

Abstract
Purpose
The combination of fibular hemimelia with congenital short femur worsens the limb length discrepancy which requires extensive femoral and tibial lengthening.
Patients and methods
Eight patients having unilateral lower extremity shortening presented to the National Institute of Neuromotor System, Egypt, between September 2008 and September 2010 and underwent single session femoral and tibial lengthening using Ilizarov ring external fixator technique.
Consolidation of the femoral and tibial required length gain was evident in the radiographic follow-up.
Conclusion
Extensive limb length discrepancy can be managed by simultaneous femoral and tibial lengthening.
Level of evidence
The study is type IV clinical evidence.
Keywords: Fibular hemimelia, Congenital short femur, Extensive limb length discrepancy
1. Introduction
Congenital fibular partial or complete deficiency or hemimelia exists in three types ranging from type I or fibular shortness, type II or partial fibular deficiency, to type III or complete fibular absence1 which is frequently associated with femoral shortness, anterior tibial bowing, knee valgus, ankle instability and equinus, foot valgus deformity and/or malformation, and limb length discrepency.2
The combination of type III complete fibular absence with Aitken class A congenital short femur with contained femoral head in the acetabulum,3 worsens the limb length discrepancy which may exceed 12 cm and require extensive femoral and tibial lengthening.4 Isolated lengthening of either the femur or the tibia separately requires multiple operations for lengthening achievement in several sittings which adds to the psychological and economic burden. The use of Ilizarov ring external fixator corticotomy distraction technique enables to restore the extremity length as well as to correct the deformity in a single sitting.5,6
The objective of treatment of such cases is to implement simultaneous femoral and tibial lengthening to restore limb equality and gait, to correct deformities, to shorten the treatment period, and to minimize the problems.
2. Patients and methods
Eight consecutive patients having unilateral lower extremity shortening caused by combined complete fibular hemimelia (type III) and congenital short femur (Aitken class A); with stable hip, knee, and ankle joints, no coxa vara, no genu valgus as evident clinically and by plain radiography, no foot malformation but with equinus deformity; presented to the National Institute of Neuromotor System, Imbaba, Egypt, between September 2008 and September 2010. The results of this group after at least two years follow-up were reported in September 2013 and revised in December 2013 using previous medical records, history, and physical and imaging examinations. The study fulfilled the Egyptian's ethics code of research.
2.1. Inclusion criteria
Only cases of combined complete fibular hemimelia (type III) with congenital short femur (Aitken class A), in absence of hip, knee, or ankle instability, hip or knee deformity, or foot malformation, above 14 years of age were included.
2.2. Exclusion criteria
Other cases of limb length discrepancy, types I or II fibular hemimelia, or types of fibular hemimelia not associated with congenital short femur, or associated with hip, knee, or ankle instability, coxa vara, or genu valgus, or foot anomaly, and cases less than 14 years of age were excluded.
2.3. Evaluation of cases
The age ranged from 14 to 18 years, with the mean age 16.5 years. They were 6 females and 2 males. The left lower limb was short in 6 female patients, but the right one was short in one of the male patients. The lower limb shortness ranged from 8 to 12 cm, with the mean shortness 10 cm, both femoral (mean 3.75 cm) and tibial (mean 6.25 cm) contribution (Table 1).
Table 1.
Case evaluation.
| Case no. | Age (years) | Gender | Side | Total shortness (cm) | Femoral shortness (cm) | Tibial shortness (cm) | Equinus deformity |
|---|---|---|---|---|---|---|---|
| 1 | 15 | Female | Left | 9 | 3 | 6 | 10° |
| 2 | 14 | Female | Left | 8 | 2 | 6 | 15° |
| 3 | 18 | Male | Left | 10 | 4 | 6 | 20° |
| 4 | 17 | Female | Left | 12 | 5 | 7 | 25° |
| 5 | 17 | Female | Left | 11 | 4 | 7 | 20° |
| 6 | 15 | Male | Right | 8 | 3 | 5 | 15° |
| 7 | 18 | Female | Left | 12 | 5 | 7 | 25° |
| 8 | 18 | Female | Left | 10 | 4 | 6 | 20° |
2.4. Previous treatment
All cases received conservative treatment for several years in the form of high heel ankle/foot orthoses (AFO) to achieve limb length equalization, but no previous surgical interference.
