ahvaz (Iran).
Materials and Methods:
This case-control study was conducted on 113 MS patients and 113 healthy women. Food information was collected through interviews using a standard designed questionnaire. Statistical analysis was performed by adopting descriptive tests (mean, frequency, standard deviation) and inferential tests (Chi-square test, Fisher's exact test, logistic regression, and multivariate conditional logistic regression with a significance level of 0.05 and 95% confidence interval) through SPSS version 19.
Results:
Univariate regression analysis showed a significant association between MS and consumption of solid vegetable oil (P = 0.004), fruits (P = 0.002), vegetables (P = 0.016), dates (P = 0.02), and low-fat dairy (P = 0.009) more than five times a week. According to multivariate conditional logistic regression analysis, consumption of fruits (P = 0.03) and low-fat dairy (P = 0.04) more than five times a week had a protective role and solid vegetable oil consumption was significantly associated with a risk for MS (P = 0.01).
Conclusions:
This study suggests a protective role of consumption of fruits and low-fat dairy in MS and an increased risk of MS with solid vegetable oil consumption in Ahvaz (Iran).
Keywords: Case-control study, food items, Iran, multiple sclerosis, nursing
INTRODUCTION
Multiple sclerosis (MS) is a complex inflammatory disease of the central nervous system which leads to destruction of myelin and axons, and consequently, a progressive dysfunction of nervous system.[1] The age of disease onset is 20-40 years (it is a little higher in men than women), but the disease can occur at any age.[2] The trend of this disease is chronic and disabling, and in 80-85% of the cases, it has a relative recovery and relapse and leads to a reduction in individuals’ practical functions. This disease is defined by disturbances in cognitive function, paralysis of hands and legs, and loss of vision, as well as cerebral syndromes.[3] Presently, over 2.5 million people in the world are involved in MS.[2] Based on international MS prevalence categorization, Iran is in a low-risk region of MS (5-25 in 100,000 individuals),[4] although its prevalence has increased to 35.5-51.9 cases in 100,000 in the central areas of the country.[5] Despite extensive research, its exact etiology is unknown yet.[6] Based on epidemiology studies conducted all over the world, interaction of genetics and environmental factors is vastly associated with the incidence of this disease.[7,8] Among the effective environmental factors in disease etiology, nutrition, lifestyle, infectious diseases, and environmental and occupational contacts are considered important.[9] Several studies have been already conducted on the association between food habits and the diet, and MS, suggesting an association between consumption of animal saturated fats, dairy, vegetables and fruits, and MS.[9,10,11] The association between food habits and MS was investigated in several case-control studies, which yielded controversial results. Prospective studies show that neither saturated fats nor animal fats are associated with the risk of MS.[12] Meanwhile, some retrospective studies suggest the association between saturated fats consumption and the risk of MS.[11,13] Pekmezovic et al. suggested higher risk of MS resulted from consumption of high fat dairy (ice cream and butter).[13] On the other hand, consumption of fruits and vegetables has been considered in some research, possibly due to the effect of antioxidants on lowering the risk of MS.[13,14] Incidence of most MS cases has been ecologically reported to be associated to a specific food habit. Among these nutritional ecologic studies on following a specific food habit, Mediterranean diet is at the heart of attention. It is considered that this pattern can have a basic role in the modification strategies of inappropriate environmental changes.[15] Research showed an inverse association between MS and Mediterranean diet;[6] however, there are several interpretations from this food pattern.[16] In different Mediterranean regions, this pattern has also been under the influence of socioeconomic and cultural factors, religion, etc.[15] On the other hand, some studies suggest the effect of consumption of meat containing nitrate or smoked meat in increased risk of MS as well as protective effect of fish consumption and a diet containing vegetables in reduction of MS incidence.[6] Ahvaz, one of the eight major cities located in the south of Iran, is the center of Khuzestan province which is categorized as an MS low-risk region and has a lower prevalence of MS, compared to central cities in Iran.[17] MS is a multifactorial disease with various epidemiologic patterns in different populations. Khuzestan province has a more different ecologic and cultural condition, which necessities a specific regional food pattern, compared to the cities where MS is more prevalent. Nursing profession gives health services parallel to other medical professions in the direction of maintaining life, provision of health, prevention and control of diseases, and ultimately, treatment and rehabilitation. Nurses have a commitment and are responsible for any defect in individuals, families, groups and society. They play a key role in prevention and control of diseases, and can play their role through determination of priorities in health services provision and attaining epidemiological information to prevent diseases.[18,19]
