

Abstract
Chronic stress is among the most common diagnoses in Sweden, most commonly in the form of exhaustion syndrome (ICD-10 classification – F43.8). The majority of patients with this syndrome also have disturbed breathing (hyperventilation). The aim of this study was to investigate the association between hyperventilation and exhaustion syndrome. Thirty patients with exhaustion syndrome and 14 healthy subjects were evaluated with the Nijmegen Symptom Questionnaire (NQ). The participants completed questionnaires about exhaustion, mental state, sleep disturbance, pain and quality of life. The evaluation was repeated 4 weeks later, after half of the patients and healthy subjects had engaged in a therapy method called ‘Grounding’, a physical exercise inspired by African dance. The patients reported significantly higher levels of hyperventilation as compared to the healthy subjects. All patients’ average score on NQ was 26.57 ± 10.98, while that of the healthy subjects was 15.14 ± 7.89 (t = −3.48, df = 42, p < 0.001). The NQ scores correlated strongly with two measures of exhaustion (Karolinska Exhaustion Scale KES r = 0.772, p < 0.01; Shirom Melamed Burnout Measure SMBM r = 0.565, p < 0.01), mental status [Hospital Anxiety and Depression Score (HADS) depression r = 0.414, p < 0.01; HADS anxiety r = 0.627, p < 0.01], sleep disturbances (r = −0.514, p < 0.01), pain (r = −.370, p < 0.05) and poor well-being (Medical Outcomes Survey Short Form 36 questionnaire- SR Health r = −0.529, p < 0.05). In the logistic regression analysis, the variance in the scores from NQ were explained to a high degree (R2 = 0.752) by scores in KES and HADS. The brief Grounding training contributed to a near significant reduction in hyperventilation (F = 2.521, p < 0.124) and to significant reductions in exhaustion scores and scores of depression and anxiety. The conclusion is that hyperventilation is common in exhaustion syndrome patients and that it can be reduced by systematic physical therapy such as Grounding.
Keywords: stress, burnout, hyperventilation
Introduction
Chronic stress is among the most common diagnoses for individuals on long-term sick leave in Sweden 1. Chronic stress can be seen as a process of deteriorating energetic resources 2,3. Severe stress symptoms occur if an imbalance between investing and regaining energy persists over a long period of time. Chronic stress symptoms usually occur within three areas: emotional exhaustion, physical tiredness and cognitive difficulties 3–6. Emotional exhaustion refers to having a lack of energy in social intercourse situations. Physical tiredness manifests itself in a feeling of tenseness as well as an inability to accomplish everyday tasks. Cognitive difficulties are characterised by decelerated cognitive processes and by memory and concentration problems. In Sweden, chronic stress symptoms leading to inability to work has been recognised by the National Board of Health and Welfare as ICD-10 medical diagnosis (exhaustion syndrome – F43.8) 7. The diagnosis and treatment of exhaustion syndrome has been a subject of numerous studies 8–10 in the last decade. In one of the first published treatment studies 11, we examined a group of 80 patients with exhaustion syndrome and exposed them to a treatment programme based on group cognitive behavioural therapy (CBT). Along with other health complaints, it was noted that the patients consistently complained about breathing problems. Although the relationship between disturbed breathing and stress response has been well studied 12, to our knowledge, there has not been a published study on the disturbed breathing that occurs in connection with exhaustion syndrome, nor have there been any accounts of attempts to systematically influence respiratory patterns in the treatment of patients with exhaustion syndrome. One potential method for such treatment comes from the tradition of body awareness training often used in Sweden as a part of physical therapy. The method is based on the observation that yoga respiration training (pranayama) stimulates the parasympathetic nervous system 13–15 and thus reduces sympathetically driven stress responses. It has also been found that the parasympathetic nervous system can be stimulated through dance and other mind–body interventions 14,16,17 and that these activities have a positive effect in the treatment of diseases caused by stress 18. Breathing practice exercises, as shown in another study, have brought about decreases in anxiety levels by re-establishing breathing patterns 19. One new method which may be used is based on the African dance called ‘Grounding’ and involves performing rhythmical movements while maintaining a balanced respiration 20. The founder of Grounding, Bedu Annan from Ghana, hypothesised that Grounding has positive physical and psychological effects on health. In Grounding, one systematically works on releasing tension throughout the whole body: in the feet, ankles, knees, pelvis, shoulders, arms, hands, neck and head. The rhythm in the movement flows; as energetic movement shifts into relaxed movement, tension is released and free breathing becomes easier. The accompanying stamping movements ensure good contact with the ground and give a feeling of stability.
