

Abstract
Introduction: Striae distensae (SD) are a frequent skin condition for which treatment remains a challenge. The 1540-nm non-ablative fractional laser (Star Lux 500) has been shown to improve atrophic scars by increasing the amount of dermal collagen. To assess the safety and efficacy of the Star Lux 500 laser in the treatment of mature hypopigmented striae in Persian people (Striae Alba).
Methods: Ten women aged 26–50 years with SD and Fitzpatrick skin types III–V were enrolled in the study. The exclusion criteria were a history of keloids, photosensitivity and collagen, elastin disorders as well as history of other striae treatment within one year. The lesions were treated with non-ablative fractional laser 1540nm, and a total of four treatments were given at 4-week intervals. Clinical standard photographs were taken before each treatment. Also, patients were followed up at 3 months after the last treatment. Clinical improvement was assessed by comparing baseline and post-treatment photographs by two independent blinded physicians using grading scale. Treatment efficacy analysis was performed via the comparison between the images taken before and after each treatment session.
Results: There was a clinically appreciable improvement in striae ranging from 1 to 24%. A significant improvement in striae between the 16-week treatment and the 4-week treatment was identified (P<0.0001). Three months after the final treatment, patients showed noticeable improvement in the striae, compared with baseline (P<0.048). Mild post inflammatory hyperpigmentation was observed in one patient after the 8-week treatment and mild to moderate acne occurred in another patient after 4 weeks of treatment.
Conclusion: Therapy with Star lux 500 laser had clinically and statistically striae improvement with no adverse events. This may be a safe and an effective treatment modality for Striae Alba lesions.
Keywords: striae, laser, lesion
Introduction
Striae distensae (SD) are linear atrophic lesions that are initially erythematous (striae rubra) but over the time become atrophic, hypo pigmented and attain a white color (striae alba).1 SD is a common skin condition that is often a significant source of distress to those affected.2 These skin abnormalities are found in people of 5 to 50 years old, in both genders and all races.3,4 The etiology of SD is poorly understood but it is considered that genetic factors play more of a role.5 They may result from mechanical stress, such as weight changes, puberty, pregnancy, oral contraceptive use, topical steroids use 2,3,6 and Cushing's syndrome.4,6 They are usually located on the breasts, buttocks, thighs, knees in females and in males on the shoulder and lumbosacral areas.6
Histological findings have showed thin and flattened epidermis with loss of the rete ridges. At the level of the papillary dermis, thin and densely packed collagen bundles are arranged in parallel arrays horizontal to the epidermis .7
The atrophic appearance of striae is due to reduced amounts of fibrillin and elastin in the papillary dermis.1 Common treatments of striae rubra that have been used include topical 0.1% tretinoin8 and 585-nm pulsed dye laser treatment,9 also glycolic acid, ascorbic acid, Carbon Dioxide Laser (CO2) laser and eximer laser have been tried effectively.5, 10
In contrast, striae Alba has been difficult to treat and there are no satisfactory treatments options for all skin types.11
High incidence and treatment remain a challenge to stretch marks and more study is needed to find the most effective treatment. The 1540-nm non-ablative fractional laser (Star Lux 500) is the first laser with Food and Drug Administration (FDA) approval for stretch marks treatment.12 This study was performed to evaluate the safety and efficacy of the Star Lux 500 laser in the treatment of mature Striae Alba in Persian people.
Methods
This prospective pilot clinical before-after single center study was approved by the institutional review board of Shahid Beheshti University of Medical Science. Verbal and written informed consent was obtained from each patient. Patients with striae alba were enrolled to the study with the inclusion criteria of female, aged 18- 50 years, Fitzpatrick skin type III-V. The exclusion criteria were a history of keloids, photosensitivity and collagen and elastin disorders. Patients with history of topical, oral retinoid use and other striae treatment within one year of the study entry were also excluded. The lesion was initially identified with marked area 10*10 cm. The lesions were treated with Star lux 500 laser (Palomar's non-ablative fractional laser 1540nm, XD Microlens) with energy settings from 50 to 70 J/cm2 . The patients received treatment for selected area at baseline (week 0) followed by once a month for 3 months. Clinical standard photographs were taken before each treatment with canon power shot SX-200 camera. Also, patients were followed up at 3 months after the last treatment. Clinical improvement was assessed by comparing baseline and post-treatment photographs by two independent blinded dermatologists using grading scale. (I: no improvement (0%), II: poor (1-24%), III: fair (25% to 64%), IV: good (65% to 94%) and V: (95% to 100%) excellent improvement). Any side effects (erythema, blistering, keloid, hyperpigmentation or scarring) were recorded. All statistical analyses were carried out using SPSS 16 (Statistical Package for the Social Sciences). Spearman correlation test were used for assessing the linear correlation. The statistical significance was accepted for p-values less than 0.05.