Nurses have a role in health education, behavior change, and prevention of diseases, as well as in helping individuals access appropriate level of health. With respect to rapid increase of MS patients in the world and the numerous physical, psychological, and financial problems imposed on the patients and their families, discovering and prevention of accompanying factors of this disease may be helpful in controlling or delaying the occurrence of this disease. Most of the studies conducted to investigate the association between food patterns and MS are based in Europe and the western countries, which are different from Iran in climate, lifestyle, culture, and MS rate. As the food intake differs in various parts of the world, public food patterns of each country and their association with health and disease status should be separately evaluated. Investigation of food patterns reflects individuals’ food habits and behavior and can yield more details about patients’ nutritional etiology.[15] With regard to the scientific evidences in relation to food behaviors and MS and its suggested role in disease etiology, this study aimed to investigate the association between several food items and MS to have more details about nutritional etiology of MS.
MATERIALS AND METHODS
This is a case-control study. After obtaining permission from the ethics committee of Jundishapur University of Medical Sciences in Ahvaz, random sampling was conducted from Jan 2012 to July 2013 in Khuzestan MS Association. Subjects who met the inclusion criteria and were in the age group of 20-50 years were selected for the study group (MS disease diagnosed by a neurologist with McDonald criteria, mental ability to attend the study, having a medical record in Khuzestan MS Association, and residing in Ahvaz). After they were explained about the research goals and how to fill the questionnaire, the subjects in the study and control groups who were interested in participating in the study filled up and signed the consent form. All the subjects were ensured about the confidentiality of their data. Sample size was calculated with regard to previous studies.[5,9,20] A total of 126 subjects finally attended the study. Healthy subjects residing in Ahvaz with age, sex, and location of residence identical to the patients and willing to attend the research were selected in the control group.
Data collection tool consisted of two sections. The first section included 10 questions on demographic characteristics and disease-related information. The second section was related to the frequency of nutrient intake. Food items were measured based on modified FFQ Food Frequency Questionnaire[21] and the intake of nutrients in the form of food groups of meat, viscera, oils, dairy, vegetables, and fruits was assessed in a seven-item frequency as “daily”, “five times a week”, “two to three times a week,” “weekly”, “every 2 weeks”, “once a month”, and “seldom or never”. They were reported as frequency of consumption less than or more than five times a week. Content validity was evaluated for the questionnaire through review of scientific texts and articles and similar questionnaires on food frequencies. Some academic members were referred to evaluate and revise the questionnaire. Cronbach's α was calculated as 0.90 for the reliability of the questionnaire. The collection of data in the present study was conducted by filling the questionnaire through face-to-face and phone interviews conducted by the principal researcher or her assistant (a trained staff of Khuzestan MS Association). In case of physical disability preventing patient's attendance in MS Association, data were collected in both study and control groups through a face-to-face interview or phone call.
Data analysis was conducted using SPSS 19. The statistical tests adopted were descriptive tests (mean, percentage, frequency, and SD) and inferential tests of Chi-square, Fisher's exact test, logistic regression, and multivariate logistic regression at a significance level of 0.05 and 95% Confidence Interval (CI). Firstly, Odds Ratio (OR) and 95% CI were separately calculated for each variable through univariate logistic regression analysis. Then, food items which are associated with MS were entered into multivariate conditional logistic regression analysis model at a significance level of P < 0.05.