2.5. Imaging studies
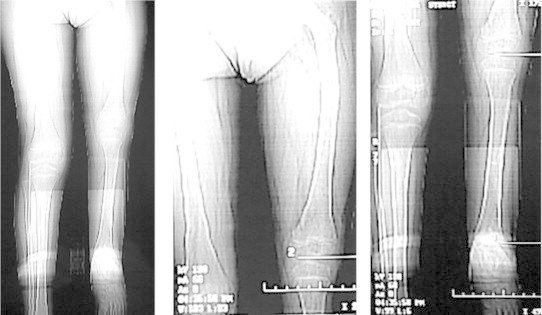
Anteroposterior and lateral weight-bearing plain radiographies pelvis to feet, with the short limb supported by appropriately sized wooden blocks, were taken prior to surgery to view the bony deficiency, deformity, and limb shortness (Fig. 1). Computerized tomography (CT) scanographies were taken to reveal the mechanical limb axes, and to accurately measure the amount of the limb shortness (Fig. 2).
Fig. 1.

Preoperative anteroposterior and lateral weight-bearing plain radiographies pelvis to feet.
Fig. 2.
Preoperative CT scanographies.
2.6. Preoperative fixator construct
Five appropriately sized rings of Ilizarov external fixator, two for the lower thigh and three for the leg, were assembled to the patient and prepared prior to surgery.
2.7. Operative treatment
Minimal skin incisions were made in the lower thigh and upper leg between the proposed ring sites to expose the lower femur and upper tibia respectively. Circumferential drill holes were made through the periosteum of the respective bones. The previously assembled ring fixator construct was applied to the patient using percutaneous 1.5 mm K-wires and 4 mm Schanz screws in accordance to the Ilizarov technique. After securing the external ring fixator apparatus and tensioning the wires, the drill holes were connected to complete the corticotomy using either Gigli saw or small sharp osteotome. The skin wound was closed. The equinus deformity was achieved at a later session after removal of the apparatus.
2.8. Postoperative treatment
Daily skin cleansing around the sites of entry and exit of the K-wires and entry of the Schanz screws using 0.9% saline solution or 70% ethyl alcohol was instructed to the patient or parents to minimize pin tract infection.
Distraction-lengthening was achieved by the patient or the parents a week after surgery at a rate of ¼ mm (or ¼ turn of the motor of the apparatus) every 6 h till the required length was gained (Fig. 3).
Fig. 3.
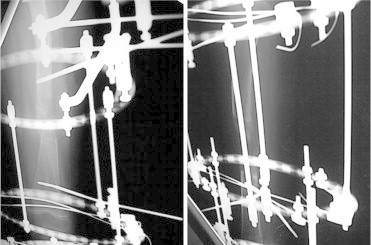
Follow-up plain radiographies in the regeneration phase.
Movements of the knee and ankle started within a few days but weight-bearing was postponed till the condition of the patient permitted.
Plain radiographic anteroposterior and lateral views were taken every 2 weeks to assess the bony callus regenerate, to be every 4 weeks in the consolidation period (Fig. 4). If the regenerate was not satisfactory either lengthening was discontinued or shortening was achieved in the reverse direction for a week, to restart lengthening later on till satisfactory regenerate in the follow-up plain radiography was regained.
Fig. 4.
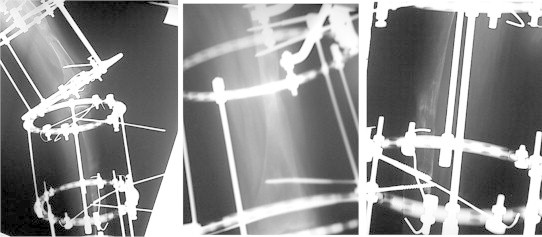
Follow-up plain radiographies in the consolidation phase.