Results
Ten women aged 26–50 years (mean age of 30.8±7 years) with striae distensae and Fitzpatrick skin types III–V were enrolled in the study. The duration of striae ranged from 4 to 15 years (average duration: 8.3±3.4 years). The cause of the striae varied from weight gain (seven patients) to pregnancy (three patients). (Figure 1)The lesions were distributed on the breast (4 patients), buttock (3 patients), abdomen (2 patients) and the thigh. (Figure 2)There was a clinically appreciable improvement in striae ranging from 1 to 24%. (Table 1, 2,) Frequency distribution of patients with striae alba, classified according to the percentage of improvement from baseline are listed in table 1.
Figure 1 .
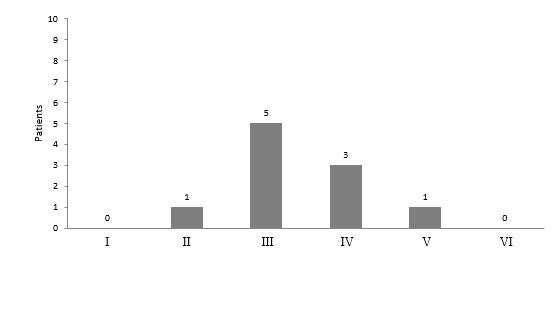
The frequency distribution of the Fitzpatrick skin type in patients
Figure 2 .
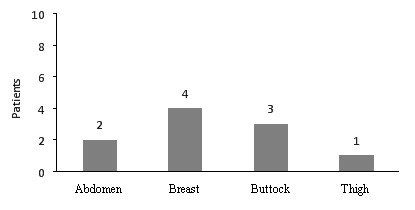
The frequency distribution of the lesions ‘location in patients
Table 1 . Frequency distribution of patients with striae alba, classified according to the percentage improvement from baseline .
| Improvement from baseline |
Week 4
(n=10) |
Week 8
(n=10) |
Week 12
(n=8) |
Week 16
(n=8) |
3 months after the end of therapy
(n=9) |
| No improvement | 6 | 3 | 3 | 2 | 2 |
| Poor | 4 | 6 | 5 | 6 | 5 |
| Fair | 0 | 1 | 0 | 0 | 2 |
| Good | 0 | 0 | 0 | 0 | 0 |
| Excellent | 0 | 0 | 0 | 0 | 0 |
*based on percentage improvement from baseline
Improvement of the treated area was graded as excellent with 95% to 100%, good with 65% to 94%, fair with 25% to 64% and poor with 1-24% improvement.
Table 2 . Descriptive statistics of percentage improvement of treated areas from baseline .
| Sessions | N | Min | Q1 | Median | Q2 | Max |
| Week 4 | 10 | 0 | 0 | 0 | 10 | 20 |
| Week 8 | 10 | 0 | 0 | 10 | 10 | 40 |
| Week 12 | 8 | 0 | 0 | 10 | 20 | 20 |
| Week 16 | 8 | 0 | 1.25 | 17.5 | 20 | 20 |
| 3 months after the end of therapy | 9 | 0 | 2.5 | 20 | 25 | 30 |
Q1, first quartile; Q2, second quartile
In addition, a significant improvement in striae between the 16-week treatment and the 4-week treatment was identified (P<0.0001). Three months after the final treatment, patients showed noticeable improvement in the striae, compared with baseline and also the 4-week treatment (P<0.048). (Figure 3) But there is no significant statistical differences between improvements at the 16-week treatment and the 3-month follow up (P<0.36). No significant adverse effect appeared, but in one patient with skin type V, mild post inflammatory hyperpigmentation was observed on buttock after the 8-week treatment. After 4 weeks of treatment, mild to moderate acne of the breast occurred in another patient with skin type of IV. (Figure 4) Two patients were lost to follow-up. It was because of weak result in one patient and traveling to other city in the other one.
Figure 3 .
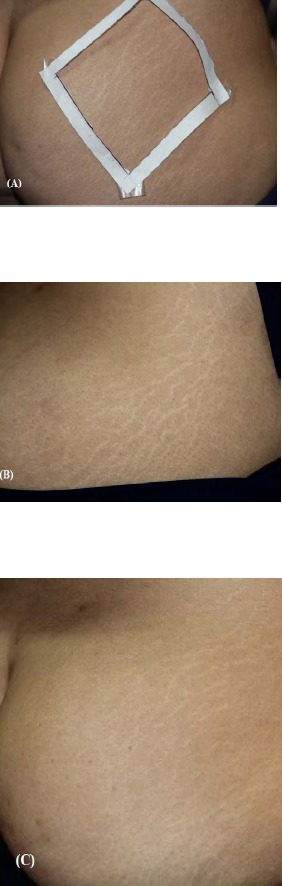
Striae Alba in a 28 years old women. (A). Before Treatments, (B) poor improvment (1-24%) after final treatment, and (C) fair improvment (25% to 64%) 3 months after last treatment.