RESULTS
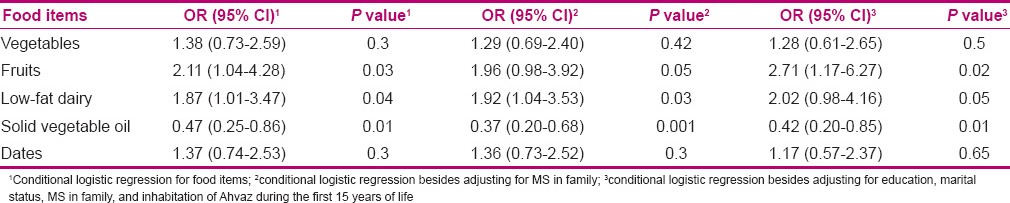
In this study, a total of 113 MS patients in the study group and the same number in the control group were enrolled. Table 1 shows the demographic characteristics of subjects in the study and control groups. Subjects’ mean age in the study and control groups was 33.67 (7.66) and 33.25 (7.62) years, respectively, and the mean age at which primary signs of the disease started was 27.57 (6.39) years. Based on the findings presented in Table 2, consumption frequency of solid vegetable oil was more in the study group compared to control, and consumption frequency of salad liquid oil and frying liquid oil was lower in MS patients compared to healthy individuals. Findings showed that consumption frequency of solid vegetable oil more than five times a week is accompanied with higher risk of MS (P = 0.002). Based on univariate logistic regression, this difference was significant (P = 0.004). Consumption of liquid salad oil (P = 0.01) and frying liquid oil more than five times a week was significantly associated with lower risk of MS (P = 0.02). Findings also showed that consumption of different nuts (walnut, almond, etc.) more than five times a week was not associated with the risk of MS (P = 0.12). Logistic regression showed no significant difference in the total consumption of oil and the risk of MS (P = 0.60, df = 5). Findings showed no significant difference in MS risk involvement in both groups concerning consumption of red meat (P = 0.14), poultry (chicken, etc.) (P = 0.17), fish (P = 0.22), and sausage and bologna (P = 0.37). Logistic regression showed no significant association between the total amount of consumed meat and the risk of MS (P = 0.81, df = 4). There was no significant association between consumption of animal viscera, including heart, liver and kidney, and head, and risk of MS (P > 0.05). Frequency of low-fat dairy consumption (milk, cheese, yoghurt, etc.) was more among healthy individuals than MS patients, may be shows its positive effect on reduction of MS risk (P = 0.003). Univariate logistic regression showed that this association was significant (P = 0.009), but no significant association between consumption of high-fat dairy (ice cream, cream, etc.) and MS risk was observed (P > 0.05). Logistic regression showed no significant association between total consumption of dairy and MS risk (P = 0.30, df = 2). With regard to the frequency of consumption of fruits and vegetables, the findings showed that consumption of fruits more than five times a week was more in healthy subjects compared to MS patients. Results showed an association between lowered risk of MS and consumption of fruits (P = 0.006), which was based on univariate logistic regression (P = 0.002). There was a significant association between vegetable consumption more than five times in a week and lower risk of MS (P = 0.001), which was based on univariate logistic regression (P = 0.016). No significant association was observed between consumption of cookies, cheetos, chips, and beans and MS (P > 0.05). Results showed lower risk of MS for consumption of dates (P = 0.01), which was significant based on univariate logistic regression (P = 0.02). The food items which had an association with MS based on univariate logistic regression analysis at a significance level of P < 0.05 (solid vegetable oil, liquid salad oil, frying liquid oil, low-fat dairy, fruits, vegetables, and dates) were ultimately entered in multivariate conditional logistic regression model [Table 3]. The obtained results showed that food items associated with MS risk included fruits, low-fat dairy, and solid vegetable oil that are consumed more than five times a week, in such a way that fruit (P = 0.03) and low-fat dairy consumption (P = 0.04) was associated with a reduction in risk of MS and consumption of solid vegetable oil more than five times a week (P = 0.01) was associated with a higher risk of MS. It should be noted that confounding variables such as marital status, history of MS in family members, education, and residing in Ahvaz in the first 15 years of life were controlled.