The aim of the present study is to systematically study the role of disturbed breathing in patients with exhaustion syndrome and to explore the efficacy of utilising the African dance of Grounding as a type of short-term physical therapy for normalising their respiratory patterns.
The first hypothesis is that patients with exhaustion syndrome experience disturbed breathing, manifested mainly as hyperventilation, and that the severity of this dysfunction is related to the severity of their exhaustion syndrome.
The second hypothesis is that the respiratory patterns of patients with exhaustion syndrome patients can be normalised through short-term physical therapy based on Grounding and that such a normalisation will lead to a reduction of the symptoms of exhaustion.
Material and method
Participants and procedure
Consecutive patients referred to the Stress Clinic in Stockholm by primary care physicians and diagnosed as having work-related exhaustion syndrome (F43.8 diagnosis in the ICD-10 classification system) were asked to participate in the study before the regular treatment programme was initiated. Out of 45 patients invited to participate, 30 patients were enrolled (Table1). Following advertisement about participation in the study at the campus at Karolinska Institute, 17 healthy subjects expressed interest and 14 were included in the study. The patients were divided into control and intervention groups by placing the first eight consecutive patients into the control group and the next eight into the intervention group, and then, similarly, placing the next seven in the control group and the final seven into the intervention group.
Table 1.
Characteristics of patients with exhaustion syndrome and healthy subjects, n and mean ± SD
| Healthy subjects N = 14 | Patients | |||
|---|---|---|---|---|
| Total group N = 30 | Intervention group N = 15 | Control group N = 15 | ||
| Age (years) | 42.8 ± 4.1 | 44.2 ± 8.8 | 43.4 ± 6.2 | 45.0 ± 11.0 |
| BMI(kg/m2) | 21.9 ± 1.7 | 25.1 ± 4.1 | 24.3 ± 3.8 | 25.9 ± 4.3 |
| Smoking (n) | 0 | 0 | 0 | 0 |
Thus, the intervention group consisted of 15 patients (12 female and three male), the control group of 15 patients (12 female and three male) and the healthy group of 14 persons (12 female and two male). Participants were invited to an introductory group session in which the study programme was explained, questionnaires completed and monitoring equipment introduced (see below). The patients in the intervention group and the healthy subjects were asked to return twice a week for 4 weeks to participate in Grounding training sessions (1.5 hours each) conducted in groups of seven or eight participants. The intervention group met on Tuesdays and on Thursdays early in the afternoon; the healthy group met on Mondays and on Thursdays late in the afternoon. The grounding training was standardised for all the participating subjects. The physiotherapist, who led all the training sessions, was trained by a grounding/dance therapist 20. During the first and last week of training, physiological monitoring equipment was employed on the participants for a 2-day period while they engaged in their normal life activities. The results of the physiological tests will be reported separately. At the end of the training period, identical questionnaires were completed. The control patient group completed similar evaluations at the beginning and at the end of the 4-week period without undergoing any intervention attempts. The study was approved by the Ethics Committee at the Karolinska Institute, and written informed consent was received from each participant.
Grounding
Grounding is defined as a kind of physical exercise, involving free-swinging movements and sounds which originate from African dance 20. The founder's main philosophy was to move in a way that effectively makes use of a person's movement energy. In this study, the Grounding-based intervention was aimed at improving body awareness, breathing and relaxation.
The content of the programme gradually expanded over the 4-week intervention period, 1, 5 hours, twice a week. During the first week, the participants were taught to listen and move to the rhythm. Attention was then given to the contact between the feet and the ground as well as the position of the pelvis. During the second week, the participants began moving to music of the drums. During the third and fourth weeks, the participants tried out African ‘working movements’ to the sound of music and they also tried capturing pauses using African music of polyrhythmic character. This session was ended with stretching, body shaking and relaxation, lying on the floor, focusing on free flow of breathing. The group of patients and the control group of healthy persons both realised the same Grounding programme.
Measures
For each patient and healthy subject, demographic data and information about age, height, weight and smoking were assessed by a questionnaire (Table1).
Hyperventilation
Hyperventilation is defined as breathing in excess of metabolic requirements, in terms of CO2 production. It was first used by Kerr et al. 21 in 1938 to describe patients with somatic symptoms of both hypocapnia and anxiety. A majority of patients who experience hyperventilation, as measured with NQ, have a thoracic dominant breathing pattern 21, increased anxiety and a decreased quality of life 22.