During the lengthening procedure, ankle foot orthosis was applied to prevent worsening of the equinus deformity.
2.9. Operative correction of the equinus deformity
Achilles' tendon lengthening was achieved to correct the equinus deformity at the same session of removal of the apparatus. Above knee Plaster of Paris POP cast was applied for 6 weeks, after which physiotherapy to restore knee and ankle movements, full weight-bearing, and activities started.
3. Results
The lengthening procedure continued for 90–130 days (mean 110 days). The ring fixator apparatus was removed after 240–360 days (mean 300 days), at which time complete consolidation of the femoral and tibial required length gain was evident in the radiographic follow-up (Fig. 5). Limb length equalization which ranged from 8 to 12 cm was achieved in all the eight patients. All of the eight feet were plantigrade. The knee, ankle, and foot movements were restored. Pin track infection in the form of redness and serous discharge but without purulent discharge or pin loosening occurred in 3 stout female patients and one male patient. It was thoroughly controlled by systemic and local antibiotics for 1–2 weeks. Knee or ankle/foot instabilities or deformities never occurred (Table 2).
Fig. 5.
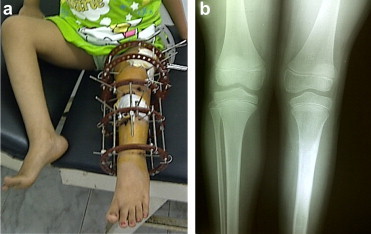
The final apparatus prior its removal (a), and the final radiograph after removal of the apparatus – Knees level and bones consolidated (b).
Table 2.
Results.
| Case no. | Lengthening duration (days) | Apparatus duration (days) | Total length gain (cm) | Femoral length gain (cm) | Tibial length gain (cm) | Pin track infection | Joint motion | Joint instability/deformity | Equinus deformity |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 100 | 270 | 9 | 3 | 6 | No | Restored | No | Corrected |
| 2 | 90 | 240 | 8 | 2 | 6 | Present | Restored | No | Corrected |
| 3 | 110 | 300 | 10 | 4 | 6 | Present | Restored | No | Corrected |
| 4 | 130 | 360 | 12 | 5 | 7 | No | Restored | No | Corrected |
| 5 | 120 | 330 | 11 | 4 | 7 | Present | Restored | No | Corrected |
| 6 | 95 | 240 | 8 | 3 | 5 | No | Restored | No | Corrected |
| 7 | 130 | 360 | 12 | 5 | 7 | Present | Restored | No | Corrected |
| 8 | 110 | 300 | 10 | 4 | 6 | No | Restored | No | Corrected |
4. Discussion
The unhappy combination of complete fibular hemimelia type III Achterman's and Kalamachi classification,1 with congenital short femur, even in the absence of hip, knee and ankle instability, coxa vara, genu valgus, or foot malformation, causes extensive lower limb shortness which may reach 12 cm or more.3
Basbozkurt et al7 (2005) and Herring8 (1992) advised early amputation and prosthesis of the foot for cases of limb length discrepancy more than 7.5 cm having the advantages of single surgery, early ambulation, short hospital stay, limb length equalization, and quick return to activities. However, amputation is irreversible, psychologically burdening, causes lack of proprioception sensation, and requires periodical change of the prosthesis.
The current study rejected the concept of amputation and adopted the use of Ilizarov ring external fixator corticotomy distraction technique in extensive limb length discrepancy which ranged from 8 to 12 cm, as an alternative to amputation, despite of the morbidity of the lengthening procedure like regenerate failure, pin tract infection, and the psychological burden of the apparatus. This is contrary to Basbozkurt et al7 (2005) who advised Ilizarov technique in limb shortness less than 5 cm. The current study adopted also simultaneous femoral and tibial lengthening to achieve limb equalization, correct deformities, shorten the duration of treatment, and minimize the problems. The equinus deformity was fully corrected at a separate session during removal of the apparatus by soft-tissue procedure without the necessity of bony interference.