Table 1.
Demographic characteristics of the subjects in case and control groups

Table 2.
Frequency of consumption of various food groups and food items in groups
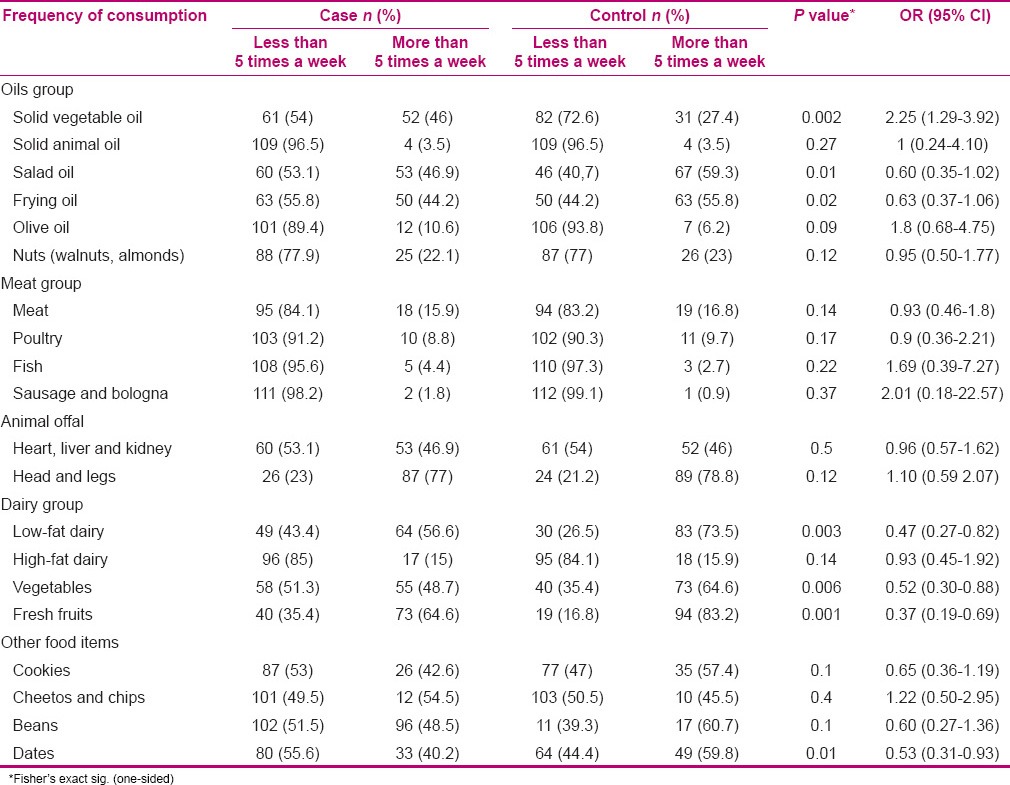
Table 3.