Figure 4 .
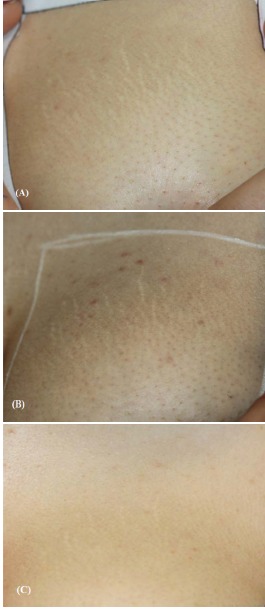
Striae Alba in a 39 years old women, (A) Before Treatments, (B) mild to moderate acne of the breast occurred after final treatment, (C) fair improvment (25% to 64%) 3 months after last treatment
Discussion
Treatment of striae distensae is challenging. Although there are some effective treatments for striae rubra such as topical 0.1% tretinoin cream2 and 585-nm pulsed dye laser, there is no useful modality for treatment of striae alba till now. 9,11 There are some studies which showed the relative efficacy of The 308-nm excimer laser that temporarily repigment the striae alba by increasing the number of melanocytes but without improving the atrophy.5 The non-ablative fractional 1540-nm laser has been shown to improve atrophic scars by increasing the amount of dermal collagen.13,14 It was approved by the FDA in February 2007 for skin resurfacing and dermatological procedures of soft tissue.5,12,15 . Star lux 500 is a particular laser for treatment of the striae alba, they are no studies, as far as we know, which evaluated the effect of laser on striae in the Asian patients with dark skin types. In our study the efficacy and safety of the Star lux 500 laser for Striae alba was evaluated. Among the 10 Iranian subjects enrolled in the study, a clinically and statistically improvement ranging from 1 to 24% was seen. Our patients had no adverse effect except mild post inflammatory hyperpigmentation in one case which occurred after the 8-week of treatment and mild to moderate acne in another patient after 4 weeks. Manuskiatt et al. showed the promising efficacy of Tri Pollar radiofrequency for treatment of striae distensae in seventeen patients. Patients received six weekly treatments. They were evaluated at baseline, 1 and 6 weeks after the final treatment. At 1-week evaluation, 38% of subjects showed 25-75% improvement in their striae. Also in 6-weeks follow-up, a higher improvement percentage was found. No side effects were reported.16 In Yang et al. study, 24 patients with varying degrees of atrophic striae alba in the abdomen were treated with 1550 nm fractional Erb:Glass laser and ablative fractional CO2 laser resurfacing. Each half of the abdominal lesion was randomly selected and treated three times for 4 weeks interval. Although they did not statistically differ, both treatments (nonablative fractional laser and ablative CO2 fractional laser) showed significant clinical and histopathologic improvement .17 In relation to this study, our study also showed the effectiveness of non-ablative laser for Striae improvement. De Angelis et al. conducted a study using fractional non ablative 1540-nm erbium:glass laser on 51 patients for both striae rubra and striae alba. They reported overall improvement as 50% or more for all patients at six months. In all patients during 18 to 24 months follow-up, there was no recurrence. The typical side effects that occurred included transient erythema and edema. Some patients experienced transient trace post inflammatory hyperpigmentation (PIH), which all resolved. Histological observations revealed thickening of the epidermis and dermis, neocollagenesis and increased elastin deposition one month after the last treatment.18 This study showed a higher rate of improvement than our study but the rate of PIH occurrence was also more in their patients.
According to our study, we found clinically and statistically improvement with no adverse effects. This may be a safe and effective treatment option for SD in Iranian patients. The major limitation of our study was the high cost of the laser therapy and because of this limitation, our cases were limited. Further clinical trials with larger sample size are recommended.