Nijmegen Symptom Questionnaire
The Nijmegen Symptom Questionnaire (NQ) is used as a measure of hyperventilation 23. It is a quick and easy to administer assessment tool which assesses 16 symptoms associated with abnormal breathing on a 5-point ordinal scale (1 = never, 5 = very frequently). The symptoms relate to different systems: (i) cardiovascular, for example palpations; (ii) neurological, for example dizzy spells, tingling fingers; (iii) respiratory, for example shortness of breath; (iv) gastro-intestinal, for example bloated abdominal sensation; and (v) mental, for example tension. A score of 24/64 or more indicates a possible diagnosis of hyperventilation 24,25
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) measures mental health 26. The score range in HADS is 0–21; a higher score indicates poorer mental health.
Karolinska Exhaustion Scale
The Karolinska Exhaustion Scale (KES) has been constructed to provide specific assessments of exhaustion in clinical and research settings. It is a self-report pen-and-paper instrument based on the Swedish National Board of Health and Welfare's description of the diagnosis of the syndrome of exhaustion 27. The 41 items in KES, each graded from 1 (never) to 5 (always) comprise four inter-related dimensions: (i) lack of recovery, (ii) cognitive exhaustion, (iii) somatic symptoms and (iv) emotional distress. Lack of recovery contains items relating to excessive fatigue and perpetuated patterns of sleep and rest. The dimension of cognitive exhaustion contains items that are associated with problems with memory, concentration and coping with mental demands. The dimension of somatic symptoms assesses such physical sensations as headaches, palpitations, chest pain, muscular tension and pain. Finally, the dimension of emotional distress covers symptoms of irritability, depression and anxiety. Data can be presented as a total average or as an average of four subscales.
Karolinska Sleepiness Scale
Sleep disturbances were examined through an eight-question index (graded 1–5) taken from the Karolinska Sleep Questionnaire (KSQ; e.g., I have difficulties falling asleep; I do not feel well-rested when I wake up in the morning; I experience disturbed sleep; 28). The Cronbach's α coefficient was 0.71.
Shirom Melamed Burnout Measure
The measures in the study included the Shirom Melamed Burnout Measure (SMBM), which is designed to measure chronic stress according to perceived stress symptoms. The SMBM contains 22 items (graded 1–7) that measure different facets of chronic stress by focusing on the depletion of an individual's energetic resources 4. The respondents rate how much physical, emotional and psychological stress symptoms they experience 29. High scores indicate an intense experiencing of stress symptoms. In this study, as in previous studies, a rating of four or above was considered to be indicative of serious stress symptoms 30. The Cronbach's α coefficient was 0.93 at time 1 and 0.94 at time 2.
Medical Outcomes Survey Short Form 36 questionnaire
The Medical Outcomes Survey Short Form 36 questionnaire (SF-36) 31 is a multipurpose, short-form health survey with 36 questions. It yields an 8-scale profile of functional health and well-being scores, psychometrically based physical and mental health summary measures and a preference-based health unity index. For the present study, we have chosen to use item 1 ‘Your health is’ (1 = excellent, 5 = bad).
Pain
Pain intensity was rated on a 0–100 mm visual analogue scale (VAS). Zero was defined as ‘no pain’ and 100 as ‘the worst imaginable pain.’ Pain location was also shown on a pain drawing, indicating particular pain areas 32
Data analysis
In a first step, the data were explored by means of descriptive statistics as the correlations between variables were tested with the Spearman's correlation coefficient, and t-tests between patients and healthy group data were conducted. In a second step, to answer the research questions, an analysis of variance and a logistic regression analysis were conducted. To test the treatment effect, anova for repeated measures was conducted. The statistical analyses were carried out using the Statistical Package for Social Sciences (spss) version 19.0 for Macintosh (IBM Corp., Armonk, NY, USA). A p < 0.05 was considered significant, while a p < 0.1 was considered a trend for significance.
Results
During the initial evaluation of the participants' respiration, the patient group scored significantly higher than the healthy subjects on the NQ, indicating hyperventilation syndrome (Table2). The patients’ average score was 26.57, while that of the healthy subjects was 15.14 (t = −3.48, df = 42, p < 0.001). In the patient group, 19/30 scored ≥24, indicating hyperventilation, while 3/14 of the healthy subjects had such scores. After the Grounding intervention, there was a slight but nonsignificant decrease in hyperventilation in the patient group who had received intervention, whereas there was no change in the patient control group (Table2).
Table 2.