Conditional logistic regression models for food items associated with multiple sclerosis (113 cases vs. 113 controls)
DISCUSSION
Some studies revealed the association between consumption of animal fat foods and the risk of MS. It is argued that an increase in saturated animal fats and a reduction in polyunsaturated fatty acids may enhance the risk of MS.[22,23] Meanwhile, the results of prospective studies on dietary fats and MS show that neither saturated fats nor animal fats are associated with an increase in risk of MS, but the possible reverse association between intake of n-3 multiform unsaturated fat of linoleic acid and the risk of MS must not be ignored.[12] In other words, studies showed that an imbalance in the ratio of saturated and unsaturated fatty acids affects the sensitivity of myelin destructive elements. Protective effect of polyunsaturated unsaturated fatty acids, especially linoleic acid (omega-3), is possibly due to their immune-suppressive function.[24] On the other hand, saturated solid oils increase cholesterol and triglycerides, which can be the reason for the significant association between consumption of solid vegetable oil and risk of MS. Mashinchi et al. showed that most of the patients in Iran used solid vegetable oil before developing MS.[25] Schwarz and Leweling showed that consumption of saturated fatty acids can increase the risk of MS,[26] which is consistent with the results of the present study. Previous studies showed the association between high consumption of fatty acids and low intake of foods containing unsaturated fatty acids, especially polyunsaturated fatty acids, and the risk of MS.[23,25] Present study shows that consumption of liquid salad oil (sunflower, soya, etc.) is associated with a reduction in the risk of MS. Vegetable oils such as soya, walnut, sunflower, and corn oils contain essential fatty acids, monounsaturated fatty acids, and polyunsaturated fatty acids. Along with a reduction in intake of saturated fatty acids and an increase in intake of essential fatty acids existing in vegetable oils like soya, canola, wheat, walnut, and flax, use of their complements (complements of omega-3) can be effective on the prevention and amelioration of disease signs.[21,22] Also, including fresh nuts (walnut, hazelnut, almond, and pistachio) in the diet leads to an increase in the intake of essential fatty acids, which can be effective on the risk of MS as an appropriate food intake. Research on food habits as a potential factor showed that consumption of meat is associated with higher risk of MS.[27] Zorzon et al. showed that consumption of meat more than five times a week increases the risk of MS.[20] Pekmezovic et al. reported that constant consumption of beef, lamb meat, and chicken increased the risk of MS.[13] In other words, some ecologic studies all over the world support the role of red meat, pork, processed meat like smoked meat, and nitrate containing meat products (bologna and sausage) as the possible risk factors for MS,[6] which is not consistent with the present study. Berr et al.[28] and Zhang et al.,[12] in their prospective studies, showed no association between consumption of red meat, fish, sausage, and bologna and the risk of MS. Pekmezovic et al. showed no association between consumption of sausage and hot dog and the risk of MS,[13] which is consistent with the present study. The controversy in the role of consumption of various types of meat in MS can be due to the type of study (a retrospective study) and recall bias, which can influence the obtained results. The amount and type of meat consumed in various countries can be influenced by specific regional cultures, e.g. in the Mediterranean countries, consumption of red meat is less prevalent compared to other meat groups (poultry and fish) due to their culture and values (consumption of pork is a taboo), in comparison with western and European countries. On the other hand, difference in the amount of fat in the consumed meat should be noted and further studied.
The results on the association between dairy consumption and MS are controversial. Berr et al. in France and Zhang et al. showed no association between consumption of dairy and MS.[12,28] Meanwhile, research shows that consumption of saturated fats increases the risk of MS.[22,23] Pekmezovic et al. reported that consumption of high-fat dairy (ice cream and butter) increases the risk of MS.[13] Khadilkar et al. showed that daily consumption of milk or its products, especially high-fat dairy, increases the risk of MS.[11] This association was marginally significant in the present study. Two categorizations were considered for dairy products, i.e. low fat (milk, yoghurt, cheese, etc.) and high fat (ice cream, cream, butter, etc.), in the present study. Our obtained results show that consumption of low-fat dairy more than five times a week in MS patients and healthy individuals was 56.6% and 73.5%, respectively, which can support the suggested protective role of calcium level in nervous degenerative diseases[29] and reduced intake of saturated fatty acids. Consumption of animals’ viscera is associated with the risk of MS due to high level of saturated fatty acids in them. In the present study, a less number of subjects were found to consume animal viscera, which could have been due to the Iranian culture supporting limited consumption of animal viscera, the type of study (retrospective), and recalling bias. Results of some studies revealed the possible effect of antioxidants in the reduction of MS risk.