Please cite this article as follows:
Malekzad F, Shakoei S, Ayatollahi A, Hejazi S. The Safety and Efficacy of the 1540nm Non-Ablative Fractional XD Probe of Star Lux 500 Device in the Treatment of Striae Alba: Before-After Study. J Lasers Med Sci 2014;5(4):194-8
References
- 1.Alexiades-Armenakas MR, Bernstein LJ, Friedman PM, Geronemus RG. The safety and efficacy of the 308-nm excimer laser for pigment correction of hypo pigmented scars and striae Alba. Arch Dermatol. 2004;140:955–60. doi: 10.1001/archderm.140.8.955. [DOI] [PubMed] [Google Scholar]
- 2.Elsaie ML, Baumann LS, Elsaaiee LT. Striae distensae (stretch marks) and different modalities of therapy: an update. Dermatol Surg. 2009;35:563–73. doi: 10.1111/j.1524-4725.2009.01094.x. [DOI] [PubMed] [Google Scholar]
- 3.Tay YK, Kwok C, Tan E. Non ablative 1,450 nm diode laser treatment of striae distensae. Lasers Surg Med. 2006;38:196–99. doi: 10.1002/lsm.20281. [DOI] [PubMed] [Google Scholar]
- 4.Singh G, Kumar LP. Striae distensae. Indian J Dermatol Venereol Leprol. 2005;71(5):370–2. doi: 10.4103/0378-6323.16800. [DOI] [PubMed] [Google Scholar]
- 5.Ostovari N, Saadat N, Nasiri S, Moravvej H, Toossi P. The 308-nm excimer laser in the darkening of the white lines of striae alba. J Dermatolog Treat. 2010;21:229–31. doi: 10.3109/09546631003592044. [DOI] [PubMed] [Google Scholar]
- 6.Goldberg DJ, Sarradet D, Hussain M. 308-nm Excimer laser treatment of mature hypopigmented striae. Dermatol Surg. 2003;29:596–8. doi: 10.1046/j.1524-4725.2003.29144.x. [DOI] [PubMed] [Google Scholar]
- 7.Goel A, Krupashankar DS, Aurangabadkar S, Nischal KC, Omprakash HM, Mysore V. Fractional lasers in dermatology--current status and recommendations. Indian J Dermatol Venereol Leprol. 2011;77:369–79. doi: 10.4103/0378-6323.79732. [DOI] [PubMed] [Google Scholar]
- 8.Taub AF. Fractionated delivery systems for difficult to treat clinical applications: acne scarring, melisma, atrophic scarring, striae distensae, and deep rhytides. J Drugs Dermatol. 2007;6:1120–8. [PubMed] [Google Scholar]
- 9.Suh DH, Chang KY, Son HC, Ryu JH, Lee SJ, Song KY. Radiofrequency and 585-nmpulsed dye laser treatment of striaedistensae: a report of 37Asian patients. Dermatol Surg. 2007;33:29–34. doi: 10.1111/j.1524-4725.2007.33004.x. [DOI] [PubMed] [Google Scholar]
- 10.Kim BJ, Lee DH, Kim MN, Song KY, Cho WI, Lee CK, Kim JY, Kwon OS. Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol. 2008;9:33–7. doi: 10.2165/00128071-200809010-00003. [DOI] [PubMed] [Google Scholar]
- 11.Alexiades-Armenakas MR, Dover JS, Arndt KA. The spectrum of laser skin resurfacing: nonablative, fractional, and ablative laser resurfacing. J Am Acad Dermatol. 2008;58:719–37. doi: 10.1016/j.jaad.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 12.http://www.palomarmedical.com.
- 13.Hedelund L, Moreau KE, Beyer DM, Nymann P, Haedersdal M. Fractional nonablative 1,540-nm laser resurfacing of atrophic acne scarsA randomized controlled trial with blinded response evaluation. Lasers Med Sci. 2010;2:749–54. doi: 10.1007/s10103-010-0801-1. [DOI] [PubMed] [Google Scholar]
- 14.Sachdeva S. Nonablative fractional laser resurfacing in Asian skin--a review. J Cosmet Dermatol. 2010;9:307–12. doi: 10.1111/j.1473-2165.2010.00528.x. [DOI] [PubMed] [Google Scholar]
- 15.Moravvej H, Barikbin B, Ghavam S A, Karimi S. Nonablative Fractional Laser Resurfacing. Jf Lasers Med Sci. 2011;2:30–5. [Google Scholar]
- 16.Manuskiatti W, Boonthaweeyuwat E, Varothai S. Treatment of striaedistensae with a TriPollar radiofrequency device: A pilot study. J Dermatol Treat. 2009;20:359–64. doi: 10.3109/09546630903085278. [DOI] [PubMed] [Google Scholar]
- 17.You Jin Yang, Ga-Young Lee. Treatment of Striae Distensae with Nonablative Fractional Laser versus Ablative CO2 Fractional Laser: A Randomized Controlled Trial . Ann Dermatol. 2011;23:481–9. doi: 10.5021/ad.2011.23.4.481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.De Angelis F, Kolesnikova L, Renato F, Liguori G. Fractional nonablative 1540-nm laser treatment of striaedistensae in Fitzpatrick skin types II to IV: clinical and histological results. Aesthet Surg J. 2011;31:411–9. doi: 10.1177/1090820X11402493. [DOI] [PubMed] [Google Scholar]