Hyperventilation in healthy subjects and patients, mean ± SD
| Before Intervention | After Intervention | p-value | |
|---|---|---|---|
| Healthy subjects n = 14 | 15.14 ± 7.89 | 14.07 ± 9.38 | 0.396 |
| Intervention patient group n = 15 | 26.67 ± 12.05 | 24.73 ± 9.01 | 0.232 |
| Patient control group n = 15 | 25.78 ± 10.27 | 27.92 ± 10.07 | 0.251 |
At baseline, when both patients and healthy subjects were combined in one group (n = 44), highly significant correlations were found between the NQ scores and a number of measures: two measures of exhaustion (KUS r = 0.772, p < 0.001; SMBM r = 0.565, p < 0.01; Fig.1), mental status (HADS depression r = 0.414, p < 0.001; HADS anxiety r = 0.627, p < 0.01), sleep disturbances (r = −0.514, p < 0.01), pain (r = −0.370, p < 0.05) and well-being (SF-36, health r = −0.529, p < 0.05). Similarly strong correlations were observed within the patient and healthy groups. The same pattern of correlation appeared after the intervention 4 weeks later.
Figure 1.
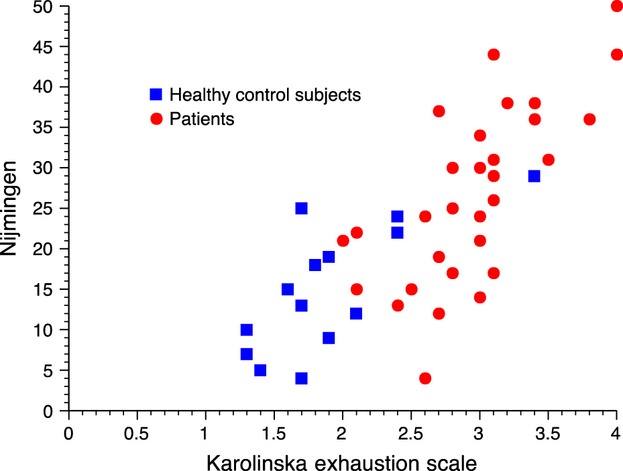
Correlation between hyperventilation (Nijmingen Symptoms Questionnaire) and exhaustion (Karolinska Exhaustion Syndrome) in a group of patients with exhaustion syndrome (n = 30) as well as a group of healthy control subjects (n = 14).
To study which factors best predict hyperventilation syndrome, a linear stepwise regression analysis was conducted with all factors included. The NQ scores were best predicted by KES (B = 13.690, p = 0.001), HADS depression (B = −1.058, p = 0.021), and HADS anxiety (B = 0.937, p = 0.013; Table3). The R2 was high and significant (R2 = 0.752). Neither sleep disturbances nor measures of quality of life contributed further to the variance in hyperventilation syndrome.
Table 3.
Predicting level of hyperventilation syndrome scores (Nijmegen Symptoms Questionnaire) by means of a stepwise regression analysis
| Model | Unstandardised Coefficients | Standardised Coefficients | t | Significance | 95% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|
| B | SE | Beta | Lower Bound | Upper Bound | |||
| (Constant) | −10.865 | 36.326 | −0.299 | 0.767 | −85.052 | 63.323 | |
| KES | 13.690 | 3.564 | .863 | 3.841 | 0.001 | 6.412 | 20.968 |
| Age | .035 | .169 | .023 | 0.209 | 0.835 | −0.309 | 0.380 |
| Weight | −.053 | .120 | −.054 | −0.440 | 0.663 | −0.298 | 0.192 |
| Height | .050 | .194 | .036 | 0.256 | 0.800 | −0.347 | 0.446 |
| HAD Depression | −1.058 | .436 | −.429 | −2.426 | 0.021 | −1.948 | −0.167 |
| HAD Anxiety | 0.937 | 0.353 | 0.394 | −2.655 | 0.013 | 0.216 | 1.657 |
| SMBM | −0.700 | 1.731 | −0.091 | −0.404 | 0.689 | −4.234 | 2.834 |
| Sleep | 0.127 | 2.781 | 0.008 | 0.046 | 0.964 | −5.553 | 5.807 |
| SR 36 Well-being | −0.207 | 1.365 | −0.019 | −0.152 | 0.880 | −2.995 | 2.580 |
| Pain | −0.405 | 0.590 | −0.085 | −0.687 | 0.498 | −1.611 | 0.800 |
The evaluation of the intervention
The brief Grounding intervention was intended to reduce hyperventilation syndrome, reduce exhaustion syndrome, improve mental state and improve quality of life. In the patient intervention group, hyperventilation syndrome scores were lower at follow-up, as compared to the patient control group (Table4), but this difference did not reach significance. Statistically significant changes in level of exhaustion syndrome (KES and SMBM) and level of depression and anxiety (HADS) were also observed. No statistically significant changes between the intervention and control groups were observed in the level of sleep complaints, pain or quality of life measurements.