[14,24,30] Fruits and vegetables are rich in various types of vitamins and minerals. Vitamins, especially, are the antioxidants whose protective role in the prevention of MS is suggested.[24] A case-control study conducted in Serbia showed that the frequency of consumption of fruits and vegetables was more in healthy individuals compared to MS patients,[13] which is in line with the present study. Results of a study conducted in Canada showed that constant consumption of fruits and vegetables has a protective effect on MS and consumption of fruit juice and vitamin C is significantly associated with MS.[24] Johnson reported on the role of gradual decrease of zinc, magnesium, selenium and vitamins B2, B6, D, and E in MS, and argued that vitamin B6 balances intracellular nitric acid and extracellular magnesium and is essential for nitric acid release from the cells. Therefore, deficiency of these substances leads to increased production of intracellular nitric acid and its lowered release form the cells. Stored nitric acid combines with superoxide and forms peroxynitric acid, which is a strong free radical and causes destruction of myelin of nerves. Vitamin B2 is a cofactor for xanthine oxide whose deficiency increases the level of uric acid resulting in destruction of myelin. Finally, selenium and vitamin E prevent fat peroxidation.[31] A case-control study conducted in Canada on the effect of antioxidant vitamins, especially vitamin C, of fruits supported the protective effect of high consumption of fruits and vegetables on MS and reported an inverse significant association between vitamin C consumption and the risk of MS.[24] In the present study, the association between consumption of fruits and vegetables and MS was found to be significant in univariate regression analysis. Although the frequency of consumption of vegetables in healthy people was more than in MS patients, this association was not found to be significant in the analysis. Pekmezovic et al. showed no significant association between consumption of beans and cookies and the risk of MS,[13] which is in line with the present study. As the present study was retrospective, the data related to prior to involvement in MS are needed; therefore, recall bias was possible due to collecting the data by questionnaires and relying on patients’ memory. Patients’ physiological condition at the time of filling the questionnaire could have an effect on their response. In the present study, although the difference in intake of some food items was not statistically significant due to the low sample size consuming these items, it can support the possible effect of nutritional elements on the incidence of MS.
CONCLUSION
The protective effect of consumption of fruits and vegetables and a reduction in intake of saturated fatty acids, as an appropriate food pattern, has been confirmed in cardiovascular disease and cancer. These factors may affect the nervous system and act as antioxidants. The present study supports the protective role of consumption of common plants (fruits and vegetables) and low-fat dairy (milk, yoghurt, cheese, etc), as well as the role of common solid vegetable oil consumption in higher risk of MS incidence. The findings of the present study show existence of inappropriate food habits and behaviors in MS patients. With regard to the role of nurses in health education, this issue reveals the importance of giving attention to and emphasizing their role in health education with the goal of familiarizing the patients with appropriate food habits, which can act as a preventive factor for MS. On the other hand, Ahvaz has lower prevalence of MS due to its geographic and tropical climate conditions, but the present study yielded results similar to the studies conducted in other geographic areas on the consumption of fruits and vegetables and intake of low-fat dairy. It is recommended to conduct further studies in similar populations with a higher sample size to investigate this association more precisely. Investigations conducted in similar populations but in various geographic areas may help determination of the factors effective on reducing or increasing the risk of MS.
It is suggested to conduct such a study in the other provinces of Iran with different climatic conditions and food behaviors.
ACKNOWLEDGMENTS
This article has been extracted from a sponsored dissertation project approved in Ahvaz Jundishapur University of Medical Sciences and financial support was provided by this center. (NO-U90294). The authors greatly appreciate the cooperation of Khuzestan MS Association and Mrs. Nedamat for her kind coordination in sampling.
Footnotes
Source of Support: This paper was part of MSc. dissertation of Maryam Bagheri that has been financially supported by Ahvaz Jundishapur University of Medical Sciences (Grant No. U-90294)
Conflict of Interest: Nil.