The late onset of lengthening at the age of 14 or more rendered another lengthening session unnecessary according to Moseley's straight line graph for limb length discrepency.9
There was no regenerate failure, nor knee or ankle deformity or stiffness. The pin track infection happened in 4 cases and was thoroughly controlled by systemic antibiotics and local measures. The long duration of the apparatus was the only problem; however, the patients and/or parents were previously informed about it.
Choi et al10 (1990) reported repeated tibial lengthening using Wagner's technique with good outcome. The current study achieved single session femoral and tibial lengthening with similar outcome.
Miller et al11 (1992) reported satisfactory outcome in 12 fibular deficiency by Ilizarov technique. McCarthy et al12 (2000) achieved limb equalization and gait with minimal complications and good activity by Ilizarov technique; a result comparable to the current study.
In conclusion, the extensive limb length discrepancy in cases of combined complete (type III) fibular hemimelia and congenital short femur can be managed by single session simultaneous femoral and tibial lengthening using Ilizarov ring external fixator corticotomy distraction technique. However, the patients and/or the parents should have sufficient knowledge about the potential problems, the long duration of treatment, and the possibility of second surgery.
Conflicts of interest
The author has none to declare.
References
- 1.Achterman C., Kalamachi A. Congenital deficiency of the fibula. J Bone Joint Surg Br. 1979;61:133–137. doi: 10.1302/0301-620X.61B2.438260. [DOI] [PubMed] [Google Scholar]
- 2.Bohne W.L., Root L. Hypoplasia of the fibula. Clin Orthop Relat Res. 1977;125:107–112. [PubMed] [Google Scholar]
- 3.Grill F., Dungl P. Lengthening for congenital short femur: results of different methods. J Bone Joint Surg Br. 1991;73-B:439–447. doi: 10.1302/0301-620X.73B3.1670446. [DOI] [PubMed] [Google Scholar]
- 4.Paley D. Current techniques of limb lengthening (Review) J Pediatr Orthop. 1988;8:73–92. doi: 10.1097/01241398-198801000-00018. [DOI] [PubMed] [Google Scholar]
- 5.Dal Monte A., Donzelli O. Tibial lengthening according to Ilizarov in congenital hypoplasia of the leg. J Pediatr Orthop. 1987;7:135–138. doi: 10.1097/01241398-198703000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Catagni M.A. Management of fibular hemimelia using the Ilizarov method. Instr Course Lect. 1992;41:431–434. [PubMed] [Google Scholar]
- 7.Basbozkurt M., Yildiz C., Komurcu M., Demiralp B., Kurklu M., Atesalp S. Management of fibular hemimelia with Ilizarov circular external fixator. Acta Orthop Trumatul Turc. 2005;39:46–53. [PubMed] [Google Scholar]
- 8.Herring J.A. Symes amputation for fibular hemimelia: a second look in the Ilizarov era. Instr Course Lect. 1992;41:435–436. [PubMed] [Google Scholar]
- 9.Moseley C.F. Straight line graph for leg length discrepancies. J Bone Joint Surg Am. 1977;59:174–179. [PubMed] [Google Scholar]
- 10.Choi I.H., Kumar S.J., Bowen J.R. Amputation or limb lengthening for partial or total absence of the fibula. J Bone Joint Surg Am. 1990;72:1391–1399. [PubMed] [Google Scholar]
- 11.Miller L.S., Bell D.F. Management of congenital fibular deficiency by Ilizarov technique. J Pediatr Orthop. 1992;12:651–657. [PubMed] [Google Scholar]
- 12.McCarthy J.J., Glancy G.L., Chnag F.M., Eilert R.E. Fibular hemimelia: comparison of outcome measurements after amputation and lengthening. J Bone Joint Surg Am. 2000;82:1732–1735. doi: 10.2106/00004623-200012000-00006. [DOI] [PubMed] [Google Scholar]