Table 4.
Changes observed between the initial measurement and the 5-week follow-up, a period in which the intervention patient group which received weekly Grounding training, and patient control group without training, mean ± SD
| Intervention N = 15 | Control N = 15 | F ratios | ||
|---|---|---|---|---|
| Time (nano seconds) | Time × Groups | |||
| Hyperventilation syndrome | ||||
| Before | 26.67 ± 12.05 | 25.78 ± 10.27 | 0.007 | 2.521 (p < 0.124) |
| After | 24.73 ± 9.01 | 27.92 ± 10.07 | ||
| KES | ||||
| Before | 3.09 ± 0.42 | 2.85 ± 0.54 | 3.14 (p < 0.089) | 12.05 (p < 0.002) |
| After | 2.87 ± .51 | 3.05 ± 1.08 | ||
| SMBM | ||||
| Before | 5.17 ± 1.01 | 4.52 ± 1.0 | 0.28 | 13.67 (p < 0.001) |
| After | 4.55 ± .67 | 5.08 ± 1.09 | ||
| HAD depression | ||||
| Before | 9.53 ± 2.99 | 9.00 ± 4.72 | 2.26 (p < 0.145) | 3.32 (p < 0.080) |
| After | 9.33 ± 3.22 | 11.08 ± 5.87 | ||
| HAD anxiety | ||||
| Before | 10.53 ± 4.40 | 9.83 ± 3.47 | 0.179 | 3.36 (p < 0.079) |
| After | 8.93 ± 3.47 | 10.83 ± 4.15 | ||
| Sleep quality | ||||
| Before | 2.87 ± 0.586 | 2.78 ± 0.673 | 1.736 (p < 0.200) | 0.24 ns |
| After | 2.93 ± 0.630 | 2.90 ± 0.664 | ||
| Pain | ||||
| Before | 4.9 ± 2.43 | 4.15 ± 2.22 | 0.074 | 0.06 ns |
| After | 4.6 ± 2.42 | 4.67 ± 2.21 | ||
| SF 36 well-being | ||||
| Before | 3.6 ± 0.82 | 3.67 ± 0.65 | 0.015 | 1.86 (p < 0.105 |
| After | 3.4 ± 0.63 | 3.83 ± 0.58 | ||
Hyperventilation syndrome according to Nijmegen Symptoms Questionnaire; Karolinska Exhaustion Scale (KES); Shirom Melamed Burnout Measure (SMBM); Hospital anxiety and Depression (HAD); 36-Item Short-Form Health Survey (SF 36).
Discussion
The present study found significantly disturbed breathing patterns among patients with work-related exhaustion syndrome, as compared to healthy subjects. Of the conditions tested for, hyperventilation syndrome, as assessed by the NQ, was most prominent among the patients. The severity of their hyperventilation syndrome was highly correlated with levels of exhaustion, depression, anxiety, sleep disturbances and quality of life. The present study also demonstrated that a short-term physical therapy intervention based on Grounding may have a potentially ameliorating effect on the hyperventilation syndrome of exhausted patients, as well as on their experiencing of exhaustion, anxiety and depression.
To our knowledge, this severe disturbance of breathing in patients with exhaustion syndrome has not been reported before. There are many reasons why normal breathing can become negatively affected, including biochemical-, biomechanical- or psychological-based disorders 33. Conscious or unconscious changes in breathing can affect both our feelings and thoughts, and emotions and feelings of anger, fear and anxiety can increase our breathing 33. Biomechanical aspects of breathing influence its functionality and patients with unexplained breathing symptoms, such as dyspnoea, often show abnormalities in breathing pattern 34,35. Alterations in the performance of the respiratory muscles may reduce the effectiveness of ventilation. Subjects who suffer from hyperventilation syndrome often show a predominantly upper chest breathing pattern at rest. It has been proposed that the abdominal afferent proprioceptive input associated with such breathing can directly result in the perception of respiratory symptoms 19. Unpleasant sensations can arise in the intercostals and other breathing muscles due to prolonged upper chest breathing, and the sensations may become even worse if the subject is stressed. Thus, it is not surprising that patients with exhaustion syndrome and increased levels of anxiety show higher levels of hyperventilation compared to healthy controls. The present results are strengthened by results from Hagman et al. 34 whose patients with nondiagnosed dysfunctional breathing problems scored similarly to the patients in the present study on the NQ. In addition, the control subjects in the study by Hagman et al. had the same level of hyperventilation as the healthy subjects in the present study. In our study, 63% (19/30) of the patients and 2% (3/14) of the healthy subjects had scores indicating hyperventilation (≥24). This is in accordance with Thomas et al. 35 who estimated the prevalence of dysfunctional breathing in an adult population, as measured by the NQ in a cross-sectional postal survey and found it to be 9.5%.