REFERENCES
- 1.Hedström AK, Sundqvist E, Bäärnhielm M, Nordin N, Hillert J, Kockum I, et al. Smoking and two human leukocyte antigen genes interact to increase the risk for multiple sclerosis. Brain. 2011;134:653–64. doi: 10.1093/brain/awq371. [DOI] [PubMed] [Google Scholar]
- 2.Hauser SL, Goodin DS. Multiple sclerosis and other demyelinating diseases. In: Longo DL, Fauci A.S, Kasper D.L, Hauser S.L, Jameson J.L, Loscalzo J, editors. Harrison's principles of internal medicine. 18th ed. Vol. 2. New York: McGraw Hill; 2012. p. 3395. [Google Scholar]
- 3.Smeltzer S, Sholtis L, Smith D. 12th ed. New York: Williams and Wikims; 2010. Brunner and suddarth's. Text book of medical surgical nursing; p. 1345. [Google Scholar]
- 4.Ashtari F, Shaygannejad V, heidari F, Akbari M. Prevalence of Familial Multiple Sclerosis in Isfahan, Iran. J Isfahan Med Sch. 2011;29:9–15. [Google Scholar]
- 5.Alonso A, Cook SD, Maghzi AH, Divani A. A case-control study of risk factors for multiple sclerosis in Iran. Mult Scler. 2011;17:550–5. doi: 10.1177/1352458510397685. [DOI] [PubMed] [Google Scholar]
- 6.Lauer K. Environmental risk factors in multiple sclerosis. Expert Rev Neurother. 2010;10:421–40. doi: 10.1586/ern.10.7. [DOI] [PubMed] [Google Scholar]
- 7.Marrie RA. Environmental risk factors in multiple sclerosis aetiology. Lancet Neurol. 2004;3:709–18. doi: 10.1016/S1474-4422(04)00933-0. [DOI] [PubMed] [Google Scholar]
- 8.Ascherio A, Munger K. Epidemiology of multiple sclerosis: From risk factors to prevention. Semin Neurol. 2008;28:17–28. doi: 10.1055/s-2007-1019126. [DOI] [PubMed] [Google Scholar]
- 9.Silva KR, Alvarenga RM, Fernandez Y, Fernandez O, Alvarenga H, Thuler LC. Potential risk factors for multiple sclerosis in Rio de Janeiro: A case-control study. Arq Neuropsiquiatr. 2009;67:229–34. doi: 10.1590/s0004-282x2009000200011. [DOI] [PubMed] [Google Scholar]
- 10.Ghadirian P, Dadgstar B, Azani R, Maisonneuve P. A case-control study of the association between sociodemographic, lifestyle and medical history factors and multiple sclerosis. Can J Public Health. 2001;92:281–5. doi: 10.1007/BF03404961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Khadilkar SV, Sahni AO, Agarwal S. A case control study of environmental risk factors in Indians with multiple sclerosis. Neurol Asia. 2005;10:47–52. [Google Scholar]
- 12.Zhang SM, Willett WC, Hernán MA, Olek MJ, Ascherio A. Dietary fat in relation to risk of multiple sclerosis among two large cohorts of women. Am J Epidemiol. 2000;152:1056–64. doi: 10.1093/aje/152.11.1056. [DOI] [PubMed] [Google Scholar]
- 13.Pekmezovic TD, Tepavcevic DB, Mesaros ST, Basuroski IBD, Stojsavljevic NS, Drulovic JS. Food and dietary patterns and multiple sclerosis: A case-control study in Belgrade (Serbia) Italian Journal of Public Health. 2009;6:81–7. [Google Scholar]
- 14.Ascherio A, Munger KL. Environmental risk factors for multiple sclerosis. Part II: Noninfectious factors. Ann Neurol. 2007;61:504–13. doi: 10.1002/ana.21141. [DOI] [PubMed] [Google Scholar]
- 15.Saneie P, Azadbakh L. Methods to Evaluate Adherence to Mediterranean Diet: A Review on Epidemiologic Studies. J Isfahan Med Sch. 2012;30:1–18. [Google Scholar]