In this study, the level of respiratory disturbance was highly correlated with the level of exhaustion as well as with depression and anxiety scores, sleep disturbances and low quality of life. This result is in accordance with other researchers reporting that patients with dysfunctional breathing have a lower level of quality of life and are more anxious and depressed 34. Our breathing can be under automatic or voluntary control 36,37. This dual nature of breathing gives us great power but can also involve risks and problems 36,38, as breathing is an activity on which our physiological and our psychological being depend. Most of the time, we are unaware of breathing, but as soon as something physical or psychological causes breathing to change, it immediately impinges on our sense of well-being. The discomfort it carries with it can bring on a range of sensations, such as becoming emotionally upset – which can indirectly disrupt physical functions in the body 36. For example, excessive breathing with an upper chest breathing pattern can be triggered by a stressful situation associated with fear, anger or anxiety. This breathing pattern can generate unpleasant sensations such as dyspnoea, pain or tightness in the chest 36.
In the present study, changes in the level of hyperventilation syndrome between two study points were accompanied by similar changes in the level of exhaustion syndrome, mental state and quality of life, which further points to the strong relationship between respiration and exhaustion due to work stress.
The intervention in this study comprised Grounding, a kind of physical exercise. At present, there is no standardised treatment for patients with hyperventilation syndrome. Previous studies of patients experiencing hyperventilation or dysfunctional breathing have reported positive results after a period of breathing retraining 33,39–41. Also, improvements in coping with stressful situations 33,41, reduction in somatic complaints 33,40,41 and lower anxiety levels 33,41 have been reported. A 3-year follow-up study of patients with functional cardiac symptoms related to hyperventilation reported that the patients were less prone to future respiratory deregulation and subsequent cardiac symptoms after they had been trained in diaphragmatic breathing 40.
In treating asthma, breathing retraining has involved both informational and practical components, although the modification of breathing patterns is the most central component in most programmes 42.
In this study, we assessed the participants' breathing problems using the NQ, a measure of hyperventilation. Although there is a lack of consensus on the definition and best methods for evaluating breathing problems 39,43, the NQ is widely accepted and was deemed to be appropriate for our purposes.
There are some limitations in this study. Due to a large variability in the NQ scores, the difference between the intervention and control groups in the present study was only marginally significant. This problem could be remedied in the future by using a much larger sample size.
Thus, the conclusion of the study is that hyperventilation is common in exhaustion syndrome patients and that it can potentially be reduced through systematic physical therapy such as Grounding.
Author contributions
Heli Ristiniemi designed research/study, performed research/study, collected data, analysed data and wrote the paper. Aleksander Perski designed research/study, analysed data, contributed with important comments and wrote the paper. Eugene Lyskov contributed with important comments. Margareta Emtner designed research/study, analysed data, contributed with important comments and wrote the paper.
Ethical approval
The study was approved by the Ethics Committee at the Karolinska Institute, and written informed consent was received from each participant.
Funding
The study was supported by a generous grant from Foundation Stress Mottagningen, Stockholm, Sweden.
References
- Swedish National Social Insurance Board. 2012. http://www.fk.se (last accessed 15 September 2012)
- Shaufeli WB, Leiter MP, Maslach C. Burnout: thirty-five years of research and practice. Career Dev Int. 2009;14:204–20. [Google Scholar]
- Shirom A. Job-related burnout. In: Quick JC, Tetrick LE, editors. Handbook of Occupational Health Psychology. Washington, DC: American Psychological Association; 2003. pp. 245–65. [Google Scholar]
- Melamed S, Kushnir T, Shirom A. Burnout and risk-factors for cardiovascular diseases. Behav Med. 1992;18:53–60. doi: 10.1080/08964289.1992.9935172. [DOI] [PubMed] [Google Scholar]
- Melamed S, Shirom A, Toker S, Berliner S, Shapira I. Burnout and risk of cardiovascular disease: evidence, possible causal paths, and promising research directions. Psychol Bull. 2006;132:327–53. doi: 10.1037/0033-2909.132.3.327. [DOI] [PubMed] [Google Scholar]
- Schaufeli W, Enzmann D. The Burnout Companion to Study and Practice: A Critical Analysis. London: Taylor&Francis; 1998. [Google Scholar]
- Socialstyrelsen. Utmattningssyndrom– Stressrelaterad Psykisk Ohälsa. Stockholm: Bjurner & Bruno AB; 2003. (Exhaustion syndrome -Stress related mental health problems) [Google Scholar]
- Peterson U, Bergström G, Demerouti E, Gustavsson P, Asberg M, Nygren A. Burnout levels and self-rated health prospectively predict future long-term sickness absence: a study among female health professionals. J Occup Environ Med. 2011;53:788–93. doi: 10.1097/JOM.0b013e318222b1dc. [DOI] [PubMed] [Google Scholar]
- Stenlund T, Birgander LS, Lindahl B, Nilsson L, Ahlgren C. Effects of Qigong in patients with burnout: a randomized controlled trial. J Rehabil Med. 2009;41:761–7. doi: 10.2340/16501977-0417. [DOI] [PubMed] [Google Scholar]
- Peterson U, Bergström G, Samuelsson M, Asberg M, Nygren A. Reflecting. Peer-support groups in the prevention of stress and burnout: randomized controlled trial. J Adv Nurs. 2008;63:506–16. doi: 10.1111/j.1365-2648.2008.04743.x. [DOI] [PubMed] [Google Scholar]
- Perski A, Grossi G. Behandling av långtidssjukskrivna patienter med stressdiagnoser – Resultat från en interventionsstudie (Treatment of patients on long-term sick leave because of stress-related problems. Results from an intervention study) Läkartidningen. 2004;14:1295–8. [PubMed] [Google Scholar]
- Schleifer LM, Ley R, Spalding TW. A hyperventilation theory of job stress and musculoskeletal disorders. Am J Ind Med. 2002;41:420–32. doi: 10.1002/ajim.10061. [DOI] [PubMed] [Google Scholar]
- Brown RP, Gerbarg PL. Yoga breathing, meditation and longevity. Ann N Y Acad Sci. 2009;1172:54–62. doi: 10.1111/j.1749-6632.2009.04394.x. [DOI] [PubMed] [Google Scholar]
- West J, Otte C, Geher K, Johnson J, Mohr D. Effects of hatha yoga and african dance on perceived stress, affect, and salivary cortisol. Behav Med. 2004;28:114–8. doi: 10.1207/s15324796abm2802_6. [DOI] [PubMed] [Google Scholar]
- Brown RP, Gerbarg PL. Sudarshan Kriya Yoga breathing in the treatment of stress, anxiety, and depression: part II-clinical applications and guidelines. J Altern Complement Med. 2005;11:711–7. doi: 10.1089/acm.2005.11.711. [DOI] [PubMed] [Google Scholar]
- Lane AM, Lovejoy DJ. The effects of exercise on mood changes: the moderating effect of depressed mood. J Sports Med Phys Fitness. 2001;41:539–45. [PubMed] [Google Scholar]
- Bartholomew LB, Miller BM. Affective responses to an aerobic dance class: the impact of perceived performance. Res Q Exerc Sport. 2002;73:301–309. doi: 10.1080/02701367.2002.10609024. [DOI] [PubMed] [Google Scholar]
- Jacobs GD. Clinical applications of the relaxation response and mind-body interventions. J Altern Complement Med. 2001;7(Suppl 1):S93–101. doi: 10.1089/107555301753393850. [DOI] [PubMed] [Google Scholar]
- Tweeddale PM, Rowbottom I, McHardy GJR. Breathing retraining: effect on anxiety and depression scores in behavioural breathlessness. J Psychosom Res. 1994;38:11–21. doi: 10.1016/0022-3999(94)90004-3. [DOI] [PubMed] [Google Scholar]
- Annette Liljefors. Grounding. 2012. September, Google http://www.grounding.dinstudie.se (last accessed 15 September 2012)