- 16.Tangney CC, Kwasny MJ, Li H, Wilson RS, Evans DA, Morris MC. Adherence to a Mediterranean-type dietary pattern and cognitive decline in a community population. Am J Clin Nutr. 2011;93:601–7. doi: 10.3945/ajcn.110.007369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sharafaddinzadeh N, Moghtaderi A, Majdinasab N, Dahmardeh M, Kashipazha D, Shalbafan B. The influence of ethnicity on the characteristics of multiple sclerosis: A local population study between Persians and Arabs. Clin Neurol Neurosurg. 2013;115:1271–5. doi: 10.1016/j.clineuro.2012.11.027. [DOI] [PubMed] [Google Scholar]
- 18.Stanhope M, Lancaster J. 6th ed. Mosby; 2004. Community and public health nursing; p. 8. [Google Scholar]
- 19.Stanhope M, Lancaster J. 2nd ed. Mosby; 2006. Foundations of nursing in the community; pp. 8–10. [Google Scholar]
- 20.Zorzon M, Zivadinov R, Nasuelli D, Dolfini P, Bosco A, Bratina A, et al. Risk factors of multiple sclerosis: A case-control study. Neurol Sci. 2003;24:242–7. doi: 10.1007/s10072-003-0147-6. [DOI] [PubMed] [Google Scholar]
- 21.Piamani F, Nazari AA, Noktehdan H, Mehran A, Sahraeian MA. Study of lifestyle in multiple sclerosis patients, Admitted to the MS Society of Tehran 2008. Yafteh. 2010;13:8–31. [Google Scholar]
- 22.Alter M, Yamoor M, Harshe M. Multiple sclerosis and nutrition. Arch Neurol. 1974;31:267–72. doi: 10.1001/archneur.1974.00490400081010. [DOI] [PubMed] [Google Scholar]
- 23.Schwarz S, Leweling H. Multiple sclerosis and nutrition. Mult Scler. 2005;11:24–32. doi: 10.1191/1352458505ms1119oa. [DOI] [PubMed] [Google Scholar]
- 24.Ghadirian P, Jain M, Ducic S, Shatensteind B, Morisset R. Nutritional factors in the aetiology of multiple sclerosis: A case-control study in Montreal, Canada. Int J Epidemiol. 1998;27:845–52. doi: 10.1093/ije/27.5.845. [DOI] [PubMed] [Google Scholar]
- 25.Mashinchi Sh, Ebrahimi-Mameghani M, Saberi A, Yousefzadeh SH. Pattern of diet and supplement consumption among multiple sclerotic patients pre and post diagnosis and their attitudes toward the effects of these parameters on disease progression. J Guilan Univ Med Sci. 2013;21:1–14. [Google Scholar]
- 26.Schwarz S, Leweling H. Multiple sclerosis and nutrition. Mult Scler. 2005;11:24–32. doi: 10.1191/1352458505ms1119oa. [DOI] [PubMed] [Google Scholar]
- 27.Gusev E, Boiko A, Lauer K, Riise T, Deomina T. Environmental risk factors in MS: A case-control study in Moscow. Acta Neurol Scand. 1996;94:386–94. doi: 10.1111/j.1600-0404.1996.tb00050.x. [DOI] [PubMed] [Google Scholar]
- 28.Berr C, Puel J, Clanet M, Ruidavets JB, Mas JL, Alperovitch A. Risk factors in multiple sclerosis: A population-based case-control study in Hautes-Pyrenees, France. Acta Neurol Scand. 1989;80:46–50. doi: 10.1111/j.1600-0404.1989.tb03841.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Emard JF, Thouez JP, Gauvreau D. Neurodegenerative diseases and risk factors: A literature review. Soc Sci Med. 1995;40:847–58. doi: 10.1016/0277-9536(94)00138-j. [DOI] [PubMed] [Google Scholar]
- 30.Bermejo Vicedo T, Hidalgo Correas FJ. Antioxidants: The therapy of the future? Nutr Hosp. 1997;12:108–20. [PubMed] [Google Scholar]
- 31.Johnson S. The possible role of gradual accumulation of copper, cadmium, lead and iron and gradual depletion of zinc, magnesium, selenium, vitamins B2, B6, D, and E and essential fatty acids in multiple sclerosis. Med Hypotheses. 2000;55:239–41. doi: 10.1054/mehy.2000.1051. [DOI] [PubMed] [Google Scholar]