- Kerr WJ, Gliebe PA, Dalton JW. Physical phenomena associated with anxiety states: the hyperventilation syndrome. Cal West Med. 1938;48:12–16. [PMC free article] [PubMed] [Google Scholar]
- Garcia G. Hyperventilation syndrome. Rev Prat. 2011;61:456–9. [PubMed] [Google Scholar]
- Van Doorn P, Colla P, Folgering H. Een vragenlijst voor hyperventilatieklachten. De Psycholoog. 1983;18:573–7. [Google Scholar]
- Van Dixhoorn J, Duivenvoorde H. Efficacy of Nijmegen questionnaire in recognition of the hyperventilation syndrome. J Psychosom Res. 1985;29:199–206. doi: 10.1016/0022-3999(85)90042-x. [DOI] [PubMed] [Google Scholar]
- Vansteenkiste J, Rochette F, Demedts M. Diagnostic tests of hyperventilation syndrome. Eur Respir J. 1991;4:393–9. [PubMed] [Google Scholar]
- Zigmond A, Snaith R. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- Saboonchi F, Perski A, Grossi G. Validation of Karolinska Exhaustion Scale: psychometric properties of a measure of exhaustion syndrome. Scand J Caring Sci. 2012 doi: 10.1111/j.1471-6712.2012.01089.x. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- Kecklund G, Åkerstedt T. The psychometric properties of the Karolinska Sleep Questionnaire. J Sleep Res. 1992;6:221–9. [Google Scholar]
- Shirom A, Melamed S. A comparison of the construct validity of two burnout measures in two groups of professionals. Int J Stress Manag. 2006;13:176–200. [Google Scholar]
- Grossi G, Perski A, Blomkvist V, Evengård B, Orth-Gomér K. Physiological correlates of burnout among women. J Psychosom Res. 2003;55:309–16. doi: 10.1016/s0022-3999(02)00633-5. [DOI] [PubMed] [Google Scholar]
- Ware J, Scherbourne C. The MOS 36-Item Short-Form Health Survey (SF-36): conceptual framework and item selection. Med Care. 1992;30:473–83. [PubMed] [Google Scholar]
- Huskison EC. Measurement of pain. Lancet. 1974;2:1127–31. doi: 10.1016/s0140-6736(74)90884-8. [DOI] [PubMed] [Google Scholar]
- Gershon R, Barocas B, Canton A, Li X, Vlahov D. Mental, physical, and behavioral outcomes associated with perceived work stress in police officers. Crim Justice Behav. 2009;36:275–89. [Google Scholar]
- Hagman C, Janson C, Emtner M. A comparison between patients with dysfunctional breathing and patients with asthma. Clin Res J. 2008;2:86–91. doi: 10.1111/j.1752-699X.2007.00036.x. [DOI] [PubMed] [Google Scholar]
- Thomas M, McKinley RK, Freeman E, Foy C, Prodger P, Price D. Breathing retraining for dysfunctional breathing in asthma: a randomised controlled trial. Thorax. 2003;58:110–5. doi: 10.1136/thorax.58.2.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilbert C. Breathing and the cardiovascular system. J Bodyw Mov Ther. 1999;3:215–24. [Google Scholar]
- Butler JE. Drive to the human respiratory muscles. Respir Physiol Neurobiol. 2007;159:115–26. doi: 10.1016/j.resp.2007.06.006. [DOI] [PubMed] [Google Scholar]
- Gilbert C. Hyperventilation and the body. Accid Emerg Nurs. 1999;7:130–40. doi: 10.1016/s0965-2302(99)80072-1. [DOI] [PubMed] [Google Scholar]
- Courtney R, Greenwood KM, Cohen M. Relationships between measures of dysfunctional breathing in a population with concerns about their breathing. J Bodyw Mov Ther. 2011;15:24–34. doi: 10.1016/j.jbmt.2010.06.004. [DOI] [PubMed] [Google Scholar]
- DeGuire S, Gevirtz R, Hawkinson D, Dixon K. Breathing retraining: a three-year follow-up study of treatment for hyperventilation syndrome and associated functional cardiac symptoms. Biofeedback Self Regul. 1996;21:191–8. doi: 10.1007/BF02284695. [DOI] [PubMed] [Google Scholar]
- Han JN, Stegen K, De Valck C, Clement J, Van de Woestijne KP. Influence of breathing therapy on complaints, anxiety and breathing pattern in patients with hyperventilation syndrome and anxiety disorders. J Psychosom Res. 1996;41:481–93. doi: 10.1016/s0022-3999(96)00220-6. [DOI] [PubMed] [Google Scholar]
- Bruton A, Thomas M. The role of breathing training in asthma management. Curr Opin Allergy Clin Immunol. 2011;11:53–57. doi: 10.1097/ACI.0b013e3283423085. [DOI] [PubMed] [Google Scholar]
- Van Dixhoorn J. Hyperventilation and dysfunctional breathing. Biol Psychol. 1997;46:90–91. [Google Scholar]